General information
Literally translated from Greek, cardiopathy means kardia - heart, pathos - disease and unites a whole group of pathologies of the heart muscle of various origins; it is assigned the code “cardiopathy” according to ICD-10 I42.
As the main organ pumping blood in the body, the heart has a special structure of striated muscle fibers, structure and conductivity, which ensures normal functioning and constant contraction every minute of life of any organism with a developed circulatory system. Most often, disorders are expressed in the form of inadequate hypertrophy - thickening of the walls of the ventricles or septa, in the form of dilatation - stretching of the cavities or myocardial rigidity - increased tone, impeding mobility (restrictive type).
Types of cardiopathy
If conduction is impaired arrhythmias ; if the coronary system is affected, ischemic disorders occur, which can lead to a heart attack .
All this leads to heart failure and dysfunction of the heart muscle, which makes it impossible to pump blood in the volumes necessary for the functioning of all organs and tissues of the body.
Methods for diagnosing functional cardiopathy
Clinical and instrumental methods are used for diagnosis
ECG: signs of myocardial hypertrophy, rhythm and conduction disturbances, ST changes.
X-ray of the lungs: you can see hypertrophy, dilatation of the myocardium, congestion in the lungs.
EchoGK: allows you to evaluate the size of the heart cavities, the condition of the valves, the thickness of the walls and interventricular septum, and evaluate systolic and diastolic functions.
Sometimes they use: MRI, radioisotope ventriculography, angiocardiography, cardiac catheterization, endomyocardial biopsy is taken.
Pathogenesis
Damage to the heart muscle is primarily associated with its mechanical (blood pumping) and electrical functions (conductivity). The basis of pathological processes is:
- the presence of infectious, viral and inflammatory aspects;
- autoimmune disorders - heart proteins can acquire antigenic characteristics, which provokes the synthesis of antibodies to them and leads to stretching of the heart chambers and systolic dysfunction;
- poisoning with various chemicals, including heavy metals, medications, alcohol, drugs, etc.;
- environmental factors, including radiation damage;
- decompensation of conditions;
- injuries;
- ischemia – lack of blood supply to the heart muscle itself;
- birth defects – heart defects and genetic predisposition;
- cancer formation.
Functional cardiopathy
Functional pathology is associated with impaired ability to perform the main task of the heart - pumping blood. Exposure to negative factors can lead to a decrease in the number of normally and fully functioning heart cells - cardiomyocytes. This leads to a decrease in cardiac output, which can lead to deterioration of coronary perfusion, decreased tissue oxygenation, fluid retention, activation of the sympathetic nervous and renin-angiotensin systems, peripheral vasoconstriction, tachycardia and arrhythmias .
It happens that cardiac disorders are not part of a generalized disease, but are isolated. They can lead not only to disability, but also to death.
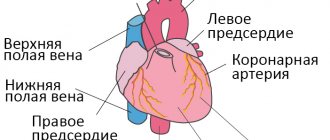
Structure of the heart
Degrees and stages
Cardiomyopathies are classified into degrees and stages of dilated cardiomyopathy and other types.
They have 3 degrees of severity:
- Moderate severity. The disease was diagnosed at an early stage, there are no pronounced pathological changes, the symptoms are not pronounced, and there are no signs of heart failure.
- Moderate severity. There are pronounced changes in the functioning of the heart muscle, myocardial decompensation, and the initial stage of heart failure.
- Severe degree. Heart failure develops, symptoms are severe, and the pathological process decompensates.
Cardiomyopathy goes through 3 stages in its development:
- Stage 1 – initial. The first symptoms of cardiomyopathy are observed; they are of an unexpressed nature.
- Stage 2 – height. There is a gradual increase in clinical symptoms, and there may be a sharp progression.
- Stage 3 – terminal. At this stage, irreversible heart damage occurs. Severe clinical symptoms with symptoms of heart failure are observed. At this stage, treatment is no longer effective and therefore therapy is symptomatic.
Classification
Depending on the origin, cardiac disorders can be primary or idiopathic, without an established cause; they are most often based on genetic changes that cause:
- hypertrophic - an autosomal dominant disease, which results in the formation of thickening of the wall of the left ventricle or, less commonly, the right, which are distinguished by a chaotic arrangement of the fibers of the heart muscles, provoke pathological mutations of the genes responsible for encoding the synthesis of myocardial proteins;
- arrhythmogenic right ventricular - genetically determined replacement of muscle fibers with fatty and fibrous tissues, at risk are young men suffering from fainting;
- non-compact left ventricular myocardia - which is characterized by a primary genetically determined abnormal spongy structure of the internal part facing the middle of the chamber;
- ion channelopathies - “electrical diseases” that disrupt heart rhythm due to mutations in genes encoding proteins of cell membranes responsible for transmembrane currents of sodium and potassium ions;
- Lenegra's disease - degenerative-sclerotic changes and intraventricular calcification, fibrosis of the connective stroma, provoking a progressive slowdown in conduction, usually caused by a defect in the SCN5A gene;
Diseases of mixed etiology are dilatational , causing the progression of heart failure due to stretching of the walls of the chambers without thickening them. There are cardiopathy resulting from acquired inflammatory, stress-induced and postpartum changes, as well as primary restrictive cardiopathy .
Secondary - associated with the course of various systemic diseases - hemochromatosis , amyloidosis , sarcoidosis , scleroderma , carcinoid , coronary heart disease , glycogenesis , anthracycline intoxication and conditions after exposure to negative factors. The most common among them:
- alcoholic – accompanied by rhythm disturbances, irreversible changes under the influence of ethyl alcohol and leading to severe failure and multiple organ disorders;
- thyrotoxic - a frequent complication of thyrotoxicosis , which uncouples oxidative phosphorylation and a decrease in the content of ATP and creatine phosphates , while protein breakdown predominates, the amount of energy resources and plastic processes decreases, which ultimately inhibits contractile function;
- diabetic cardiovascular pathology - leads to changes under the influence of diabetes mellitus , leads to failure, increasing the risk of heart attacks and cardiosclerosis ;
- autoimmune – accompanied by autoimmune inflammatory processes in the myocardium, leading to necrosis of cardiomyocytes;
- secondary infiltrative cardiopathy is deposits of abnormal substances that cause wall rigidity and dystolic dysfunction.
Publications in the media
Hypertrophic cardiomyopathy (HCM) is a primary lesion of the heart, characterized by thickening of the walls of the left ventricle and the development of heart failure, predominantly diastolic • Hypertrophy of the left ventricular wall of more than 15 mm of unknown origin is considered a diagnostic criterion for HCM • The following options are distinguished •• Symmetrical HCM (enlargement involving all walls left ventricle) •• Asymmetric HCM (hypertrophy involving one of the walls): ••• apical HCM (hypertrophy covers only the apex of the heart in isolation) ••• obstructive HCM (interventricular septum or idiopathic hypertrophic subaortic stenosis ••• HCM of the LV free wall.
Important general features of HCM (both with and without obstruction) are a high frequency of cardiac arrhythmias, primarily ventricular extrasystole and paroxysmal tachycardia, and impaired diastolic filling of the left ventricle, which can lead to heart failure. Arrhythmias are associated with sudden death, which occurs in 50% of patients with HCM.
Statistical data. HCM is observed in 0.2% of the population, most often it is non-obstructive HCM (70-80%), less often - obstructive (20-30%, in the form of idiopathic hypertrophic muscular subaortic stenosis). Men get sick more often than women. The incidence is 3 cases per 100,000 people per year.
Etiology • Many HCM are hereditary diseases resulting from mutations in genes encoding myocardial contractile proteins. Familial hypertrophic cardiomyopathy: • type 1: 192600, MYH7, CMH1, 160760 (cardiac myosin, heavy chain b7), 14q12; • type 2: 115195, TNNT2, CMH2, 191045 (cardiac troponin 2), 1q32; • type 3: 115196, TPM1, CMH3, 191010 (tropomyosin cardiac 1), 15q22; •; type 4: 115197, MYBPC, CMH4, 600958 (myosin binding protein C), 11p11.2; • type 7: TNNI3, 191044 (cardiac troponin I), 19p13.2 q13.2; • with Wolff Parkinson-White syndrome: CMH6, 600858, 7q3
Pathogenesis. As a result of gene mutations, left ventricular hypertrophy and areas of cardiomyocyte disorganization occur.
• An increase in the content of calcium ions in cardiomyocytes and pathological stimulation of the sympathetic nervous system are important.
• Abnormally thickened intramural arteries do not have the ability to adequately dilate, which leads to ischemia, myocardial fibrosis and pathological hypertrophy.
• With asymmetric hypertrophy of the interventricular septum, according to the latest data, the obstruction is associated mainly with the abnormal forward movement of the anterior mitral valve leaflet into systole and, to a lesser extent, with septal hypertrophy (obstruction of the outflow tract of the left ventricle - muscular subaortic stenosis: the left ventricle is “divided” into two parts: a relatively small subaortic and a large apical; during the period of expulsion, a pressure difference occurs between them).
• Due to the presence of obstructions to normal blood flow, the pressure gradient between the left ventricle and the aorta increases, which leads to an increase in end-diastolic pressure in the left ventricle. Most patients have abnormal left ventricular systolic function.
• Regardless of the pressure gradient between the left ventricle and the aorta, patients with HCM have impaired left ventricular diastolic function, leading to increased end-diastolic pressure, increased pulmonary capillary wedge pressure, pulmonary congestion, left atrial dilatation, and atrial fibrillation. The development of diastolic dysfunction is associated with a decrease in compliance and impaired relaxation of the left ventricle •• Decreased compliance occurs due to increased muscle mass, a decrease in the left ventricular cavity and a decrease in myocardial compliance due to its fibrosis •• Deterioration of relaxation is the result of systolic (incomplete emptying of the left ventricle due to outflow tract obstruction) and diastolic (decreased ventricular filling) disorders.
• HCM in some cases is accompanied by myocardial ischemia, which is associated with the following reasons •• Reduced vasodilator reserve of the coronary arteries •• Abnormal structure of the intramural arteries of the heart •• Increased myocardial oxygen demand (increased muscle mass) •• Compression during systole of the arteries passing through the thicker myocardium •• Increased diastolic filling pressure •• In addition to the above reasons, 15–20% of patients experience concomitant atherosclerosis of the coronary arteries.
Pathomorphology • Macroscopic examination •• The main morphological manifestation of HCM is thickening of the walls of the left ventricle over 30 mm (sometimes up to 60 mm) in combination with normal or reduced dimensions of its cavity •• Dilatation of the left atrium (occurs due to increased end-diastolic pressure in the left ventricle ) •• In most patients, the interventricular septum and most of the lateral wall of the left ventricle are hypertrophied, while the posterior wall is less often involved in the process. In other patients, only the interventricular septum hypertrophies. In 30% of patients there may be local hypertrophy of the wall of the left ventricle of small sizes: the apex of the left ventricle (apical), only the posterior wall, the anterolateral wall. In 30% of patients, the right ventricle, papillary muscles or apex of the heart are involved in the hypertrophic process • Microscopic examination •• Disorderly arrangement of cardiomyocytes, replacement of muscle tissue with fibrous tissue, abnormal intramural coronary arteries •• The presence of disordered hypertrophy, characterized by multidirectional arrangement of myofibrils and unusual connections between neighboring myocardial cells •• Foci of fibrosis are represented by randomly intertwined bundles of coarse collagen fibers.
Clinical manifestations are caused by obstruction of the left ventricular outflow tract, its diastolic dysfunction, myocardial ischemia and cardiac arrhythmias
• Sudden cardiac death is possible, most cases (80%) resulting from ventricular fibrillation. Other causes of sudden cardiac death include atrial fibrillation with a high ventricular rate, supraventricular tachycardia, and a sharp decrease in cardiac output with the development of shock. Risk factors for sudden cardiac death in HCM include the following •• History of cardiac arrest •• Persistent ventricular tachycardia •• Severe left ventricular hypertrophy •• Genotype features (see Etiology) or family history of sudden cardiac death •• Frequent paroxysms of ventricular tachycardia, detected by daily ECG monitoring •• Early appearance of symptoms of HCM (in childhood) •• Frequent fainting •• Abnormal response of blood pressure to physical activity (decrease).
• Complaints •• The disease can be asymptomatic for a long time, and it is accidentally detected during examination for another reason •• Shortness of breath as a result of an increase in diastolic filling pressure of the left ventricle and a passive retrograde increase in pressure in the pulmonary veins, which leads to impaired gas exchange. An increase in left ventricular filling pressure is due to worsening diastolic relaxation due to severe hypertrophy •• Dizziness and fainting during exercise as a result of worsening cerebral circulation due to worsening obstruction of the left ventricular outflow tract. Also, episodes of loss of consciousness can be caused by arrhythmias •• Chest pain due to worsening diastolic relaxation and increased myocardial oxygen demand as a result of hypertrophy. Typical attacks of angina pectoris may occur, the causes of which are a discrepancy between the coronary blood flow and the increased oxygen demand of the hypertrophied myocardium, compression of the intramural branches of the coronary arteries by subendocardial ischemia as a result of impaired diastolic relaxation •• Palpitations can be a manifestation of supraventricular or ventricular tachycardia, atrial fibrillation.
• Upon examination, there may be no external manifestations of the disease. In the presence of severe heart failure, cyanosis is detected. HCM can be combined with arterial hypertension.
• Palpation can reveal a double apical impulse (contraction of the left atrium and left ventricle) and systolic tremor at the left edge of the sternum.
• Auscultation of the heart •• Heart sounds are usually not changed, although there may be a paradoxical splitting of the second tone with a significant pressure gradient between the left ventricle and the aorta •• The main auscultatory manifestation of HCM with obstruction of the outflow tract of the left ventricle is systolic murmur ••• The occurrence of systolic murmur is associated with the presence of an intraventricular pressure gradient between the left ventricle and the aorta and mitral regurgitation (reflux of blood into the left atrium as a result of prolapse of one of the mitral valve leaflets due to excess pressure in the left ventricle) ••• The murmur has a waxing-waning character and is better heard between the apex of the heart and the left edge of the sternum. It may radiate to the axillary region ••• The murmur decreases (due to decreased obstruction of the left ventricular outflow tract) with decreased myocardial contractility (for example, due to the use of beta-blockers), an increase in left ventricular volume, or an increase in blood pressure (for example, in the squatting position, taking vasoconstrictors) ••• The murmur increases (due to increased obstruction) as a result of increased contractility (for example, during physical activity), a decrease in left ventricular volume, a decrease in blood pressure (for example, with the Valsalva maneuver, taking antihypertensive drugs, nitrates).
Instrumental data
• ECG changes in HCM are detected in 90% of patients •• Main ECG signs: left ventricular hypertrophy, changes in the ST segment and T wave, the presence of pathological Q waves (in leads II, III, aVF, chest leads), atrial fibrillation and flutter , ventricular extrasystole, shortening of the P–R (P–Q) interval, incomplete blockade of the His bundle branches. The causes of pathological Q waves are unknown. They are associated with myocardial ischemia, abnormal activation of the interventricular septum, imbalance of the resulting electrical vectors of the interventricular septum and the wall of the right ventricle •• Less commonly, ventricular tachycardia and atrial fibrillation are recorded on the ECG in patients with HCM •• With apical cardiomyopathy, “giant” negative T waves often occur ( depth more than 10 mm) in the chest leads.
• Daily ECG monitoring: supraventricular arrhythmias are detected in 25–50% of patients with HCM, ventricular tachycardia is detected in 25% of patients.
• EchoCG is the main method for diagnosing this disease •• Determine the localization of hypertrophied areas of the myocardium, the severity of hypertrophy, and the presence of obstruction of the outflow tract of the left ventricle. Asymmetric hypertrophy is detected in 60%, symmetric in 30%, apical in 10% •• In Doppler mode, the severity of mitral regurgitation and the degree of pressure gradient between the left ventricle and the aorta are determined (a pressure gradient of more than 50 mm Hg is considered pronounced). In addition, Doppler can also detect concomitant mild or moderate aortic regurgitation in 30% of patients with HCM •• In 80% of patients, signs of left ventricular diastolic dysfunction can be detected •• Left ventricular ejection fraction may be increased •• Signs of HCM also include • •• small size of the cavity of the left ventricle ••• dilatation of the left atrium ••• reduced amplitude of movement of the interventricular septum with normal or increased movement of the posterior wall of the left ventricle ••• mid-systolic closure of the aortic valve leaflets •• The following are considered signs of obstructive HCM ••• Asymmetric hypertrophy of the interventricular septum with a ratio of its thickness to the thickness of the posterior wall of the left ventricle more than 1.3:1 (and the thickness of the interventricular septum should be 4–6 mm greater than normal for this age group) ••• Systolic movement of the anterior leaflet of the mitral valve forward.
• X-ray examination: the contours of the heart may be normal. With a significant increase in pressure in the pulmonary artery, bulging of its trunk and expansion of its branches are noted.
Diagnostics. The main diagnostic method is echocardiography, which allows to detect myocardial thickening and assess the presence of obstruction of the left ventricular outflow tract. Before diagnosing HCM, it is necessary to exclude causes of secondary hypertrophy, incl. acquired and congenital heart defects, arterial hypertension, coronary artery disease, etc.
Differential diagnosis • Other forms of cardiomyopathy • Aortic stenosis • Mitral valve insufficiency • IHD.
TREATMENT
General recommendations. In case of HCM (especially in the obstructive form), it is recommended to avoid significant physical activity, since this may increase the pressure gradient between the left ventricle and the aorta, causing cardiac arrhythmias and fainting.
Drug therapy • For asymptomatic HCM, it is possible to prescribe b-blockers (from 40 to 240 mg/day propranolol, 100–200 mg/day atenolol or metoprolol) or slow calcium channel blockers (verapamil at a dose of 120–360 mg/day), although this issue still remains controversial • In the presence of moderately severe symptoms, either b-blockers are prescribed (propranolol in a dose of 40 to 240 mg/day, atenolol or metoprolol in a dose of 100–200 mg/day) or slow calcium channel blockers (verapamil in dose 120–360 mg/day). They decrease heart rate and prolong diastole, increase passive left ventricular filling, and decrease filling pressure. Similar therapy is also indicated for atrial fibrillation. In addition, due to the high risk of thromboembolism in atrial fibrillation, patients should be prescribed anticoagulants • For severe symptoms of HCM, in addition to b-blockers or verapamil, diuretics are prescribed (for example, hydrochlorothiazide at a dose of 25–50 mg/day) • For obstructive HCM the use of cardiac glycosides, nitrates, and adrenergic agonists should be avoided • In obstructive HCM, it is necessary to prevent infective endocarditis, since vegetations may appear on the anterior leaflet of the mitral valve as a result of its constant trauma.
Surgery. Surgical treatment is carried out for the obstructive form of HCM with a pressure gradient between the left ventricle and the aorta of more than 50 mm Hg. In this case, septal myotomy-myectomy (Morrow operation) is performed. In the presence of frequent paroxysms of ventricular tachycardia, they resort to implantation of a cardioverter-defibrillator.
The course is variable. In most patients, the disease is relatively stable or even tends to improve (in 5–10% over 5–20 years). Women with HCM usually tolerate pregnancy well. With a long course of the disease, the development of heart failure is increasingly observed.
Prognosis • Without treatment, the mortality rate of patients with HCM is 2–4% per year • Patients with more than one risk factor for sudden cardiac death are classified as a high-risk group • In 5–10% of patients, spontaneous reverse development of hypertrophy is possible • In 10%, the transition to hypertrophic cardiomyopathy into dilated cardiomyopathy • In 5–10% of patients, a complication develops in the form of infective endocarditis.
Concomitant pathology • Arrhythmias • Systemic arterial hypertension • Aortic stenosis • IHD.
Reduction. HCM is hypertrophic cardiomyopathy.
ICD-10 • I42.1 Obstructive hypertrophic cardiomyopathy • I42.2 Other hypertrophic cardiomyopathy.
Causes
The causes of heart disease can be of various natures, endogenous and exogenous. The greatest influence is:
- transferred infectious myocarditis , including the influence of enteroviruses, borrelia, hepatitis C virus, Coxsackie, HIV , as well as bacteria, viruses, fungi and even protozoa - Chagas disease ;
- exposure to toxic agents and accumulation of abnormal substrates;
- endocrine system disorders (lack or excess of thyroid hormones, pituitary gland dysfunction, diabetes mellitus , development of pheochromacytoma );
- suffered a heart attack ;
- cardiosclerosis – replacement of muscle fibers with connective tissues;
- poor nutrition - lack of selenium , carnitine ;
- autoimmune reactions, for example, with systemic lupus erythematosus , scleroderma , rheumatoid arthritis ;
- genetic factors - the occurrence of mutations in genes encoding the synthesis of cardiac sarcomere proteins.
Tests and diagnostics
To assess the state of the cardiovascular system, the following examinations are carried out:
- Electrocardiogram , which shows the electrical activity of the heart, the frequency and rhythm of contractions.
- Echocardiography or ultrasound of the heart makes it possible to see all the structural features and movements of structures.
- Scintigraphy allows you to assess the level of blood supply to the myocardium, detect necrotic areas, and understand the risk of complications.
- Load tests – as a result of a bicycle ergometer test , you can evaluate the functionality of the heart under conditions of increasing load.
- Magnetic resonance imaging, as the most modern method, allows you to obtain images of the heart in various planes and in high definition, as well as assess the speed of blood flow and see the features of its functioning.
Complications
Cardiomyopathy carries a high risk of complications. There are disturbances in the functioning of the heart and lungs. Common complications of cardiomyopathy:
- myocardial infarction;
- acute or chronic heart failure;
- pulmonary embolism (PE);
- pulmonary edema;
- arrhythmia;
- endocarditis;
- sudden cardiac arrest;
- stroke.
Chronic heart failure develops in the vast majority. As the disease progresses, irreversible changes occur that lead to the death of the patient.
The risk of developing complications can be reduced if cardiomyopathy is treated promptly and its main complications are prevented. Therefore, relatives of patients suffering from various forms of cardiomyopathy need to know the main symptoms of these conditions.
| Complications | Symptoms |
| Myocardial infarction | It manifests itself as a sharp pain in the sternum (“dagger” pain), radiating to the left arm, under the shoulder blade and into the lower jaw. The pain syndrome is accompanied by a feeling of fear, sticky cold sweat, and changes in pulse. |
| Heart failure | With the development of cardiomyopathy, acute and chronic heart failure occurs. Acute failure manifests itself in the form of cardiogenic shock, with severe hemodynamic disturbances. Atrial fibrillation develops, the person loses consciousness, and cardiac arrest occurs. Chronic heart failure lasts a long time, symptoms increase gradually. It is manifested by shortness of breath at rest, edema of the lower extremities, cyanosis of the skin, breathing problems and cough. |
| Endocarditis | It is an inflammation of the inner surface of the heart. Manifested by sharp pain in the chest, increased body temperature, fatigue, tachycardia, edema, changes in heart rhythm, cardiac murmurs on auscultation. |
| Pulmonary edema | There is noisy breathing with moist rales (“gurgling”), and the release of copious foamy sputum. This is an emergency and requires immediate medical attention. |
| Stroke | As a complication of cardiomyopathy, stroke occurs quite often and is accompanied by severe headache, loss of orientation in space, paralysis of the limbs (usually on one side), disturbances of speech and consciousness. |
| Arrhythmia | There is a change in heart rate, a feeling of “interruptions” in the work of the heart, shortness of breath, dizziness, and possible loss of consciousness. |
| Sudden cardiac arrest | Sudden cardiac arrest is more common in hypertrophic cardiomyopathy. It develops more often against the background of loss of consciousness in young patients. The person loses consciousness, cardiac activity and breathing stop. Urgent resuscitation measures are required (indirect cardiac massage at the first aid stage). |
| Pulmonary embolism | Accompanied by cough, chest pain, and breathing discomfort. Erased symptoms of cardiomyopathy in the form of a rare dry cough and increased body temperature are possible. |
Prevention
To prevent the development of cardiopathy it is necessary:
- quit smoking, alcohol and drugs;
- regularly undergo a complete health examination;
- do not take medications randomly and do not self-medicate;
- control weight;
- avoid psychological stress;
- adhere to proper nutrition;
- normalize physical activity and rest - at least an hour of walking and eight hours of sleep.
Symptoms of cardiomyopathies
The severity of symptoms depends on the type of pathology and concomitant diseases.
It is customary to identify the following general symptoms for cardiomyopathies:
- heart pain;
- fast fatiguability;
- shortness of breath during physical activity and at rest;
- increased shortness of breath in a horizontal position;
- swelling of the lower extremities;
- cough;
- dizziness;
- change in heart rate;
- fainting.
Symptoms of hypertrophic cardiomyopathy
Hypertrophic cardiomyopathy is diagnosed between the ages of 20 and 45 years. Symptoms of cardiomyopathy may resemble angina or hypotension.
The main symptoms of hypertrophic cardiomyopathy:
- discomfort in the sternum (reminiscent of an angina attack);
- shortness of breath on exertion;
- severe fatigue;
- pronounced pulsation of the carotid arteries.
- short-term episodes of loss of consciousness.
Fatigue in this form is not expressed, as are changes in the venous pattern in the neck. An alarming symptom of cardiomyopathy is frequent episodes of fainting. Because this phenomenon increases the risk of sudden death. But sometimes hypertrophic cardiomyopathy is completely asymptomatic.
Symptoms of dilated cardiomyopathy
About half of the total number of patients with dilated cardiomyopathy do not have any symptoms. Atypical pain in the heart area may be observed.
As dilated cardiomyopathy progresses, symptoms increase. The following symptoms of cardiomyopathy are observed:
- pain in the left half of the chest;
- shortness of breath on exertion;
- severe fatigue;
- swelling of the lower extremities;
- pallor of the skin (and as the disease progresses, cyanosis occurs).
In addition, more patients develop a pronounced venous pattern in the neck. Dilated cardiomyopathy is dangerous due to the development of ventricular arrhythmias, which can cause death.
Symptoms of restrictive cardiomyopathy
Symptoms of restrictive cardiomyopathy are nonspecific and can masquerade as other diseases of the cardiovascular system. Therefore, diagnostic difficulties arise; restrictive cardiomyopathy is often detected at a late stage. The main symptoms include:
- shortness of breath during exercise;
- shortness of breath in a horizontal position, decreasing in the sitting position;
- breathing disorder during sleep;
- swelling (usually in the lower extremities);
- fatigue;
- expansion of the venous pattern in the neck;
- arrhythmic pulse;
- discomfort in the left side of the heart (rare);
- loss of consciousness (rare).
As the disease progresses, congestion in the lungs develops, which can manifest itself as a persistent cough.
Cardiopathy in children
Heart problems in children are usually primary - genetic problems or congenital defects, because most protect their children from the negative influences of the outside world and serious illnesses.
Congenital cardiovascular pathology may not make itself felt from the first days; problems usually appear during active games or physical activity. Therefore, it is very important to identify the pathology as early as possible and protect the child by freeing him from physical education and sports, because what functional cardiopathy is in children becomes clear immediately - children get tired quickly, they have pale skin, severe shortness of breath, even panic attacks and fainting are possible. But all this is just the tip of the iceberg and cardiac dysfunction can worsen and progress.
Secondary cardiopathy in children is a complication of a primary disease - endocrine, infectious, infiltration, neuromuscular, etc. Myocardial lesions usually lead to irreversible morphological changes, which can cause disability and even death.
Cardiomyopathy in pregnant women
Cardiomyopathy can develop during pregnancy. This is due to increased load on the heart muscle, hormonal changes, and stress to the body during childbirth.
Complications during this period play an important role in the occurrence of cardiomyopathy during pregnancy. For example, gestosis in the second half of pregnancy. When it occurs, disturbances occur in all vital organs and not only in the kidneys and nervous system, but also in the heart.
In addition, gestosis increases blood pressure and increases the load on the heart.
Cardiomyopathy during pregnancy occurs in the third trimester. And it can persist into the postpartum period. Or this pathological condition occurs after childbirth.
In pregnant women, the most common are hypertrophic and dilated cardiomyopathies. They are accompanied by the following symptoms:
- increased shortness of breath;
- increased shortness of breath at rest;
- change in color of the nasolabial triangle (it becomes pale with the addition of cyanosis);
- increased blood pressure;
- increased swelling;
- change in fetal activity.
If cardiomyopathy was diagnosed during pregnancy, then, as prescribed by the doctor, the disorders are corrected with the help of medications in individual dosages.
Delivery of women with cardiomyopathy is carried out by cesarean section. As a maternity hospital, it is necessary to choose a specialized center for women in labor with cardiac pathology. If cardiomyopathy is detected in the postpartum period, then standard therapy with medications is carried out. The prognosis is more favorable than with other variants of the disease.
Is it possible to plan a pregnancy with cardiomyopathy?
Cardiomyopathy in women is associated with a high risk of complications during pregnancy. Therefore, the feasibility of planning depends on many factors. It is necessary to take into account the severity of cardiac dysfunction, the age of the mother, and whether there is a risk of heart failure.
For women with severe forms of cardiomyopathy, pregnancy is not recommended, because there is a high probability of severe consequences during pregnancy and directly during childbirth. Moreover, the degree of risk is high for both the health and life of the mother and the child. Preparing for pregnancy in patients with heart disease should be carried out not only with a gynecologist, but also with a cardiologist.
Diet for cardiopathy
Diet for heart failure
- Efficacy: therapeutic effect after 20 days
- Timing: constantly
- Cost of products: 1700-1800 rubles. in Week
For people with heart problems, a healthy diet is first recommended. To begin with, your diet should be dominated by foods that are gentle on the cardiac system:
- cereals and whole grain baked goods, high in dietary fiber, which help lower cholesterol ;
- vegetable and legume dishes are the basis of the diet, providing the body with vitamins and microelements;
- sweet berry and fruit snacks are an excellent replacement for synthetic sugar, which causes obesity and diabetes mellitus - the main diseases at risk for cardiovascular system disorders;
- dairy products, seafood and other complete animal proteins with limited consumption of fatty meats;
- enriching the menu with healthy fats - nuts, seeds;
- reducing salt intake to 5 mg per day.
Then you need to establish a strict regime and portion sizes, refuse fried, smoked and pickled foods.
Treatment of cardiomyopathy
Treatment of cardiomyopathy is aimed at relieving the cause of the disease, alleviating symptoms, and preventing complications.
Each type of treatment for cardiomyopathy has its own protocol. Non-drug treatment of cardiomyopathy, drug tactics, and surgical intervention are used.
Drug treatment of dilated cardiomyopathy consists of the use of medications and is used in most patients.
Surgical treatment of cardiomyopathy is carried out in case of ineffectiveness of conservative measures or for health reasons.
Along with these therapeutic measures, non-drug methods are used, which consist of changing work and rest schedules and changing diet.
Drug treatment
The choice of drug treatment for cardiomyopathy depends on its cause. For infectious inflammation of the myocardium, antibacterial therapy is carried out with the addition of anti-inflammatory drugs.
If the etiological factor is an autoimmune process, then treatment of cardiomyopathy with hormonal drugs (prednisolone).
If other diseases are detected, their etiotropic therapy is carried out. In all other cases, treatment is aimed at maintaining the myocardium, correcting disorders and restoring cardiac function.
| Kinds | Treatment of cardiomyopathy |
| Hypertrophic cardiomyopathy |
|
| Dilated cardiomyopathy |
|
| Restrictive cardiomyopathy |
|
Surgery
Surgical treatment of cardiomyopathy is carried out exclusively for health reasons and only in some of its forms. Heart surgery is a serious burden on the body and requires a long recovery. Therefore, surgery is not used in all patients.
This treatment is used in patients with hypertrophic cardiomyopathy. The following methods are used:
- septal myectomy;
- reconstruction of heart valves;
- valve apparatus prosthetics;
- percutaneous transluminal alcohol ablation with installation of a pacemaker;
- installation of a mini-defibrillator;
- heart transplant.
The essence of septal myectomy is to remove hypertrophied areas of the heart muscle. Used for hypertrophic cardiomyopathy. It is performed using general anesthesia, since this is an abdominal operation.
Percutaneous transluminal alcohol ablation is a minimally invasive surgical procedure. It involves inserting a thin catheter. Through it, alcohol is injected into the affected area, which promotes ischemia and scar formation. After which the ischemic area is removed.
If the patient has abnormal heart rhythms, it may be necessary to install a pacemaker, and in some cases, a defibrillator. Such devices help improve cardiac conduction and provide protection against sudden arrhythmias.
In severe cases, a heart transplant may be required. Indications include severe forms of dilated and restrictive cardiomyopathy. But such an intervention has a number of contraindications and side effects.
But the main problem is finding a suitable donor and the complexity of the operation.
The search for a suitable donor can take a long time. While providing medical care is necessary as early as possible.
In addition, to carry out this operation, a specialized medical center and equipment, as well as specialist doctors, are required.
If a heart transplant has been performed, the patient will have a long recovery period, take special medications and follow all doctor’s recommendations.
Non-drug treatment recommendations
Non-drug treatment methods include observing work and rest, avoiding physical activity and stress. An important factor is proper nutrition and taking vitamins.
A patient with cardiomyopathy must maintain a normal work and rest schedule, not overexert, and get full sleep (at least 8 hours).
Physical activity is reduced, paying attention to breathing exercises, which are not contraindicated for patients. And also when the condition normalizes, walks in the fresh air are recommended.
Physical activity needs to be restored gradually, and in addition, in some cases, bed rest is indicated.
What patients with cardiomyopathy should not do:
- run;
- lift weights;
- visit the sauna and steam bath;
- engage in heavy physical activity;
- attend massage sessions.
Are traditional methods of treatment effective?
Traditional medicine recipes should be used with caution in patients suffering from cardiomyopathy. And, of course, they should not replace drug therapy or surgery.
Alternative treatment for cardiomyopathy should complement medications and be used only with the permission of the attending physician. Since the advisability of taking it is directly related to the patient’s condition and the severity of the disease.
Various decoctions and infusions of medicinal herbs are widely used as an additional treatment for cardiomyopathy. They are taken for a long time, in small dosages, but regularly.
Collections of motherwort, viburnum, nettle and valerian are recommended. These components have a beneficial effect on the condition of the heart muscle, protecting it.
| Traditional treatment of cardiomyopathy | Cooking method |
| Infusion of valerian root and mint leaves | To prepare, take 4 tablespoons of crushed valerian root and 3 tablespoons of mint leaves. All ingredients are mixed, pour 300 ml of boiling water. Then leave for 2-3 hours. Take ¼ cup 2 |
| Infusion of nettle and motherwort | You need to take 2 tablespoons of chopped nettle and 1 tablespoon of motherwort. Mix everything and pour 200 ml of boiling water. Let it brew, strain. Drink ½ glass. |
| Infusion of viburnum fruits | Wash and dry the viburnum fruits well. Pour boiling water over and let steep for 1 hour. Then strain through cheesecloth. It is recommended to take ½ glass 2 times a day. |
| Infusion of medicinal motherwort | To prepare the product, you need to take 3 tablespoons of medicinal motherwort and add 200 ml of hot water. Let it brew for 1-2 hours. Take ½ glass 2 times a day. |
| A decoction of valerian and motherwort roots | Place the crushed roots of valerian and motherwort in a saucepan and bring to a boil. Boil after boiling for 20-25 minutes, strain. Let it brew for 1 hour. Drink ¼ cup 2 times a day. |
| Rosehip decoction | Rinse the rose hips and add to boiling water. Boil after boiling for 15 minutes. Then strain and let it brew. Drink half a glass 3 times a day. |
Diet
The diet of patients with dilated cardiomyopathy should be balanced and contain the required amount of vitamins and minerals.
It is recommended to eat small portions often (5-6 times a day). This will help you avoid overeating, control your weight, and reduce chest pain.
It is recommended to include the following products in your diet:
- lean meats and fish;
- dairy products;
- fresh fruits and vegetables;
- dried fruits (dried apricots, figs).
It is necessary to limit salt and liquid intake. Because this contributes to the appearance of edema and increased stress on the heart muscle.
It is also recommended to exclude the following products:
- fatty foods, salty and spicy;
- strong coffee and tea;
- soda;
- alcohol.
It is recommended to steam, stew or bake food with a minimum amount of oil.