General information
Homocysteine is a product of the metabolism of cysteine and methionine. Its metabolism requires folic acid, B6 and B12. If they are deficient, the level of Homocysteine may increase. An excess of this substance leads to the development of serious health problems. Blood clots and damage to vessel walls may occur. Blood test for homocysteine
is often used to determine the likelihood of cardiovascular pathologies, but its value in this regard is questionable. Studies have found that replenishing folic acid and vitamin deficiencies does not reduce the risk of disease.
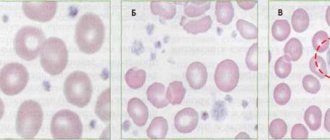
A sharp increase in indicators is often observed with homocysteinuria. This is a genetic disease in which there is a defect in the enzyme that prevents the breakdown of methionine. Amino acids accumulate in the body. A newborn with this disease is visually no different from healthy babies. Violations appear only after a few years. Children with this disease are thin and tall, and have thin fingers. They develop skeletal abnormalities, develop osteoporosis, and may develop early cardiovascular diseases.
HOMOCYSTEINE IS AN AMINO ACID THAT DAMAGES VESSELS
Earlier we talked about how excess salt and sugar consumption is a factor that threatens our blood vessels. Today we will talk about the amino acid homocysteine, since many do not even suspect what danger this amino acid can pose.
What is HOMOCYSTEINE?
To begin with, let us remind you that proteins consist of amino acids, which in turn are divided into non-essential (synthesized in the body) and essential (not synthesized in the body). So, homocysteine —
an amino acid that does not come with food, but is synthesized in the cells of the body, i.e. refers to replaceable. Further, homocysteine, under the influence of B vitamins and folic acid, is converted into harmless substances necessary for the body.
Why is a high level of HOMOCYSTEINE in the blood dangerous?
- Damages the inner wall of blood vessels, which in turn leads to the formation of cholesterol plaques in places of damage
- Activates the blood coagulation system and leads to the development of atherosclerosis, arterial and venous thrombosis, which can lead to heart attack or stroke
- During pregnancy, lead to gross malformations of the fetal nervous system
- Increases the risk of miscarriage
What can cause an increase in homocesteine levels?
- Deficiency of folate and B vitamins (B6, B12 and B1)
- Excessive coffee consumption (more than 4-5 cups per day)
- Kidney dysfunction
- Enzymopathies
Who is at risk?
- Pregnant women with previous obstetric complications
- Persons with a history of arterial/venous thrombosis, coronary heart disease
- Women under 50 years of age whose relatives have had strokes, heart attacks or thrombosis
- Smoking
- People leading a sedentary lifestyle (obese)
- Chronic alcohol abusers
How to prevent elevated homocysteine levels?
- Monitor the level of B vitamins and folic acid in the body.
- Moderately consume foods that contain methionine, from which homocysteine is synthesized (meat, cheese, cottage cheese, eggs).
- More often include in your diet foods sources of omega-3 fatty acids and B vitamins (fatty fish, walnuts, flax seeds/oil, oatmeal, greens, beef liver)
- Lead an active lifestyle (regular moderate physical activity).
- Do not abuse coffee and alcohol
- Stop smoking
Homocysteine norms for adults!
The average homocysteine level in the blood is no more than 10 µmol/l.
For pregnant women and those planning pregnancy - less than 8 µmol/l (in the 2nd-3rd trimester no more than 4-6 µmol/l).
Increase from 10 to 20
µmol/l
- mild,
from 20 to 29 - moderate,
from 30 and above – severe.
Remember!
High levels of homocysteine are not felt or shown in any way, so people at risk are advised to check their levels periodically.
Interpretation of results
Reference values vary depending on age. To correctly interpret the results, you must consult a doctor; self-diagnosis is unacceptable. Elevated levels of homocysteine may indicate a deficiency of B vitamins, kidney failure, diabetes, psoriasis, senile dementia, and pregnancy complications. They can also be elevated due to malnutrition. Significantly elevated levels in a newborn indicate homocysteinuria. To confirm this diagnosis, additional examination is required. Amino acid deficiency is observed in Down syndrome and hyperthyroidism.
The test results may be affected by long-term use of a number of medications, so you should inform your doctor if you are taking any medications.
Diagnosis of hyperhomocysteinemia
To diagnose hyperhomocysteinemia, the level of homocysteine in the blood is determined. Sometimes methionine loading tests are used (determining the level of homocysteine on an empty stomach and after a methionine load). If high levels of homocysteine in the blood are detected, tests must be performed to detect other risk factors for the development of vascular and obstetric complications. A test for homocysteine content can be carried out as a screening in practically healthy individuals to identify a group at increased risk of developing cardiovascular diseases and carry out preventive measures to reduce this risk. Homocysteine analysis is useful in diabetes mellitus with its tendency to vascular complications. Given the seriousness of the possible consequences of hyperhomocysteinemia during pregnancy, it is recommended that all women preparing for pregnancy have their homocysteine levels checked. It is mandatory to determine the level of homocysteine in patients with previous obstetric complications and in women whose relatives had strokes, heart attacks and thrombosis before the age of 45-50 years.
Stomach ulcer, steatosis, high homocysteine and LDL, intestinal problems
Michael
281 views
August 30, 2020
Good afternoon Help me understand the bunch of symptoms/tests and what to do next. Symptoms: severe fatigue for several months, severe daytime sleepiness, irritability, muscle aches, dizziness, occasional increases in blood pressure (no more than one hour), panic attacks, a feeling of lack of oxygen in the brain, sometimes dizziness and fog, lethargy, difficulty concentrating , sometimes pain in the legs in the calf area (as if it hurts inside the leg), heaviness in the right side, “sore eyes”, swelling of the face, cases of insomnia, spasms in the muscles of the neck and middle back, red spots on the face under the eyes and between the eyes and on the front edge of the hairline, flatulence with the smell of rot, bloating, periodically loose stools. Research/analysis: 08/12/2020 Ultrasound of the abdominal organs: echographic signs of diffuse changes in the liver parenchyma, probably of the type of fatty degeneration, chronic pancreatitis. The liver is enlarged due to both lobes: right lobe VR 177 mm, left lobe 0 thickness 80 mm, VR 109 mm 08/13/2020 Esophagogastroduodenoscopy: Diffuse non-atrophic gastritis. Multiple acute erosions and 2 acute gastric ulcers. Cicatricial deformity of the duodenal bulb (ulcer cured in 2009). Bulbit. The rapid test for HP is positive. 08/14/2020 Consultation with a gastroenterologist: De-nol 120 mg, 2t-2r, 50 minutes before meals, 4 weeks. Pariet 20 mg, 1t-2r, in 30 minutes. before meals, 4 weeks. Duspatalin 200 mg. 1t-2r, 30 minutes before meals, 14 days Helinorm 1k-1r, during meals, 4 weeks. Consultation with a cardiologist: CVD risk factors: increased cholesterol and LDL, decreased HDL (dyslipidemia 2A) Duplex scanning of the brachiocephalic arteries: Moderate atherosclerotic changes in the brachiocephalic arteries without signs of stenosis. Moderately pronounced non-straightness of the internal carotid artery on the left. Fibroelastometry of the liver: No fibrosis, grade 1 steatosis (251 dB/m) Fecal tests (I present only those where there are deviations): Yeast fungi - detected Muscle fibers with blackening - a little Reaction to occult blood - detected (but hemoglobin and haptoglobin - not detected) Intracellular starch - a little Extracellular starch - a little Lactose-negative Escherichia coli 10*6 Hemolyzing Escherichia coli 10*8 Klebsiella 10*6 Staphylococcus aureus 10*4 Clostridia 10*6 Blood tests (I write only those where there are deviations): Homocysteine 13.9 Estradiol 45.89 Total cholesterol 5.60 ALT 53.2 LDL cholesterol 4.02 HDL cholesterol 0.82 Gamma GT 79 Hematocrit 50.8 Platelets 410 Average platelet volume 11.3 Platelet crit 0.47 Basophils 0.11 Basophils % 1.1 Lymph oocytes 3.82 Lymphocytes% 39.6 Reticulocytes 96.3 Gastroscopy done 2 weeks after onset treatment of ulcers showed good dynamics, therefore, based on blood and stool tests, the following medications were added to the treatment: Terbinafine 250 mg. 1t-1r, 10 days Alpha-normix, 2t-2r, 10 days Heptral 400 mg, 1t-2r, 14 days The general condition has improved little, severe fatigue, drowsiness and all the symptoms indicated at the very beginning remain. The ulcer has begun to heal, the liver (it seems) as a whole is relatively normal, but the foul flatulence and bloating have not disappeared, dizziness and fogginess remain. Where should I go now? What might my tests indicate? I read about high bad cholesterol and homocysteine - it became scary)) Tell me what to do next? Which doctor should I go to? Hematologist? PS There is also an MRI of the entire spine from October 2021 - osteochondrosis, protrusions, spondyloarthrosis of the thoracic and lumbosacral regions.
The question is closed
analysis
liver
stool tests
What is homocysteine
Amino acids are the molecules that make up proteins.
There are about 500 different amino acids in the world, but only 22 are used to build all the proteins necessary for various organisms. Such amino acids are called proteinogenic. All other amino acids are formed as intermediate products of certain reactions. Homocysteine is an intermediate product of the metabolism of the proteinogenic amino acids methionine and cysteine. It does not enter the body with food, but is formed from methionine during reactions necessary for the normal functioning of our body. The resulting homocysteine can either be converted back into methionine or into another important amino acid, cysteine. These reactions occur thanks to enzymes, the adequate functioning of which requires vitamins B6, B12, as well as folic acid.
Thus, methionine, homocysteine, cysteine, some enzymes, as well as vitamins B6, B12 and folic acid are participants in the same process. Changes in the functioning of these components can lead to an increase in homocysteine.
Folate cycle genes: where is the myth and where is the reality?
How to control homocysteine levels
- Introduce into the diet foods containing vitamins B6, B12, folic acid;
- All women of reproductive age should consume a daily dosage of folic acid of 400 mcg per day;
- Reduce consumption of foods containing the amino acid methionine:
- Fish,
- Meat,
- Cheese,
- Eggs,
- Nuts.
Any diet is prescribed individually, so to change your diet you should contact a specialist.
Sources:
- Kim, J., Kim, H., Roh, H., Kwon, Y., Causes of hyperhomocysteinemia and its pathological significance, 2021.
- S. Brustolin, R. Giugliani, and T. M. Félix, Genetics of homocysteine metabolism and associated disorders, 2010.
- Andrey N. Gaiday, Akylbek B. Tussupkaliyev, Saule K. Bermagambetova, Sagira S. Zhumagulova, Leyla K. Sarsembayeva, Moldir B. Dossimbetova, Zhanibek Zh Daribay, Effect of homocysteine on pregnancy: A systematic review, 2021.
- Elena Voskoboevaa, Alla Semyachkinab, Maria Yablonskayab, Ekaterina Nikolaevab, Homocystinuria due to cystathionine beta-synthase(CBS) deficiency in Russia: Molecular and clinical characterization, 2021.
- Natassia Robinsona, Peter Grabowskib, Ishtiaq Rehman, Alzheimer's disease pathogenesis: Is there a role for folate?, 2017.
- Nadia Bouzidi, Majed Hassine, Hajer fodha, Mejdi Ben Messaoud, Faouzi Maatouk4, Habib Gamra, Salima ferchichi, Association of the methylene-tetrahydrofolate reductase gene rs1801133 C677T variant with serum homocysteine levels, and the severity of coronary artery disease, 2021.
- NHS, Homocystinuria
How homocysteine levels are related to genetics
Different genetic variants affect how enzymes work. There are several main genes that affect homocysteine levels: MTHFR, CBS, MTR, MTRR. In this article we will look at the CBS and MTHFR genes.
A hereditary disease caused by a mutation in the CBS gene is called homocystinuria. The CBS gene encodes the enzyme cystathionine beta synthase, which converts homocysteine to cystathionine. This is one of the pathways for homocysteine metabolism. The presence of a defect leads to the fact that the reaction does not occur and the chain of sequential transformations of amino acids is disrupted. As a result, the levels of homocysteine and methionine increase in the blood and urine.
Homocystinuria is a rare disease. Although it may not be noticeable in the first years of life, vision problems, osteoporosis, thrombosis and stroke may develop in the future.
Another gene involved in homocysteine metabolism is called MTHFR. It affects the activity of the enzyme that converts vitamin B9 into its active form. The active form of vitamin B9 is involved in the conversion of homocysteine into another amino acid - methionine. Thus, the normal cycle of homocysteine metabolism is maintained.
There are several variants of the MTHFR gene. People with the C677T and A1298C variants have decreased enzyme activity, which can affect homocysteine levels.
A number of studies show that the C677T genetic variant is associated with the development of cardiovascular and neurological diseases. However, it cannot be said that the presence of this gene variant becomes a direct cause of disease. Many data are inconsistent and require further study. It is also important to note that homocysteine levels are also influenced by other genes, including those responsible for the transport of B vitamins. Therefore, it is necessary to take into account all factors and conduct an individual consultation with a doctor.
You can find out about your own risks associated with genetics using the Atlas Genetic Test.
Homocysteine and pregnancy
To date, the study of how homocysteine levels affect the course of pregnancy is still ongoing. Early evidence suggested that a mutation in the MTHFR gene, associated with elevated homocysteine levels, may lead to complications during pregnancy. Complications such as preeclampsia, early termination of pregnancy, and intrauterine growth disorders have been associated with homocysteine levels.
However, more modern sources claim that there is no reliable connection between the MTHFR gene variant and pregnancy complications.
When do homocysteine levels increase?
Hyperhomocysteinemia is an increased level of homocysteine in the blood: above 15 µmol/l.
Why is this happening?:
- Enzyme disruption . Homocysteine levels rise because enzymes cannot convert it into other amino acids. Such violations are rare, but can lead to serious complications. For example, a defect in the enzyme cystathionine beta synthase leads to changes in the lens, problems with intelligence and the early development of atherosclerosis.
- Lack of vitamins. If the body does not have enough vitamins B6, B9 and B12, then even enzymes with normal activity will not be able to work correctly. The cause of vitamin deficiency may be problems with intestinal function, alcoholism, liver disease and insufficient intake of vitamins from food.
- Renal dysfunction. The exact mechanism is unknown, but it may be related to impaired homocysteine excretion.