Hyperhomocysteinemia is a pathological condition, the timely diagnosis of which in the vast majority of cases makes it possible to prescribe simple, cheap, effective and safe treatment, which reduces the risk of many life-threatening diseases and complications tenfold. Homocysteine is a product of the conversion of methionine, one of the eight essential amino acids. From homocysteine, another amino acid, cysteine, which is not one of the essential amino acids, can subsequently be formed. Excess homocysteine that accumulates in the body can be converted back into methionine. Cofactors for enzymes in the methionine metabolic pathways in the body are vitamins, the most important of which are folic acid, pyridoxine (B6), cyanocobalamin (B12) and riboflavin (B1). Homocysteine is not a structural element of proteins, and therefore does not enter the body with food. Under physiological conditions, the only source of homocysteine in the body is the conversion of methionine. Homocysteine has a pronounced toxic effect on the cell. To protect the cell from the damaging effects of homocysteine, there are special mechanisms for removing it from the cell into the blood. If an excess of homocysteine appears in the body, it accumulates in the blood, and the main site of the damaging effect of this substance becomes the inner surface of the blood vessels. Hyperhomocysteinemia leads to damage and activation of endothelial cells (the cells lining blood vessels), which significantly increases the risk of developing thrombosis. High levels of homocysteine cause “oxidative stress”, increase platelet aggregation and cause activation of the coagulation cascade, leading to disruption of endothelium-dependent vasodilation and stimulation of smooth muscle cell proliferation. Thus, hyperhomocysteinemia has an adverse effect on the mechanisms regulating vascular tone, lipid metabolism and the coagulation cascade, thereby contributing to the development of a variety of vascular diseases. Back in 1969, K. McCully, for the first time, observing children with high (more than 100 µmol/l) blood homocysteine levels, noted that they early developed severe forms of arterial damage. Based on this, it was assumed that a high level of homocysteinemia is a risk factor for the development of both atherosclerotic and thrombogenic vascular damage.
Introduction
Homocysteine is a product of the conversion of methionine, one of the eight essential amino acids. From homocysteine, another amino acid, cysteine, which is not one of the essential amino acids, can subsequently be formed.
Excess homocysteine that accumulates in the body can be converted back into methionine. Cofactors for enzymes in the methionine metabolic pathways in the body are vitamins, the most important of which are folic acid, pyridoxine (vitamin B6), cyanocobalamin (vitamin B12) and riboflavin (vitamin B1).
Homocysteine is not a structural element of proteins, and therefore does not enter the body with food. Under physiological conditions, the only source of homocysteine in the body is the conversion of methionine.
Homocysteine has a pronounced toxic effect on the cell. To protect the cell from the damaging effects of homocysteine, there are special mechanisms for removing it from the cell into the blood. Therefore, if an excess of homocysteine appears in the body, it begins to accumulate in the blood, and the main place of the damaging effect of this substance becomes the inner surface of the blood vessels.
To convert excess homocysteine to methionine, high concentrations of the active form of folic acid (5-methyltetrahydrofolate) are required. The main enzyme that converts folic acid into its active form is 5,10 methylenetetrahydrofolate reductase (MTHFR). A decrease in the activity of this enzyme is one of the important reasons for the accumulation of homocysteine in the body. (Fig. 1)
Rice. 1
Please note that homocysteine can only be formed from methionine. Homocysteine can be converted either to cystathionine, which is subsequently used for the synthesis of cysteine, or to methionine. Vitamins play an important role in all key stages of methionine and homocysteine metabolism. Red indicates the methionine conversion cycle, green indicates the folic acid conversion cycle. MTHFR - 5,10 methylenetetrahydrofolate reductase. Methionine, homocysteine and folic acid are amino acids. Amino acids are the most important substrates for nitrogen metabolism in the body. Proteins, enzymes, purine and pyrimidine bases (and nucleic acids), pyrrole derivatives (porphyrins), biologically active compounds of peptide nature (hormones), as well as a number of other compounds originate from amino acids. When needed, amino acids can serve as a source of energy, mainly through the oxidation of their carbon skeleton. In living organisms, amino acids form a pool, the value of which in adulthood remains constant under physiological conditions. It corresponds to the difference between the supply of amino acids from the outside or sometimes from endogenous sources, and the consumption of amino acids that serve as substrates in anabolic and catabolic processes. Living organisms do not store amino acids and proteins for future use, so the required amount of nitrogen (preferably in the form of amino acids) must come from food. In an adult body under physiological conditions, the amount of nitrogen entering and exiting is the same (nitrogen balance). Amino acids from exogenous sources (from food) are absorbed in the digestive tract and transported by the blood to the liver and other tissues and organs, where they are further used. In addition, the source of amino acids (endogenous source) can be tissue proteins of the body, which are constantly subject to metabolism to release the amino acids they contain. These amino acids are used to a small extent for the synthesis of new proteins, but endogenous sources are very important because they provide about two-thirds of the total amino acid pool, and only one-third of the amino acids come from food. Essential amino acids are those amino acids that cannot be synthesized by a given body. For humans, these are valine, leucine, isoleucine, lysine, methionine, threonine, phenylalanine, tryptophan and, under certain conditions, also arginine and histidine.
Results of clinical studies conducted in recent years
Clinical trials (HOPE) 2 [7] and NORVIT [1] showed that the administration of folic acid, vitamin B6 and vitamin B12 does not reduce the number of recurrent heart attacks. However, Refsum H. and Smith AD made a number of criticisms of the data obtained in these studies, which are highly probable [8]:
- The patients' mean levels of homocysteine, vitamin B6, vitamin B12, and folic acid were within the normal range in both studies. Therefore, no big effect should be expected.
- 70% of patients in the (HOPE) 2 study received folic acid-fortified flour products. Therefore, the control group also had good homocysteine levels in the blood.
- The duration of the studies (2-3 years) was too short, since atherosclerosis develops over decades.
- A reanalysis of data from the VISP trial (excluding patients with renal impairment) showed a 21% reduction in stroke [9, 10].
- Since 1998, National Programs for fortifying flour with folic acid have been introduced in the USA and Canada. Studies have shown a significant reduction in mortality from stroke in women after 5 years (see Fig. 1). Homocysteine levels in the blood of the population also decreased [12].
- A study of men and women aged 50–70 years with elevated blood homocysteine levels found that when folic acid was prescribed for more than 3 years, homocysteine levels decreased by 26% [2].
The reduction in stroke mortality in women in the US and Canada after flour fortification with folic acid is shown in the chart below:
Rice. 1. Mortality from stroke in women in the USA and Canada before and after fortification of flour with folic acid (number of cases per 100,000) [12]
The average reduction in stroke mortality in Canada was -1.0% annually from 1990 to 1997 and increased to -5.4% annually from 1998 to 2002 (p < 0.0001).
Background
In 1932, De Vigneaud discovered homocysteine as a product of methionine demethylation. A few years later, a second pathway for homocysteine metabolism was discovered—transsulfuration. In 1962, homocyteinuria syndrome (homocysteine in the urine) was discovered, associated with a deficiency of the enzyme cystathionine synthase. This disease causes mental retardation, bone deformities, lens displacement, progressive cardiovascular disease, and a very high incidence of thromboembolism. Kilmer McCully studied in depth patients with high levels of homocysteine in the blood and found a link between hyperhomocysteinemia and the development of severe vascular disease. These studies served as the basis for the homocysteine theory of atherosclerosis that he proposed in 1975. He was convinced that there was a connection between homocysteine levels, vitamin deficiency and heart disease.
Research over the past 15 years has confirmed and deepened the homocysteine theory of the development of vascular disorders. Every year dozens of publications appear devoted to different aspects of this problem. However, unfortunately, at present only a few laboratories can determine the level of homocysteine in the blood.
Causes of increased homocysteine levels in the blood
Homocysteine levels in the blood gradually increase throughout life. Before puberty, homocysteine levels are approximately the same in boys and girls (about 5 µmol/L). During puberty, homocysteine levels rise to 6-7 µmol/l; in boys this increase is more pronounced than in girls.
In adults, homocysteine levels fluctuate around 10-11 µmol/ml; in men this figure is usually higher than in women. With age, homocysteine levels gradually increase, and in women the rate of increase is faster than in men. The gradual increase in homocysteine levels with age has been attributed to decreased kidney function, and higher homocysteine levels in men have been attributed to greater muscle mass.
During pregnancy, normal homocysteine levels tend to decrease. This decrease usually occurs at the border of the first and second trimesters of pregnancy, and then remains relatively stable. Normal homocysteine levels are restored 2-4 days after birth. It is believed that a decrease in homocysteine levels during pregnancy favors placental circulation. The level of homocysteine in the blood is inversely proportional to the weight of the fetus and newborn.
Homocysteine levels in the blood can increase for many reasons. One of the factors is an increased intake of methionine from food. Therefore, during pregnancy, additional administration of methionine tablets, still practiced by some doctors, should be carried out with caution and under the control of homocysteine levels. The most common causes of increased homocysteine levels are vitamin deficiency conditions. The body is especially sensitive to a lack of folic acid and vitamins B6, B12 and B1. It is assumed that smokers have an increased tendency to hyperhomocysteinemia. Consuming large amounts of coffee is one of the most powerful factors in increasing homocysteine levels in the blood. Individuals who drink more than 6 cups of coffee per day have homocysteine levels that are 2-3 µmol/L higher than those who do not drink coffee. It is assumed that the negative effect of caffeine on homocysteine levels is associated with changes in kidney function. Homocysteine levels often increase with a sedentary lifestyle. Moderate physical activity helps reduce homocysteine levels in hyperhomocysteinemia. Drinking small amounts of alcohol can lower homocysteine levels, while large amounts of alcohol increase homocysteine in the blood.
Homocysteine levels are affected by a number of medications. The mechanism of their action may be related to the effect on the action of vitamins, homocysteine production, kidney function, and hormone levels. Of particular importance are methotrexate (a folic acid antagonist, often used to treat psoriasis), anticonvulsants (phenytoin, etc., deplete folic acid reserves in the liver), nitrous oxide (a drug used for anesthesia and for pain relief in childbirth, inactivates vitamin B12), metformin (a drug used to treat diabetes mellitus and polycystic ovary syndrome) and H2 receptor antagonists (affect the absorption of vitamin B12), aminophylline (inhibits the activity of vitamin B6, often used in obstetric hospitals for the treatment of gestosis). Homocysteine levels may be adversely affected by taking hormonal contraceptives, but this is not always the case.
Another factor that contributes to increased homocysteine levels is certain concomitant diseases. The most important of these are vitamin deficiency conditions and renal failure. Thyroid diseases, diabetes mellitus, psoriasis and leukemia can contribute to a significant increase in homocysteine levels in the blood.
One of the main causes of vitamin deficiency conditions leading to hyperhomocysteinemia are diseases of the gastrointestinal tract, accompanied by impaired absorption of vitamins (malabsorption syndrome). This explains the higher incidence of vascular complications in the presence of chronic gastrointestinal diseases, as well as the fact that with B12 vitamin deficiency, the common cause of death is not anemia, but strokes and heart attacks.
One of the important factors contributing to the increase in homocysteine in the blood is hereditary predisposition. The most studied is a defect in the enzyme 5,10 methylenetetrahydrofolate reductase (MTHFR). MTHFR mediates the conversion of 5,10-methylenetetrahydrofolate to 5-methyltetrahydrofolate, which is the main circulating form of folic acid in the body. In turn, folic acid is used in many biochemical pathways, including the methylation of homocysteine and other substances and the synthesis of nucleotides. The MTHFR gene is located on chromosome 1 at locus 1p36.3. There are several allelic variants of this enzyme that cause severe MTHFR deficiency, but most of these variants are very rare. Two alleles are of practical importance: the heat-labile allele C677T and the allele A1298C (sometimes referred to as C1298A). The C677T allele is the result of a point mutation in which alanine is replaced by valine at position 677. In this case, the normal genotype is designated as CC (normal gene variants on both chromosomes), heterozygous - as CT (carrier, on one chromosome there is a normal gene, and on the other - mutant), genotype homozygous for the mutant gene - as TT (mutant on both chromosomes). gene). Currently, DNA diagnostics of the C677T mutation is carried out in some medical centers in Moscow. The features of this mutation are presented in Fig. 2.
Rice. 2 C677T polymorphism of 5,10 methylenetetrahydrofolate reductase (MTHFR) affects the distribution of folic acid compounds (highlighted in green), used for the synthesis of DNA and RNA, and 5-methyltetrahydrofolate, necessary for the remethylation of homocysteine (Hcy), and therefore for the synthesis squirrel. The pie chart shows the genotype distribution typical of European populations, and the sizes of the arrows indicate the relative enzyme activity of MTHFR. Abbreviations: AdoMet, S-adenosylmethionine; CHOTHF, formyltetrahydrofolate; CHTHF, methenyltetrahydrofolate; CH2THF, 5,10-methylenetetrahydrofolate; CH3DNA, methylated DNA; CH3THF, 5-methyltetrahydrofolate; DHF, dihydrofolate; dTMP, dioxythymidine 5'-monophosphate; dUMP, deoxyuridine 5'-monophosphate; FAD, flavin adenine dinucleotide; Hcy, homocysteine; Met, methionine; THF, tetrahydrofolate; protein, protein; DNA, DNA; RNA, RNA; purines, purine bases. CC and TT are homozygous genotypes, CT is a heterozygous genotype. When enzyme activity decreases, there may not be enough 5-methyltetrahydrofolate to effectively convert homocysteine to methionine, and homocysteine begins to accumulate in the body.
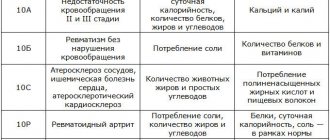
| Homocysteine level | Frequency1 | Common reasons1 |
| Moderate increase (15-30 µmol/l) | 10% | Unhealthy lifestyle, including poor and unbalanced diet MTHFR polymorphism combined with low folate status (S-folate at the lower limit of normal) Folic acid deficiency Moderate vitamin B12 deficiency Renal failure Hyperproliferative disorders Medication use |
| Increase of moderate severity (30-100 µmol/l) | MTHFR polymorphism in combination with folic acid deficiency Moderate vitamin B12 deficiency Severe folic acid deficiency Severe renal failure | |
| Severe increase (>100 µmol/l) | 0,02% | Severe vitamin B12 deficiency CBS deficiency (homozygous form) |
Table 1. Common causes of various degrees of hyperhomocysteinemia
1Data on the causes of homocysteinemia and its frequency are based on European studies. These data may vary significantly among different populations. According to our data, the frequency of moderate hyperhomocysteinemia in Moscow significantly exceeds the European average. A moderate increase in homocysteine in Muscovites is often detected even when taking large doses of vitamins, which may be associated with a high incidence of disturbances in the absorption of vitamins in the stomach and intestines. Abbreviations: CBS - cystathionine beta synthase
Homocysteine is a predictor of pathological changes in the human body
Homocysteine (Hcy) is a naturally occurring sulfur-containing amino acid not found in proteins. Hcy is a metabolic product of methionine (Met), one of the 8 essential amino acids in the body.
In blood plasma, free (reduced) Hcy is present in small amounts of 1–2% (Fig. 1). Approximately 20% is in the oxidized state, mainly in the form of a mixed disulfide of cysteinyl homocysteine and homocystine. About 80% of Hcy binds to blood plasma proteins, mainly albumin, forming a disulfide bond with cysteine-34.
The metabolism of homocysteine occurs with the participation of a number of enzymes, the main of which are: methylenetetrahydrofolate reductase (MTHFR) and cystathione-β-synthetase (CBC).
In addition to enzymes, vitamins B6, B12 and folic acid play an important role in the metabolism of homocysteine.
Met is converted to S-adenosylmethionine (SAM) by the enzyme methionine adenosyltransferase. As a result of methylation reactions carried out by methyltransferases, SAM is converted to S-adenosylhomocysteine (SAH). SAH is subsequently hydrolyzed by SAH hydrolase to form Hcy and adenosine. This cascade of enzymatic reactions, referred to as transmethylation, occurs in almost every cell of the human body.
SAM-dependent transmethylation reactions are important for a variety of cellular processes, such as methylation of nucleic acids, proteins and phospholipids.
There are several pathways for the biotransformation of Hcy in the human body [6]. It can be converted back to Met in two ways (Figure 2). First, Met can be reduced from Hcy by methionine synthase (MS), which uses 5-methyl-tetrahydrofolate (5-MeTHF) as a methyl group donor. This remethylation pathway is ubiquitous, primarily in liver cells and, in some species, in the kidney. Second, glycine-betaine (NNN-trimethylglycine) can also be remethylated to Met by betaine homocysteine methyltransferase (BHMT). Hcy can also be converted to cysteine. Under the action of cystathionine-β-synthase, Hcy and serine form cystathionine, which can be degraded by cystathionine-γ-lyase to cysteine and α-ketobutyrate, which is further metabolized by enzymes to succinyl-CoA. This series of reactions that convert Hcy to cysteine occurs in the liver, kidneys, small intestine, and pancreas. Hcy can also be excreted from cells into the blood, but transporters for this process have not yet been identified.
These two pathways of Hcy conversion (remethylation to Met, requiring folate and B12, and conversion to cystathionine, requiring pyrodoxal phosphate) are coordinated by S-adenosylmethionine, which acts as an allosteric inhibitor of methylenetetrahydrofolate reductase and as an activator of cystathionine-b-synthase.
In numerous population studies, the lower limit for homocysteine levels is usually determined fairly clearly (5 μmol/L), but the upper limit usually varies between 10 and 20 mmol/L - depending on age, gender, ethnic group and folate intake patterns.
Various hereditary and acquired disorders in the body lead to the fact that Hcy is not utilized. In this case, it accumulates in the body and becomes dangerous for it, causing a number of pathological effects. There are several forms of hyperhomocysteinemia (HHC) [2].
Severe form of HHC (>100
m
mol/l)
The reason may be:
– hereditary homocysteinuria, for example, due to homozygosity for defective genes for enzymes of methionine biosynthesis - cystathionine-b-synthase or 5,10-methylenetetrahydrofolate reductase;
– hereditary disorders of vitamin B12 utilization;
– severe vitamin B12 deficiency.
Moderate form of HHC (30–100
m mol/l)
Causes:
– severe renal dysfunction (reduced clearance of homocysteine by the kidneys);
– moderate B12 deficiency;
– severe folate deficiency.
Mild form of HHC (10–30 μmol/l)
Reasons may include:
– -heterozygosity for a defective cystathionine-b-synthase gene;
– homozygosity for the C677T base substitution in the 5,10-methylenetetrahydrofolate reductase gene;
– renal failure;
– kidney transplantation;
– slight deficiency of folate and vitamin B12;
– lack of thyroid hormones;
– alcoholism;
– medicines.
Hcy metabolism is highly dependent on cofactors - vitamin derivatives. Therefore, deficiency of any of the vitamins (B12, folic acid and B6) can lead to HHC.
Genetic mutations can also cause hyperhomocysteinemia, in particular, defects in the enzymes cystathionine β-synthase and cystathionine γ-lyase or methylenetetrahydrofolate reductase.
When studying polymorphism in the methylenetetrahydrofolate reductase (MTHER) gene associated with the 677C→T substitution, it was found that 10–16% of the population have homozygosity for the TT variant, and carriers of this variant are characterized by an increased Hcy content. If individuals who are genetically predisposed to elevated Hcy levels smoke and drink a lot of coffee, they become especially sensitive to increased Hcy concentrations. The genotype with the 677C→T substitution in the MTHER gene is predisposed to an increased risk of neural tube defects and cardiovascular diseases [7,8].
Research over the past 15 years has established that homocysteine is a ranked independent risk factor for cardiovascular diseases (CVD) - myocardial infarction, stroke and venous thromboembolism, atherosclerosis [9,10]. It is believed that hyperhomocysteinemia is a more informative indicator of the development of diseases of the cardiovascular system than cholesterol [11].
Hcy damages the walls of blood vessels, making their surface loose. Cholesterol and calcium are deposited on the damaged surface, forming an atherosclerotic plaque. Elevated Hcy levels increase thrombus formation. An increase in blood homocysteine levels by 5 µmol/l leads to an increase in the risk of atherosclerotic vascular damage by 80% in women and 60% in men.
By inhibiting the work of the anticoagulant system, homocysteinemia is one of the links in the pathogenesis of early thrombovascular disease; in its presence, the risk of developing thrombosis and deep veins increases. Patients with diabetes are at particular risk.
It has been shown that with an increase in plasma Hcy levels by 2.5 μmol/L, the risk of myocardial infarction increases by 10%, and the risk of stroke by 20% [12]. Elevated homocysteine levels are a strong predictor of mortality in people with pre-existing CVD or known other risk factors [13].
The mechanisms of influence of homocysteinemia on blood vessels may include damage due to oxidative stress, disturbances in the release of nitric oxide, changes in homeostasis and activation of inflammatory pathways.
It is also possible that high Hcy levels are only a marker of CVD, that is, the connection between them is mediated by other factors (impaired kidney function, deficiency of folate and vitamins B12 and B6), which affect both the level of Hcy and the development of vascular diseases.
Hyperhomocysteinemia is common among patients with chronic renal failure (where kidney function is reduced, but not so low that replacement therapy is required) and is almost always observed in end-stage renal disease [14]. This fact is especially important for some patients who have cardiovascular failure: their risk of death increases 30 times compared to the main group of patients.
In renal failure, Hcy levels increase, and the majority of dialysis patients (>85%) exhibit a mild degree of hyperhomocysteinemia. Creatinine clearance, which determines the presence of renal failure, inversely correlates with plasma Hcy levels. Studies conducted in healthy people and diabetic patients have confirmed the inverse relationship between Hcy levels and renal function, as well as the role of creatinine as a marker of renal failure [15].
Microthrombi formation leads to disruption of the uterine and fetoplacental circulation, which can cause infertility and miscarriage, and therefore determination of the Hcy level is relevant in obstetric practice for predicting possible complications during pregnancy and childbirth. Changes in Hcy levels may be associated with folate deficiency, which has multiple effects on fetal development [16]. In later stages of pregnancy, hyperhomocysteinemia causes the development of chronic fetoplacental insufficiency, chronic intrauterine fetal hypoxia, and, as a consequence, intrauterine fetal hypotrophy. An increase in homocysteine levels is one of the reasons for the birth of children with developmental defects (neural tube defects). In view of these circumstances, it is recommended to check the level of homocysteine in women giving birth with previous obstetric complications or who have relatives who had strokes, heart attacks and thrombosis at a fairly early age.
There are a number of premises indicating a connection between increased homocysteine levels and impaired cognitive function and mental disorders. An increase in the level of Hcy in the blood to 14.5 μmol/L leads to a twofold increase in the risk of Alzheimer's disease at the age of over 60 years [17]. It has been shown that an increase in Hcy concentration in the blood directly correlates with cognitive disorders in elderly people [18].
Among the factors influencing the content of homocysteine in the blood, the above-described genetic predisposition to increased Hcy levels, smoking, and diet (consumption of large amounts of protein foods, coffee, B vitamins, folates) should be highlighted.
Population studies have made it possible to analyze the relationship between dietary factors (B vitamins, proteins and methionine), smoking, coffee consumption, biochemical determinants (plasma creatinine, B6, B12, folate) and other factors (body mass index, blood pressure and antihypertensive drugs) with homocysteine levels. Apart from blood pressure, all other factors were associated with Hcy content. For example, in smokers the Hcy content was 1.5 μmol/L higher than in non-smokers. Folate content was the strongest determinant of Hcy levels. The differences in Hcy levels at the highest and lowest folate concentrations were 4 μmol/L, and under the influence of other factors were in the range of 0.5–2.0 μmol/L. The determinants of Hcy content varied greatly depending on gender and age, as well as on the characteristics of the national diet in different countries associated with the content of B vitamins [19].
The most common cause of HHC is folic acid deficiency, as well as a lack of vitamin B
12, which, even with sufficient folic acid intake, can lead to homocysteine accumulation.
Some drugs (eg, penicillamine, cyclosporine, methotrexate, carbamazepine, phenytoin, 6-azauridine, nitrous oxide) may increase homocysteine levels. The mechanism of action of these factors is due to either direct or indirect antagonism with enzymes or cofactors involved in Hcy metabolism.
The reasons for the increase in Hcy content in the blood can be a number of diseases (chronic renal failure, hypofunction of the thyroid gland, B12-deficiency anemia, cancer).
The effect of physical activity on Hcy levels is controversial. Thus, it has been shown [20] that after a marathon, runners (with the exception of professional athletes) experience a sharp increase in Hcy content in the body. In other studies, the increase in Hcy concentration observed in athletes is associated with diet [21]. Dosed intake of vitamins B6, B12 and folic acid helps prevent possible complications.
Although homocysteine-lowering therapy has not yet been definitively proven to reduce the risk of CVD, it is inexpensive and continues to be used. The goal of therapy should be to reduce homocysteine levels in patients at high risk of heart disease to 10 μmol/L
.
In patients with low to moderate hyperhomocysthenia, Hcy levels can be reduced to normal levels by administering either folic acid 0.4 to 5 mg/day, vitamin B12 0.5 to 1 mg/day, or both. drug. Treatment is less effective in patients with kidney disease.
It is generally accepted to use folic acid, folic acid in combination with vitamins B6 and B12 and a combination of vitamins B6 and B12, and the use of drugs such as cardonate (a combination drug containing coenzymes B1, B6, B12, as well as carnitine and lysine) for the treatment of homocysteinemia. Folic acid, originally found in spinach, is present in most plant foods that have leaves (hence its name, from the Latin word folium - leaf), green vegetables, fish and liver.
But there is evidence that therapeutic intervention for elevated Hcy levels should not be limited to replenishing vitamin and folate deficiencies and combating well-known risk factors such as smoking and excess coffee consumption.
Thus, it has been shown that therapy with high doses of folic acid, vitamins B6 and B12 does not reduce mortality and the incidence of cardiovascular events in patients with severe renal failure, and therefore cannot be recommended for this purpose. Moreover, when exogenous folic acid is administered, there is a short-term increase in Hcy levels. Among the possible reasons for the low effectiveness of vitamin therapy, the authors note the exceptional clinical severity and poor short-term prognosis of the included patients, the achievement of normal Hcy levels in only a third of the participants, and the side effects of vitamin therapy that neutralize its beneficial effect. The authors believe that one of the reasons for the failure to reduce Hcy is that its level is a marker and not a cause of CVD [22].
A promising direction in the treatment of homocysteinemia may be the use of hydroxymethylglutaryl-CoA reductase inhibitors (statins). There is evidence to suggest that a decrease in homocysteine levels is one of the effects of statin use in patients with CVD [23].
In conclusion, it should be noted that an increase in the level of Hcy in the blood is associated both with an increase in mortality in the population in general, and with diseases of the cardiovascular system, in particular [24]. According to some estimates, if Hcy levels could be reduced by 40%, this would lead to the preservation of 8 years of life per 1000 men and 4 years of life per 1000 women. This circumstance stimulates the introduction of Hcy concentration monitoring into widespread clinical practice.
References 1. Friedman AN, Bostom AG, Selhub J. et al. The kidney and homocysteine metabolism. J. Am Soc. Nephrol., 2001, v. 12, p. 2181–2189. 2. Lentz SR, Haynes WG Homocysteine: Is it a clinically important cardiovascular risk factor? Clev. Clin. J. Med., 2004, v. 71, p. 729–734. 3. Daly S., Cotter A., Molloy AE, Scott J. Homocysteine and folic acid: implications for pregnancy. Semin. Vasc. Med., 2005, v. 5, p. 190–200. 4. Ciaccio M., Bivona G., Bellia C. Therapeutic approach to plasma homocysteine and cardiovascular risk reduction Therapeutics. and Clin. Risk Manag., 2008, v. 4, p. 219–224. 5. Vollset SE, Refsum H., Ueland PM Population determinants of homocysteine. Am J. Clin Nutr., 2001, v. 73, p. 499–500. 6. Szegedi SS, Castro CC, Koutmos M., Garrow TA Betaine–homocysteine s–methyltransferase–2 is an s–methylmethionine–homocysteine methyltransferase. J Biol. Chem., 2008, v. 283, p. 8939–8945. 7. Kraus JP Biochemistry and molecular genetics of cystathionine beta-synthase deficiency. Eur. J. Pediatr., 1998, v. 157, p. 50–53. 8. Trabetti E. Homocysteine, MTHFR gene polymorphisms, and cardio-cerebrovascular risk. J. Appl. Genet., 2008, v. 49, p. 267–282. 9. Naess IA, Christiansen SC, Romundstad PR et al. Prospective study of homocysteine and MTHFR 677TT genotype and risk for venous thrombosis in a general population—results from the HUNT 2 study. Br. J. Haematol., 2008, v. 141, p. 529–535. 10. Moat SJ Plasma total homocysteine: instigator or indicator of cardiovascular disease? Ann. Clin. Biochem., 2008, v. 45, p. 345–348. 11. Potter K. Homocysteine and cardiovascular disease: should we treat? Clin. Biochem. Rev., 2008, v. 29, p. 27–30. 12. Virtanen JK, Voutilainen S., Alfthan G. Homocysteine as a risk factor for CVD mortality in men with other CVD risk factors: the Kuopio Ischemic Heart Disease Risk Factors (KIHD) Study. J. Intl. Med., 2005, v. 257, p. 255–262. 13. Homocysteine Studies Collaboration. Homocysteine and risk of ischemic heart disease and stroke: a meta-analysis. JAMA, 2002, v. 288, p. 2015–2022. 14. Bostom AG, Culleton BF Hyperhomocysteinemia in chronic renal disease. J. Am. Soc. Nephrol., 1999, v. 10, p. 891–900. 15. Bostom AG, Kronenberg F., Schwenger V. et al. Proteinuria and total plasma homocysteine levels in chronic renal disease patients with a normal range serum creatinine: Critical impact of true GFR. J. Am. Soc. Nephrol., 2000, v. 11, p. 305–310. 16. Beaudin AE, Stover PJ. Folate–mediated one–carbon metabolism and neural tube defects: balancing genome synthesis and gene expression. Birth. Defects Res. C. Embryo Today., 2007, v. 81, p. 183–203. 17. Kidd PM Alzheimer's disease, amnestic mild cognitive impairment, and age–associated memory impairment: current understanding and progress toward integrative prevention. Altern. Med. Rev., 2008, v. 13, p. 85–115. 18. Schafer JH, Glass TA, Bolla KI et al. Homocysteine and Cognitive Function in a Population–based Study of Older Adults. J. Am. Geriatr. Soc., 2005, v. 53, p. 381–388. 19. Tolmunen T., Hintikka J., Voutilainen S. et al. Association between depressive symptoms and serum concentrations of homocysteine in men: a population study. Am. J. Clin. Nutr., 2004, v. 80, p. 1574–1578. 20. Real JT, Merchante A, Gomez JL et al. Effects of marathon running on plasma total homocysteine concentration. Nutr. Metab. Cardiovasc. Dis., 2005, v. 15, p. 134–13 21. Ko??nig D., Bisse E., Deibert P. et al. Influence of training volume and acute physical exercise on the homocysteine levels in endurance–trained men: interactions with plasma folate and vitamin B12. Ann. Nutr. Metab., 2003, v. 47, p. 114–118. 22. Jamison RL, Hartigan P, Kaufman JS et al. Effect of Homocysteine Lowering on Mortality and Vascular Disease in Advanced Chronic Kidney Disease and End–stage Renal Disease. A Randomized Controlled Trial. JAMA., 2007, v. 298, p. 1163–1170. 23. Dierkes J., Luley C., Westphal S. Effect of lipid-lowering and anti-hypertensive drugs on plasma homocysteine levels. Vasc. Health Risk Manag., 2007, v. 3, p. 99–108. 24. Malinow MR Plasma concentrations of total homocysteine predict mortality risk. Am. J. Clin. Nutr., 2001, v. 74, p. 3.
Hyperhomocysteinemia and pregnancy pathology
Hyperhomocysteinemia leads to damage and activation of endothelial cells (the cells lining blood vessels), which significantly increases the risk of developing thrombosis. Not all details of the mechanism of the pathological action of hyperhomocysteinemia have been fully studied, but much is already known.
The thrombogenic effect of homocysteine may be associated with damage to endothelial cells, nonspecific inhibition of prostacyclin synthesis, activation of factor V, inhibition of protein C activation, down-regulation of thrombomodulin expression, blockade of tissue plasminogen activator binding by endothelial cells. In addition, high homocysteine levels increase platelet aggregation due to decreased endothelial synthesis of relaxing factor and NO, induction of tissue factor, and stimulation of smooth muscle cell proliferation.
Microthrombi formation and microcirculation disorders lead to a number of obstetric complications. Disorders of placentation and fetoplacental circulation can cause reproductive failure: miscarriage and infertility as a result of defects in embryo implantation. In later stages of pregnancy, hyperhomocysteinemia causes the development of chronic fetoplacental insufficiency and chronic intrauterine fetal hypoxia. This leads to the birth of children with low body weight and a decrease in the functional reserves of all life-supporting systems of the newborn and the development of a number of complications during the newborn period.
Hyperhomocysteinemia may be one of the reasons for the development of generalized microangiopathy in the second half of pregnancy, manifested in the form of late toxicosis (preeclampsia): nephropathy, preeclampsia and eclampsia. Hyperhomocysteinemia is characterized by the development of severe, often uncontrollable conditions that can lead to early termination of pregnancy for medical reasons. The birth of an immature premature baby in such cases is accompanied by high infant mortality and a high percentage of neonatal complications.
Homocysteine freely crosses the placenta and can have teratogenic and fetotoxic effects. Hyperhomocysteinemia has been shown to be one of the causes of anencephaly and spina bifida.
).
Anencephaly has a 100% mortality rate, and spina bifida
causes serious neurological problems in the child, including motor paralysis, lifelong disability and premature death. A direct toxic effect of excess homocysteine levels on the fetal nervous system cannot be excluded.
Hyperhomocysteinemia can be not only the cause, but also a companion to obstetric complications. It is assumed that in some cases problems may be associated not only with high homocysteine levels, but also with those conditions that cause the development of hyperhomocysteinemia (vitamin deficiency conditions, concomitant diseases, etc.)
It should be remembered that hyperhomocysteinemia can be accompanied by the development of secondary autoimmune reactions and is currently considered as one of the causes of antiphospholipid syndrome. Autoimmune factors can interfere with the normal development of pregnancy even after high homocysteine levels are eliminated.
Diagnosis of hyperhomocysteinemia
To diagnose hyperhomocysteinemia, the level of homocysteine in the blood is determined. For the differential diagnosis of various forms of homocysteinemia, stress tests with methionine are sometimes used (determining the level of homocysteine on an empty stomach and after a methionine load).
To find out the causes of hyperhomocysteinemia, DNA diagnostics of hereditary defects in enzymes involved in the metabolism of methionine and folic acid, in particular MTHFR, and determination of the level of vitamins B6, B12, B1 and folic acid in the blood are carried out.
If high levels of homocysteine in the blood are detected, tests are recommended to exclude additional risk factors for the development of vascular and obstetric complications. We recommend a hemostasiogram, a blood test for lupus anticoagulant, a test for antiphospholipid and anti-DNA antibodies, anti-thyroid antibodies, anti-nerve growth factor antibodies, and a blood test for hereditary hemostatic defects (Leiden mutation and hereditary prothrombin defects). Other tests may be prescribed according to indications.
Indications for a blood test for homocysteine
Homocysteine determination is carried out to assess the risk of arterial or venous thrombosis, especially at a young age. At the same time, the level of vitamin B12 and folic acid is determined to determine (exclude) hyperhomocysteinemia resulting from vitamin deficiencies. A blood test for homocysteine is done if a patient is suspected of having a hereditary disorder of methionine metabolism, including deficiency of cystathionine beta synthase (homocystinuria) and deficiency of methylenetetrahydrofolate reductase and its thermolabile variants - deficiency of methionine synthase, disorder of cobalamin metabolism.
Treatment of hyperhomocysteinemia
If hyperhomocysteinemia is detected, specially selected therapy is carried out with high doses of folic acid and B vitamins (B6, B12, B1). Considering that in many cases a vitamin deficiency state is associated with impaired absorption of vitamins in the gastrointestinal tract, treatment usually begins with intramuscular administration of B vitamins. After homocysteine levels have decreased to normal (5-15 mcg/ml), maintenance doses are prescribed vitamins per os
.
During pregnancy, antiplatelet therapy may be indicated (small doses of aspirin, which in this case acts as a kind of pregnancy vitamin, small doses of heparin drugs). If antiphospholipid syndrome is present, additional treatment may be prescribed.
Hyperhomocysteinemia is a pathological condition, the timely diagnosis of which in the vast majority of cases makes it possible to prescribe simple, safe and effective treatment, which reduces the risk of complications in mother and child tenfold.
Tags: pregnancy, homocysteine