Defects in the development of cardiac structures are encountered in the practice of medical specialists in the vast majority of cases.
Relatively rarely (25-30% of all recorded situations) they are congenital. Most often acquired. Many could have been avoided if the patient had consulted a doctor earlier.
Left atrium hypertrophy is an increase in its volume as a result of overload and thickening of the muscle layer. The pathology is associated with a minimal clinical picture in the early stages of development.
As the symptoms progress, they become obvious, but even in this case, only diagnostics can answer the question of the origin of the phenomenon.
Mortality is relatively low and amounts to 3-5% over a period of almost 8 years (data from European associations of cardiology). This does not mean that treatment should be taken lightly. The development of the condition is associated with an increase in the risk of death at a rapid pace.
Hypertrophy is not primary. In the sense that it always develops as a result of a third-party disease: the heart, endocrine, nervous system, blood vessels. Recovery is about eliminating the root cause.
Development mechanism
Left atrial hypertrophy (abbreviated as LHA) is an independent pathological process. It is similar in nature and typical features to cardiomyopathy. The development of the defect occurs in two main ways.
Normally, a muscular organ pumps the volume of blood that enters it. Adequate load leads to the complete release of liquid connective tissue from the chambers. Hence the stable operation of the structures.
If a failure occurs, the atria and/or ventricles are filled to capacity, resulting in an inability to discharge normally. Hence the overstretching of all chambers or dilatation, in other words.
This situation is most typical for professional athletes or persons suffering from congenital or acquired defects.
Another possibility is that blood returns to the left atrium from the ventricle due to mitral valve stenosis or prolapse.
The second pathogenetic mechanism concerns overload of the muscle layer - the myocardium. A similar phenomenon occurs as a result of a long course of third-party pathologies.
The main one is hypertension with numbers above 160 by 90 mmHg. The same effect is provoked by diseases of the lungs and excretory system.
Several factors may be influencing at once. Then mixed hypertrophy develops, which is difficult to treat with standard methods.
Classification
Some typifications have clinical significance.
Based on the moment of development
- Congenital appearance. Caused by disorders of the prenatal period or genetic mutations (including spontaneous ones).
In the latter case, a complex violation of anatomical structures occurs. Not only the left atrium is affected, but also the ventricles.
In addition, cosmetic defects, pathologies of the maxillofacial area and others are possible. Depends on the syndrome.
- Acquired type. Occurs more often. Develops in patients who abuse alcohol and smokers. Also during the course of hypertension and third-party defects of cardiac structures. In the early stages it is treatable, but later it becomes difficult. Complete impossibility of therapy in the final phase.
According to anatomical properties
Symmetrical view of the GLP. Left atrial hypertrophy is characterized by thickening of the myocardium at the affected sites. Moreover, along the entire length of the structure, the increase may be different.
The nature of the deviation is assessed using the so-called asymmetry index. In this case, the growth of the muscle layer is uniform, the indicator is within 1.3.
The treatment is standard and consists of stopping the root cause, that is, the main pathology. Symptoms are minimal, making early diagnosis difficult.
Asymmetrical type. The index of the same name is over 1.3, which indicates uneven growth of the myocardium within the atrium. Evidence in favor of a possible congenital developmental disorder.
By stages of formation
- Enlargement of the left atrium in compensation. The first phase of the development of the disease. Symptoms are completely absent; the echocardiogram shows minor or no abnormalities.
No recovery required. Dynamic observation under the supervision of a specialized specialist is indicated.
- Subcompensation. Second stage. It develops as a result of a long course of the main pathological process. At the same time, the deviation itself is minimally expressed.
Symptoms are present, but they are nonspecific: chest pain, rare episodes of tachycardia, fatigue, increased fatigue, short periods of shortness of breath after intense physical activity.
Treatment is required; inpatient therapy is possible at this stage. There is no longer any need to wait for independent regression.
- Decompensation. In some classifications it is the final stage, which is not entirely true. The clinical picture is pronounced. Accompanied by cardiac symptoms, as well as manifestations from the cerebral structures and excretory tract.
Treatment is urgent, in a hospital. The process is accompanied by severe heart failure, death can occur at any time, the risks are high.
- Terminal phase. Extreme degree of violation. Cannot be corrected in principle. The approximate period from the beginning of myocardial growth to the formation of the final state is 3-10 years. It happens more, depending on the endurance of the body. Palliative care, for relief. The count goes on for weeks, rarely months.
Classifications, especially staging, are used to develop therapeutic tactics and determine the diagnostic vector.
Treatment
When HLP appears, heavy physical activity is contraindicated. It is necessary to give up smoking and drinking alcohol, as well as strong tea, coffee, and tonic drinks. Dietary restrictions on salt and saturated fat are recommended. It will not be superfluous to eat foods rich in potassium (dried apricots, bananas, baked potatoes). You can also use folk remedies to maintain myocardial metabolism: the fruits of hawthorn, rowan, viburnum, honey. Walking in the fresh air helps improve the functional state of the myocardium. To reduce anxiety and stress, your doctor may recommend taking herbal sedatives. GLP has no specific treatment. Treatment is carried out for the disease that was its cause. For heart defects, surgical treatment is possible. Hypertension and coronary heart disease are treated according to appropriate standards. Treatment for pulmonary hypertension includes medications and inhaled nitric oxide. In cases of severe heart failure, heart transplantation may be indicated.
Causes
Development factors are mainly pathological. There is one exception to the rule.
Intense physical activity
This is not about simple activity, but about activity at the limit of the body’s capabilities. These are mostly professional athletes, fanatically enthusiastic amateurs.
If the left atrium is enlarged (this happens sooner or later), dynamic monitoring under the supervision of a cardiologist is indicated. Rapid progression is grounds for lifelong withdrawal from sports.
What happens when you overexert yourself? Muscles require an intensive supply of oxygen and nutrients. The body intensifies its work. The chambers are overflowing with blood. Hence the dilatation, expansion of the atrium.
On the other hand, the myocardium is forced to function faster, contract more often and more strongly. Hypertrophy - building muscle mass. This is an adaptive mechanism.
Chronic obstructive disease, bronchitis, asthma
And other respiratory pathologies. Associated with impaired supply of cardiac structures with oxygen and nutrients. The result is ischemia.
False growth of the myocardium is possible, when in fact it is not new muscle tissue that is formed, but scar tissue.
Therapy is very difficult. The described pathologies are in principle incurable. The only chance is to transfer them into a state of long-term high-quality remission, but this also requires a lot of effort.
Renal failure in the decompensation phase
Also pyelonephritis and other conditions that provoke an increase in blood pressure.
In this regard, malignant hypertension is the most aggressive. It quickly “shrinks” the heart, as well as the brain, deprives the patient of vision, and leads to the destruction of blood vessels.
Restoration is urgent. In the specialized department of the hospital. In the later stages, pathologies are poorly eliminated. Therefore, it is recommended to attend to early diagnosis and treatment by a nephrologist.
Read more about what other kidney pathologies increase or decrease blood pressure here.
Arterial hypertension
An extremely complex pathology. It is often very difficult to detect the origin factor of the disease. Because we can talk about a group of reasons.
In some situations, doctors are forced to diagnose the idiopathic form (if the cause remains unclear).
The condition does not require delay in terms of treatment. Relatively quickly, the pathological process stops responding to exposure and becomes resistant to drugs.
The prospects for eliminating left atrial hypertrophy directly depend on success in the fight against hypertension.
Narrowing of the aortic lumen
As a result of a malfunction of the corresponding valve or a congenital defect (coarctation).
Recovery is carried out surgically. Prosthetics or stenting (artificial expansion of the lumen) is possible.
Success depends on the extent of the affected area and the stage of the hypertrophic process. If anatomical disorders are persistent, they cannot be reversed. In the early stages this is not required.
Mitral valve defects
According to the type of prolapse (retraction of the valves into the previous chamber of the heart), also stenosis (up to complete fusion, when blood is not able to move to the left ventricle).
More often it has an acquired origin. Develops after infectious and inflammatory diseases and connective tissue pathologies. Treatment is strictly surgical, using prostheses.
Success depends on the stage of the pathological process. The sooner action is taken, the higher the likelihood of full recovery. It makes sense to act early.
An indirect effect is caused by lipid metabolism disorders. Obesity is considered a consequence, but not a cause. Therefore, calling increased body weight a factor in the development of cardiac problems does not make sense. This is false information.
Why does hypertrophy occur?
Thickening of the heart muscle (myocardium) can occur in any chamber of the heart - in the right or left atrium, as well as in the right or left ventricle. Each of these types has its own causes and consequences. Possible causes of left atrial hypertrophy (LAH) will be discussed below.
hypertrophy of all parts of the heart
So, enlargement of the left atrium in most cases accompanies any of the cardiac diseases. If a patient shows signs of hypertrophy on the ECG, for example, he must be further examined, because left atrial hypertrophy is not a normal variant. The exception is people who have been involved in sports for a long time and professionally, but they develop physiological uniform hypertrophy of all parts of the heart or only the left ventricle (the so-called “athlete’s heart”). Isolated thickening of the left atrium is more typical for cardiac pathology.
Possible diseases in which the left atrium hypertrophies are the following:
Heart defects
Violation of the architectonics of the heart muscle greatly affects its functioning. With defects, compensatory hypertrophy of the heart chambers develops, and subsequently heart failure increases. Enlargement of the left atrium develops with such types of defects as:
- Congenital heart defects, such as bicuspid aortic valve.
- Acquired defects of the mitral valve, which serves as a kind of “door” between the cavities of the atrium and ventricle on the left. During the expulsion of blood from the atrial cavity, the valve flaps open, allowing blood flow to pass through, and during the expulsion of blood further, from the ventricle into the aorta, the valve flaps are tightly closed to avoid the reverse flow of blood. Mitral defects develop as a result of autoimmune or bacterial inflammation in its valves - after acute rheumatic fever (previously called rheumatism), after scarlet fever, as a result of chronic tonsillitis or infective endocarditis. Due to scarring of the valves, narrowing of the valve ring (the defect is called stenosis) or insufficiency of the left atrioventricular orifice (the defect is called insufficiency) develops.
With stenotic narrowing of the aortic valve, it is very difficult for the left atrium muscle to push blood through the narrow opening; naturally, after some time, the atrium wall thickens in order to contract with greater force. But sooner or later decompensation occurs, the atrium cannot work under conditions of constantly high load, and chronic heart failure develops. The speed of development of the process varies among different patients, ranging from several months to decades.
hypertrophy of the left atrium in combination with hypertrophy of the right ventricle with mitral valve insufficiency
With mitral valve insufficiency, the mechanism of hypertrophy is slightly different. Thus, due to the fact that the valve leaflets do not close tightly, a reverse flow of blood occurs from the cavity of the left ventricle into the cavity of the left atrium (regurgitation, which should not normally exist. The walls of the atrium are constantly overstretched. Based on the Frank-Starling law (which states that the more a muscle is stretched, the more force it will contract), one can imagine that the greater the regurgitation, the more the left atrium muscle works.As a result, compensatory hypertrophy develops, which also leads to heart failure.
Arterial hypertension
With vascular spasm that accompanies high blood pressure numbers, the afterload on the heart increases, since the myocardium must make a lot of effort to push the blood flow into the arterial bed. As a result, hypertrophy of the left ventricle develops, and then thickening of the wall of the left atrium.
Cardiomyopathies
The cause of HLP may be cardiomyopathy, characterized by changes in the configuration of the heart due to previous diseases. Often develops in parallel with cardiosclerosis (proliferation of connective, scar tissue) after inflammation (myocarditis) or heart attacks.
CMP can be hypertrophic (with thickening of the walls of the heart), dilated (with expansion of the chambers of the heart and with an increase in the volume of blood in them) and restrictive (with a violation of the ability of the myocardium to relax during cardiac diastole). The mechanism for the development of left atrium enlargement in CMP that involves the left ventricle is slightly different - with hypertrophic and restrictive atrium it is difficult to push blood because more effort is required, and with dilated ventricle the ventricle is so filled and overstretched with blood that the atrium has to work with a very high load.
Symptoms
Signs of left atrial hypertrophy are varied. But they manifest themselves in later stages, starting with subcompensated and further aggravating until the patient is completely disabled.
- Chest pain. Usually of low intensity even in the most pronounced phase of the pathological process. They are detected after physical exertion, stress, an attack of suffocation against the background of pulmonary problems. The nature of the sensation is pressing, pulling or burning.
- Disturbance of normal heart rhythm. According to the type of paroxysms of tachycardia. Attacks occur spontaneously, last from 2 to 20 minutes or more, depending on the form and persistence of changes in the muscle layer of the organ.
Other arrhythmias occur in parallel. Like atrial fibrillation, and then ventricular fibrillation. These are alarm bells and may lead to death.
- Dyspnea. After intense physical activity. The threshold for symptoms to appear in the early stages is high.
As the disease progresses, the condition accompanies the patient constantly, and does not weaken even in complete rest.
The patient is unable to walk or climb stairs; everyday responsibilities fall on his shoulders as a heavy, exorbitant burden. The question of assigning a disability group is raised.
- Impaired consciousness such as frequent, short-duration fainting. Also a worrying sign. It speaks of involvement of the brain and the onset of ischemia of nerve tissue.
- Fast fatiguability. A small incentive is enough. Not necessarily physical. Mental stress is also difficult to bear.
- Cyanosis of the nasolabial triangle. Especially at the time of tachycardia or an attack of acute pain in the chest.
- Paleness of the skin and mucous membranes.
In addition to purely cardiac symptoms, manifestations of the underlying pathological process are added.
A motley clinical picture is emerging that needs to be analyzed point by point. This requires time and sufficient qualifications.
The patient is recommended to consult a doctor if at least one symptom is present.
Symptoms of the disease
Angina is the most common symptom that indicates left ventricular hypertrophy of the heart. As a rule, in the first stages there are no symptoms. With further development of hypertrophy, the patient may develop atrial fibrillation. Often there may be a condition in which the heart freezes and does not beat (this condition provokes loss of consciousness). In some cases, in a person suffering from left ventricular hypertrophy. In this case, severe shortness of breath may occur. Additionally, a number of symptoms are identified:
- unstable blood pressure;
- high blood pressure;
- general weakness, poor health;
- pain in the heart, chest;
- sleep disturbances, arrhythmia, headaches.
The main symptoms of left ventricular hypertrophy are listed above.
Diagnosis of the disease
Only a qualified cardiologist can examine a patient who is suspected of having a disease. The most effective diagnostic method is electrocardiography (ECG). Thanks to this method, a specialist can determine the thickness of the heart muscle. With this disease, the following changes are visible on the ECG:
- increase in teeth SI, V6 and Rv I, III;
- conduction disturbances in the myocardium;
- modifications of the electrical position;
- complete or partial blockade of the His bundle;
- deviation of the average QRS vector to the right or forward.
In addition to the above diagnostic method, the specialist conducts an examination using MRI, chest X-ray or computed tomography. Cardiac MRI in Moscow also allows the specialist to obtain a lot of useful information about the patient’s condition.
Get a free consultation Consultation does not oblige you to anything
Disease prevention
The risk of further development of the disease is reduced by avoiding drinking alcohol, cigarettes, and coffee. With left ventricular hypertrophy, it is recommended to lead a healthy lifestyle, systematically monitor heart function, and also reduce salt intake and reduce the amount of fatty foods in the diet. With this disease, it is necessary to include more vegetables and fresh fruits in the menu.
Diagnostics
It is carried out under the supervision of a cardiologist. As necessary, third-party specialists are involved (pulmonologist and others).
The examination takes place on an outpatient basis, excluding acute conditions:
- Oral questioning of the patient and collection of anamnestic data. Allows you to decide on the further course of action.
- Measurement of blood pressure, heart rate. Both are above the norm. In the acute period, the deviation is especially noticeable.
- Auscultation. Listening to sound. A distinct noise is detected.
Routine techniques provide the necessary vector for further diagnosis:
- Daily monitoring using an automatic tonometer. Records vital signs within 24 hours. The value of the method lies in the possibility of constant monitoring, while the patient is in natural conditions, is not nervous, and is engaged in usual activities.
- Electrocardiography. Assessment of the functional state of cardiac structures. Left atrial hypertrophy has typical features.
- Echocardiography. The main way to identify a pathological process. Visualization makes it possible to determine the stage and nature of the defect.
- MRI if necessary.
Other studies: general blood test, biochemical and hormonal tests, assessment of neurological status, EEG and others. The list may be expanded at the discretion of third-party specialists.
Signs on ECG
There are several typical features:
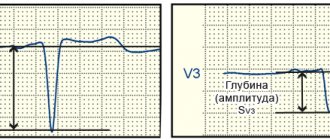
- Changes in the height, shape (“bihump”), and width of the P wave.
- Widening of the QRS complex.
The contraction frequency is normal or increased if the registration of indicators is carried out at the time of an attack of tachycardia.
Other elements are determined by the doctor. In total, there are about 10-15 characteristic features that are difficult for independent perception, much less deciphering.
Signs of left atrial hypertrophy on the ECG are determined by predominant changes in the P wave.
What symptoms can be used to recognize an enlarged left atrium?
There are no strictly specific clinical manifestations of left atrial hypertrophy itself. However, any patient will have those signs that are most characteristic of the causative disease that caused hypertrophy.
Thus, mitral stenosis is characterized by hemoptysis, attacks of dry obsessive cough and shortness of breath with exertion, which increases in the supine position. With mitral valve insufficiency, shortness of breath gradually increases and sensations of interruptions in the work of the heart or rapid heartbeat occur, caused by paroxysmal types of tachycardia (atrial fibrillation, supraventricular tachycardia, frequent ventricular extrasystole). As chronic heart failure progresses, shortness of breath is observed even at rest and with minimal household activity, and swelling of the legs and feet also increases.
A slight increase in the left atrium, caused by arterial hypertension, is accompanied by frequent deterioration with very high blood pressure numbers (180-200 mmHg and above), with frequent crises, difficult to treat with antihypertensive drugs.
If there are any complaints from the cardiovascular system, a consultation with a cardiologist or therapist is necessary for further examination, and the diagnosis of left atrium enlargement is established based on the results obtained.
Treatment methods
Depends on the root cause of the pathological condition. The point is to eliminate the factor of origin. Symptomatic measures are taken in parallel, but do not replace etiotropic effects.
- Arterial hypertension is treated with a group of pharmaceuticals. ACE inhibitors (Perindopril), calcium antagonists (Diltiazem, Verapamil), centrally acting drugs (Moxonidine), beta blockers (Carvedilol, Anaprilin), and diuretics (Veroshpiron).
They are used in combinations, but proper selection is required. Using the wrong regimen will lead to early kidney or heart failure.
- Defects of the aorta or heart valves. Surgery is indicated. Prosthetics, shunting and other methods are most widely used.
- Lung pathologies are eliminated by the use of short courses of corticosteroids, as well as bronchodilators. But with caution. Both of them affect the heart.
Symptomatic therapy:
- Antiarrhythmics to restore an adequate rhythm. Amiodarone. It is also possible to use Anapralin to relieve acute attacks of tachycardia.
- Diuretics for edema of the lower extremities and face.
- Cardioprotectors. Mildronate.
- Nitroglycerin to relieve pain.
Quitting smoking and drinking alcohol in any quantity is mandatory. Don't overexert yourself physically and emotionally.
Diet according to indications. It makes no sense to strictly limit your diet. If there are problems with lipid metabolism, statins are indicated. Sports in case of hypertrophy are contraindicated.
Can left atrial hypertrophy be cured?
The correct treatment strategy is to eliminate the causes that led to thickening of the atrium.
For mitral valve stenosis, cardiac surgery is performed to cut adhesions or replace the valve with a bioprosthesis from a pig heart or, more often, a mechanical prosthesis. In case of isolated valve insufficiency, plasty is performed with suturing of the valve ring. Due to the fact that most often the same patient has a combined defect (both stenosis and insufficiency), it is advisable to treat it by performing an operation to replace an artificial heart valve.
If the cause of hypertrophy is arterial hypertension, the patient is advised to regularly take antihypertensive drugs, and if there is a persistent increase in blood pressure, a combination of drugs from groups with different mechanisms of action is indicated. The most optimal combinations are achieved by constant intake of ACE inhibitors (Prestarium, Diroton, Noliprel) and any of the following groups - diuretics (indapamide, veroshpiron, torsemide) or beta-blockers (carvedilol, concor, coronal) or calcium channel antagonists (amlodipine, verapamil).
Even in the absence of hypertension, a patient with heart disease must take a drug from the group of ACE inhibitors or beta-blockers, since the first group achieves a cardioprotective effect, and the drugs of the second reduce the heart rate, so that the heart muscle experiences less stress.
Complications
Consequences develop in the absence of treatment or with an inappropriate regimen.
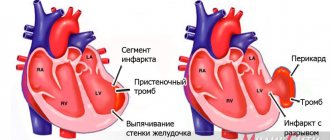
- Heart failure. Often the ambulance is powerless to help the patient.
- Heart attack. Acute death or necrosis of cardiac structures. Leads to tissue scarring; at best, it ends in disability or minor limitations in life.
- Cardiac asthma. Formation of effusion in bronchopulmonary structures.
- Dangerous types of arrhythmias and, as a result, cardiac arrest.
- Stroke.
- Respiratory failure.
Forecast
Determined by the root cause of hypertrophy. Without connection with severe pathologies, death is unlikely and accounts for up to 3-5% of the total mass of clinical cases.
The recovery has good prospects. Without therapy, especially against the background of anatomical changes, the risks grow rapidly. Mortality is determined at 25-40%. The terminal phase guarantees a fatal outcome.
In general, the prognosis is better in the early stages, and the primary pathological process is also taken into account. The possibility of radical treatment and the success of surgery are associated with a better prognosis.
Overload of the left atrium is the main factor of hypertrophy. There are many reasons, the distinction is made within the framework of diagnosis.
Therapy is supervised by a group of specialists. Prospects are not determined immediately; the response to the impact, how long ago the condition is, and other factors play a role.