Home — For the public
- Map of medical organizations
- Vaccination
- Clinical examination
- Fluorography
- Addresses and opening hours of clinics
- Emergency rooms
- Oncology
- Where to take an HIV test
- Healthy child's office
- Services
- Prevention of CVD
- Disease Prevention
- World Patient Safety Day
- Newspaper "Medical News"
- specialist
- School of Health
— Disease prevention
- HIV infection
- All about vaccination
- All about proper nutrition
- Hepatitis
- Flu
- Dementia
- Schoolchildren's health
- STD
- Tick-borne encephalitis
- Whooping cough
- Measles
- Legionellosis
- Meningococcal infection
- Oncology
- Acute intestinal infection
- Pediculosis
- First aid
- Pneumococcal infection
- Pneumonia
- Prevention of rabies
- Dependency Prevention
- Rotavirus infection
- Diabetes
- Cardiovascular diseases
- Injuries
- Tuberculosis
- Tularemia
- Physical activity
- Obstructive pulmonary disease
- Exotic infections
- Ecology
- Why is swimming in ponds dangerous?
— Cardiovascular diseases — Disease of peripheral arteries and veins
Diseases of peripheral vessels and arteries are a group of inflammatory diseases, which in most cases are accompanied by damage to the arteries and veins of the lower (less often, upper) extremities. With these pathologies, a narrowing or significant expansion of the lumen of blood vessels occurs, blood circulation and tissue nutrition in the affected areas are disrupted.
A number of these diseases are caused by atherosclerotic changes in the walls of the arteries, and varicose veins or aneurysms of the aorta and arteries are provoked by pathological overstretching of the venous and arterial walls. The diagnosis is established on the basis of a physical examination and the results of some instrumental studies, which make it possible to visualize the nature of changes in the walls of blood vessels. In severe cases, patients with such diseases may require surgical operations to correct vascular pathology; in milder cases, the resulting disorders can be eliminated conservatively.
Obliterating atherosclerosis
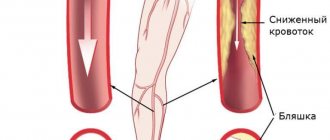
Peripheral artery disease (PAD) in most cases is caused by atherosclerosis, another systemic disease characterized by abnormalities in the structure of the artery walls. Atherosclerotic plaques form in the lumen of the vessels, leading to the settling of blood clots, narrowing of the arterial lumen and the appearance of areas of thrombosis. As a result, the trophism of the tissues surrounding the affected vessels is disrupted, they begin to suffer from ischemia (insufficient blood flow) and the patient develops obliterating atherosclerosis.
Thrombosis usually affects the vessels of the lower extremities at the level of:
- abdominal aorta (Leriche syndrome) – the infrarenal section of the abdominal aorta narrows and blood circulation is impaired in both legs;
- pelvis – the iliac artery is affected;
- hips – the lumen of the femoral artery is blocked;
- shins – blood clots settle in the arteries of the legs and feet.
With significant narrowing of the peripheral arteries of the legs, tissue trophism can be so disrupted that the patient develops trophic ulcers due to constant ischemia and gangrene can develop, leading to the need for amputation of the leg. In addition, atherosclerosis is prone to progression and the patient’s risk of developing myocardial infarction and stroke increases in the future, since both the coronary and carotid arteries are involved in the pathological process.
The process of occurrence and spread of atherosclerotic plaques occurs unnoticed in almost 50% of patients. Often, patients with such pathologies consult a doctor only when conservative treatment methods are not enough to restore blood flow and there is a need for surgical correction of the affected arteries.
The causes of PAD are the same as the factors that provoke the development of atherosclerosis:
- *imbalance in lipoproteins and accumulation of cholesterol in vascular walls;
- autoimmune pathologies accompanied by infiltration of vessel walls with leukocytes and macrophages;
- congenital defects in the structure of blood vessels;
- hormonal imbalances of adrenocorticotropic and gonadotropic hormones, leading to increased cholesterol levels in the blood;
- failures in antioxidant systems;
- brought infections.
*Elevated is considered to be a total cholesterol level of more than 8 mmol/l, an HDL level in men of less than 1 mmol/l and in women less than 1.3 mmol/l, an LDL level of more than 6 mmol/l, and a triglyceride level of more than 1.7 mmol/l.
All these reasons can trigger the process of formation of atherosclerotic deposits, but the leading role in damage to peripheral arteries lies in lipid balance disorders. According to statistics, men over 40–45 years of age are more likely to encounter such pathologies.
The following controllable and uncontrollable factors can predispose to the development of atherosclerotic lesions of the arteries:
- age (for women after 55 years and men after 45 years);
- smoking;
- postmenopausal period;
- excess weight and waist circumference in women is more than 88 cm, and in men more than 100 cm;
- arterial hypertension more than 180/110 mm Hg. Art.;
- diabetes;
- hypothyroidism;
- hereditary disorders (coagulopathies, homocystinuria);
- hereditary predisposition to vascular and heart diseases;
- congenital vascular anomalies;
- adynamia;
- taking a large amount of fast food, fatty, fried, flour, sweets, baked goods, carbonated drinks;
- taking medications that increase blood cholesterol levels;
- taking hormonal contraceptives;
- disorders in the blood coagulation system, accompanied by increased thrombus formation;
- frequent stress;
- chronic sleep deficiency.
Uncontrollable factors cannot be eliminated. They contribute to the formation of atherosclerotic plaques, but in the absence of controlled conditions are not capable of causing obliterating atherosclerosis.
With the development of atherosclerosis, the following occurs:
- on the inner wall of the artery, a lipid stain is formed that transforms into liposclerosis, leading to the formation of unstable atherosclerotic plaques, which can still dissolve;
- fibrous plaques appear that can no longer resolve, and atheromatosis develops, accompanied by the disintegration of the contents of plaques, collagen and elastin in the vessels;
- when plaques disintegrate, the stage of complications of atherosclerosis begins: thrombosis, embolism, rupture of the aneurysm formed in the lumen of the artery;
- the formation of atherocalcinosis - this stage is accompanied by the deposition of calcium salts in the atherosclerotic plaque and severe ischemia of tissues and organs.
Symptoms of peripheral artery disease do not appear immediately, but only at the stage of severe ischemia of a particular area. Initially, the patient complains of pain, cramps and fatigue in the legs after walking or physical activity. The pain is usually located in the thighs, buttocks and feet. Sometimes patients may experience swelling. There is also no pulsation in the area of damage to the arterial vessel. The skin on the affected limb becomes paler and cooler to the touch at the level of the arterial lesions. Men may experience problems with potency due to impaired blood flow.
Somewhat later, the patient develops a symptom characteristic of obliterating atherosclerosis of the lower extremities, such as intermittent claudication (claudication) - pain and cramps in the calf muscles, aggravated by walking. It is provoked by a lack of oxygen, which is most pronounced during walking, and disappears after the person stops.
Intermittent claudication is most pronounced when climbing stairs. Initially, it occurs after walking long distances, and then, as atherosclerotic lesions of the arteries and ischemia progress, it appears even after covering very short distances. In the most advanced stages, it occurs even during rest. This condition is commonly called critical ischemia.
The stages of PAD are:
- I – symptoms of thrombosis and narrowing of the arteries are not felt;
- IIa – pain and intermittent claudication occur after covering more than 200 m;
- IIb – pain and lameness occur when covering less than 200 m;
- III – pain and intermittent claudication occur at rest;
- IV – due to ischemia, ulcers and wounds occur due to tissue necrosis.
The progression of PAD is indicated by the following manifestations:
- increased pain syndrome;
- sensory disturbances and coldness of the limb;
- dry skin and the appearance of cracks prone to infection;
- the occurrence of ulcers and wounds on the feet, legs or toes.
When PAD is complicated, it leads to the development of gangrene and the need for urgent surgery to amputate the limb.
Peripheral circulatory disorders
6
Disorders
of peripheral circulation
Blood circulation is distinguished :
1. central (systemic, in the great vessels),
2. peripheral (in small vessels and microvasculature).
Types of
peripheral circulatory disorders :
1. arterial and venous hyperemia
2. ischemia
3. stasis
4. thrombosis
5. embolism
6. hemorrhage.
Based on
anatomical and functional capabilities there are 3 types circulatory collaterals :
- functionally - absolutely
insufficient
collaterals - the sum of the lumen of the anastomoses is much less than the diameter of the afferent artery, when blockage occurs, an ischemic (white) infarction occurs (occurs in the heart, spleen, kidneys, terminal arteries are often found here); - functionally - absolutely
sufficient
- the amount of the lumen of the anastomoses is equal to (or exceeds) the diameter of the afferent artery; when a vessel is blocked, blood is delivered through another vessel; - intermediate type (typical of the lungs) - functionally
relatively insufficient
collateral - the sum of the lumens of the anastomoses is less than the diameter of the afferent artery, but blood also flows through fairly large branches, although they are thin and tortuous. When blockage occurs in this case, a hemorrhagic infarction often develops due to the abundance of blood and hypoxia.
Hyperemia
- excessive filling of tissue with blood.
Arterial hyperemia is increased blood flow to an organ through the arteries.
Microscopic changes:
- expansion of capillaries, increase in functioning vessels;
- increased blood pressure in arteries and arterioles;
- acceleration of blood flow through the vessels;
- The supply of oxygen to tissues increases, metabolism increases.
Macroscopic signs:
- an increase in organ volume due to blood supply, there may be a slight increase in heat production;
- metabolism increases, blood flow in the skin accelerates (increased skin temperature);
- redness (because there is a lot of oxidized hemoglobin);
- the arteriovenous difference in O2 decreases.
Classification of arterial
hyperemia :
1) physiological (physical activity, emotions, food intake):
a) working - this is an increase in blood flow in an organ with an increase in its function (for example, hyperemia of the pancreas during digestion);
b) reactive - this is an increase in blood flow after its short-term restriction (develops in the kidneys, brain, skin, intestines, muscles).
2) pathological (action of pathological stimuli).
According to
the mechanism of action of stimuli, pathological arterial hyperemia is divided into the following types :
- neurotonic (increased tone of parasympathetic fibers or sympathetic vasodilator => vasodilation, reverse impulse current => formation of prostaglandins => vasodilation);
- neuroparalytic (when nerves are blocked or cut => vasodilation; bradykinin and other substances have a vasodilating effect);
- myogenic (production of certain substances and their effect on smooth vascular myocytes => vasodilation). It is caused by difficulty in the flow of calcium into the cell due to the effect of lack of oxygen, hypercapnia, accumulation of lactate, ADP, adenosine, potassium, bradykinin, serotonin, histamine, GABA, prostaglandins, and increased blood pH. It happens with burns, injuries, exposure to ultraviolet and ionizing radiation, etc.
Causes of
arterial hyperemia :
- the effect of environmental factors (biological, chemical, physical);
- increased load on the organ;
- psychogenic effects.
Pathological
arterial hyperemia ( PAH ).
Occurs under the influence of a pathological irritant (chemicals, products of metabolic disorders due to inflammation, burns, fever, under the influence of mechanical factors.
There is increased sensitivity of blood vessels to irritants due to allergies.
Appears in diseases (rash, redness due to nerve damage, etc.).
Depending on the PAG factor, it happens:
1. inflammatory;
2. thermal
3. ultraviolet erythema, etc.
Prostaglandin I2 (prostacyclin) is released in the muscular wall of blood vessels, relaxing the arteries and having a powerful anti-aggregation effect on platelets.
The meaning of
pathological arterial hyperemia :
Good: 1. Removal of toxins,
2. Increased oxygen delivery to tissues,
3. This is the mechanism of action of diathermy, quartz, solux, galvanization, compresses, heating pads;
Bad: there may be rupture of sclerotic vessels with hemorrhages.
Venous
hyperemia ( VH )
is a violation of the outflow of blood from an organ through the veins. Causes: blockage (thrombus, embolus); pressure (tumor, edema, pregnant uterus, ligature).
Contributing factors: low elasticity of veins (constitution).
VH is distinguished by etiology :
1. obstructive
2. from compression
Microscopic
signs :
1. expansion of venules and veins, and later arterioles, drop in blood pressure, mainly increase in pressure;
2. the number of functioning vessels increases due to the opening of previously closed vessels;
3. blood flow speed decreases, linear and volumetric blood flow speed decreases;
4. jerky and pendulum-like movement of blood;
5. decreased metabolism, accumulation of under-oxidized metabolic products;
6. temperature drop due to a decrease in heat production and an increase in heat transfer;
7. arteriovenous difference in O2 increases sharply, hypoxia, increase
capillary permeability.
Macroscopic
signs :
1. enlargement of the organ due to dilation of blood vessels, an increase in their number, due to tissue swelling due to increased capillary permeability;
2. bluish color of the organ (a lot of reduced Hb, which has a dark cherry color);
3. ischemia (may be phlebosclerosis due to thickening of the venous wall, varicose veins) => stimulation of connective tissue growth => hardening of the organ, but sometimes this is useful for cavernous tuberculosis and trophic ulcers.
Venous
hyperemia develops with :
1. weakening of the function of the right ventricle;
2. reducing the suction effect of the chest (exudative pleurisy, hemothorax);
3. obstruction of the duct in the pulmonary circulation (pneumosclerosis, pulmonary emphysema);
4. weakening of left ventricular function.
VG value :
Good: increased rate of scar formation,
Bad: 1. Atrophy and dystrophy (due to inhibition of metabolism),
2. Sclerosis and fibrosis of the organ with dysfunction.
Ischemia
- a violation of peripheral circulation, which is based on the restriction or complete cessation of arterial blood flow to the organ.
Etiology
:
1. blockage (embolism, thrombosis, sclerosis) of the artery,
2. obturation,
3. vasospasm.
Accordingly ,
according to the etiology ischemia is :
1. compression
2. obstructive
3. angiospastic
Causes:
1. compression – compression of the artery by a ligature, scar, tumor, foreign body, etc.
2. obstructive – thrombosis, embolism (atherosclerosis, obliterating endarteritis, periarteritis nodosa)
3. angiospastic – emotions (fear, anger), physical and chemical factors (cold, trauma, mechanical irritation, chemicals, bacterial toxins).
The differences between a physiological spasm and a pathological one are the persistence and duration of the latter.
Microscopic
changes during ischemia :
1. narrowing of arterioles,
2. reduction in the number of functioning vessels (collapse of many vessels),
3. slowing down of blood flow with a more pronounced slowdown in volumetric velocity than linear,
4. lowering blood pressure,
5. tissue hypoxia,
6. arteriovenous difference in O2 increases slightly
7. decreased metabolic rate
8. accumulation of under-oxidized metabolic products => acidosis. Macroscopic
changes during ischemia :
1. pallor of tissues (low blood flow),
2. reduction in organ volume, decrease in tissue turgor,
3. decrease in organ temperature,
4. painful sensations (paresthesia - tingling, goose bumps; pain up to painful shock).
Stages
of ischemia :
- stage of decreased metabolic rate;
- stage of dystrophic changes: decreased synthesis of enzymes, NK, structural proteins => changes in organelles (swelling of mitochondria, disruption of the structure of crypts, then their reduction and destruction, death of the nucleus), cell death ^> necrosis (infarction);
- stage of sclerosis: synthesis of connective tissue => scarring (synthesis of collagen, acidic and neutral glycosaminoglycans) => sclerosis.
Angiospastic (neurospastic) ischemia: mechanism: spasm of the renal artery in one kidney leads to a reflex spasm in the other, spasm of other arteries (maybe the conditioned reflex nature of the spasm), reasons: fear, stress, predominance of the tone of the sympathetic nervous system, maybe direct irritation of the vasomotor center by toxins, tumors, cerebral hemorrhages, with increased intracranial pressure, inflammation in the diencephalon.
Outcome
with ischemia :
1. dystrophy
2. atrophy
3. necrosis
Factors that
determine the outcome of ischemia :
1. diameter of the damaged artery;
2. Duration of spasm, compression, thrombosis, embolism;
3. the rate of development of ischemia and the degree of obliteration of the artery (if the vessel is abruptly ligated, there will be a reflex spasm of other arteries);
4. tissue sensitivity to hypoxia (the most sensitive neurons, then the myocardium);
5. initial state of the organ (hyperfunction worsens the consequences of ischemia);
6. the nature of the development of collateral circulation.
Thrombosis
– intravital formation of blood clots on the inner surface of the vessel wall. Types of blood clots:
1. a) wall
b) clogging
2. a) red
b) white
c) mixed
Stages
of thrombus formation ( phases ):
1. cellular (when it predominates, the thrombus is white)
a) formation of active thrombokinase
b) prothrombin => thrombin
c) fibrinogen => fibrin
2. plasma (if it predominates, the blood clot is red) – fastening of fibrin threads with a stabilizing factor and getting stuck in the fibrin threads of blood cells
Mechanism:
- damage to the vascular wall (trauma, the action of chemicals: NaCl, FeCl3, HgCl2, AgNO3, microbial endothelins), trophic disturbances, atherosclerosis - damage without injury;
- violation of the coagulation and anticoagulant system - an increase in thromboplastin or a decrease in heparin, maybe. thrombocytosis;
- disturbance of blood flow - its slowdown, jerky, pendulum-like flow - with atrial fibrillation.
With a significant slowdown in blood flow, there are more conditions for erythrocytes to get stuck and coagulation and the blood clot will be red, but with fast flow there are no conditions for erythrocytes to get stuck, blood clotting factors are carried away, red blood cells are washed out and the blood clot will be white. That. Red blood clots often form in veins, and white ones in arteries. Red blood clot forms faster
Outcome
of thrombosis :
- aseptic melting (enzymatic, authentic) – typical for small blood clots;
- organization of a blood clot - germination by connective tissue;
- recanalization – germination of connective tissue with the formation of a canal;
- purulent septic melting of a blood clot by microbes;
- rupture and embolism (until the thrombus has sprouted with connective tissue);
- deposition of calcium salts in the veins – petrification with deformation (formation of phleboliths).
Strict bed rest for phlebothrombosis is necessary for about 3 weeks to organize a blood clot so that it does not break off and lead to ischemia and necrosis.
Factors that
determine the severity of the consequences ( consequences - ischemia , necrosis ):
1. diameter of the vessel (the larger the diameter, the worse);
2. type of vessel (artery – necrosis, vein – venous hyperemia, edema);
3. the nature of the thrombus (parietal - less dangerous, clogging - more dangerous);
4. rate of thrombus formation;
5. sensitivity of organs and tissues to hypoxia;
6. the possibility of a reflex disturbance of blood flow in nearby vessels;
7. degree of severity of collateral circulation.
Embolism
– blockage of blood vessels by bodies (emboli) brought by blood or lymph flow. Types of emboli:
1. endogenous (blood clots, pieces of tissue from injuries, tumor metastases, in case of fractures of tubular bones, yellow bone marrow enters the non-collapsing vessels of the bones with the development of fat embolism, amniotic fluid embolism)
2. exogenous
a) air – it enters large veins
- air embolism - when large veins are damaged (subclavian, jugular, chest veins - due to negative pressure, neck veins - because they are fused to the fascia and do not collapse)
- gas embolism – decompression sickness
b) bacterial embolism (squeezing a boil on the face => veins of the face communicate with the veins of the brain => brain abscess)
c) foreign bodies
d) parasites
Types
of embolism by location :
1. small circle
2. large circle
3. Gate system
Sources of large circle emboli are the lungs, the left half of the heart, and large arteries.
The sources of emboli in the small circle are the veins of the systemic circle and the right heart.
The sources of portal system emboli are the vessels of the unpaired abdominal organs.
Retrograde embolism occurs when a thrombus moves against the blood flow due to the weak suction effect of the chest.
Paradoxical embolism occurs with defects of the septum of the heart (a thrombus from the right heart goes to the left).
Pulmonary embolism :
Pathogenesis :
1. drop in blood pressure, multiple small embolism is more dangerous; a drop in systemic pressure due to the fact that there is a reflex decrease in arterial tone;
2 myocardial hypoxia;
3. increased pressure in the pulmonary artery due to spasm of the arteries of the pulmonary artery system (a protective reaction that prevents pulmonary edema);
4. acute cor pulmonale (overload of the right parts) => decreased contractility => fibrillation => death;
Clinic – severe shortness of breath, collapse, cyanosis, drop in blood pressure, swelling of the neck veins.
Portal vein embolism :
When the portal vein is blocked, up to 90% of the blood accumulates in the veins of the portal system, because Normally, portocaval anastomoses do not function, and portal hypertension does not occur. If there is thrombosis of a branch of the portal vein (splenic, superior and inferior mesenteric veins), then there will be portal hypertension. If there is a blockage of the portal vein itself, then death occurs within 15 minutes. - 2 hours due to cerebral ischemia. With gradual obstruction, portal hypertension develops (ascites, dilatation of the superficial veins of the anterior abdominal wall, enlargement of the spleen, drop in blood pressure, decrease in blood volume due to accumulation of blood in the gastrointestinal tract, shortness of breath, then decreased breathing, apnea, loss of consciousness, respiratory paralysis).
Factors that
determine the severity of the consequences of embolism ( consequences - ischemia , necrosis ):
1. diameter of the vessel (the larger the diameter, the worse);
2. type of vascular system;
3. duration of embolism;
4. the nature of the embolus (the bubble dissolves, microbes cause an abscess, the tumor causes metastases);
5. multiplicity of vascular damage;
6. sensitivity of organs and tissues to hypoxia;
7. the possibility of a reflex disturbance of blood flow in nearby vessels;
8. degree of severity of collateral circulation.
Stasis
– slowing down and stopping blood flow in capillaries, small arteries and veins.
Types
of stasis :
- ischemic – a consequence of cessation of blood flow, reversible;
- venous – a consequence of venous hyperemia (compression of veins, thrombosis, embolism), reversible;
- true (capillary) – a consequence of pathological changes (damage by toxins, chemicals, temperature, radiation, mustard, castor oil) in the capillaries or a drop in blood rheology, irreversible.
Mechanism:
In true stasis, red blood cells stick together => obstructed blood flow => increased peripheral resistance, increased capillary permeability, slowed blood flow due to blood thickening, release of Hb from red blood cells. BAS (serotonin, bradykinin, histamine) and acidosis are also important in the mechanism. The release of plasma albumin into tissue causes a decrease in the charge of erythrocytes. The adhesion of red blood cells is also explained by the fact that
that their surface becomes rough, their sorption properties decrease.
Microcirculation
– orderly movement of blood and lymph through microvessels, transcapillary metabolism, as well as the movement of fluids in the extravascular space.
The microvasculature includes: arterioles, precapillaries, capillaries, postcapillaries, venules, arteriovenular shunts, lymphatic capillaries.
Microcirculation disorders:
- intravascular: aggregates (sludge syndrome) - a violation of the suspension state of the blood (the more globulins and fibrinogen that have a “+” charge (in erythrocytes there is a “-“ charge), the stronger the sludge syndrome), a violation of blood viscosity.
- extravascular
- transmural
Aneurysms
Aneurysms of peripheral arteries are characterized by the appearance of pathologically dilated areas of the arterial wall, resulting from its weakening. As a result, the artery wall bulges and this condition can be complicated by thromboembolism, strokes, or, if the arterial wall is significantly thinned, ruptures.
About 70% of such aneurysms occur in the popliteal arteries, and 20% in the iliofemoral segment. Sometimes they are combined with abdominal aortic aneurysms, which in 50% of cases are bilateral. Typically, aneurysms of peripheral arteries are provoked by atherosclerosis and infectious diseases (in such cases, the protrusion is most often localized in the femoral artery). Sometimes the root cause of their occurrence is entrapment of the popliteal artery or septic emboli, leading to the formation of a mycotic aneurysm.
Peripheral aneurysms are often asymptomatic. In some cases they are manifested by the following symptoms:
- pain when palpating;
- pallor and coldness of the affected limb;
- sensitivity disorders;
- absence of pulse in the affected area due to thromboembolism or rupture of a pathological protrusion;
- pain, fever, general malaise (if the aneurysms are infectious).
The risk of artery rupture in the area of the aneurysm is low - no more than 5% for popliteal bulges and 1 - 14% for iliofemoral aneurysms.
Phlebeurysm
Varicose veins are a pathological expansion of the lumen of superficial venous vessels, accompanied by incompetence of the venous valves and leading to impaired blood flow. It is usually not possible to determine the underlying cause of vascular damage. Such a disorder is usually caused by primary valvular insufficiency and reflux, primary dilatation of the venous walls due to weakness of vascular tissues, chronic venous hypertension or insufficiency.
Varicose veins are more often detected in women. It often occurs during pregnancy or difficult childbirth. There are usually no risk factors for its development, but sometimes its occurrence is explained by hereditary predisposition. As a rule, it is the veins of the lower extremities that are affected.
Symptoms of varicose veins are not always visually noticeable. At the beginning, the veins may be tense and palpable. As the disease progresses, they enlarge, protrude above the surface of the skin and become visible. The patient complains of leg pain, discomfort, fatigue, tension and pressure. Particularly pathological dilated vessels are noticeable in a standing position.
When a vein thromboses, the patient experiences severe pain, and the superficial veins can form venous bullae, which rupture and bleed at the slightest physical impact. Sometimes such bleeding goes unnoticed (for example, during sleep), and leads to death.
Ulcers and other dermatological disorders with varicose veins rarely occur. They can manifest as eczema or pigmentation that appears in the ankle area. Ulcerative lesions usually occur after injury and are small in size and superficial.
Circulatory disorders
General information
The health of the body depends on the condition of the circulatory system. Violation of the blood supply to an organ of the body leads to the fact that the tissues cannot receive the required amount of nutrients and oxygen. As a result, a person’s metabolism slows down and hypoxia develops. In addition, metabolism slows down. Hypoxia develops - low oxygen content in the body or individual organs and tissues. This can lead to the development of serious diseases. As a result, the health of the body as a whole depends on the state of the circulatory system.
Circulatory disorders
Ensuring blood flow is a complex process that depends on the functioning of the heart and the integrity of blood vessels. Depending on the location, blood circulation can be:
- general;
- local.
General disorders can occur in the body as a result of disruption of the heart, changes in the physicochemical properties of the blood. Disorders of blood and lymph circulation are caused by structural and functional damage to the vascular bed in any of its sections - in one organ, part of an organ or part of the body.
What diseases cause circulatory disorders
It is necessary to understand that the division of circulatory disorders into general and local is quite arbitrary, since in terms of reducing blood pressure in the aorta it leads to a decrease in blood supply to the renal cortex. Which, in turn, activates the renin-angiotensin system and causes an increase in blood pressure.
Local circulatory disorders are a consequence of general disorders. With general venous congestion, thrombosis of the veins of the lower extremities often develops.
Myocardial infarction is the first cause of heart failure, and bleeding as a local process can be the cause of general acute anemia.
General circulatory disorders:
- general arterial plethora;
- venous congestion;
- anemia (acute or chronic);
- blood thickening;
- blood thinning;
- shock;
- DIC syndrome.
Arterial hyperemia is an increase in the number of blood cells (erythrocytes), sometimes combined with an increase in the volume of circulating blood. The process is relatively rare: when climbing to a height, in residents of mountainous areas, in people with lung pathologies, as well as in newborns. Symptoms may be as follows:
- redness of the skin;
- increased blood pressure.
Arterial congestion is of greatest importance in Vaquez disease (polycythemia vera), a disease in which there is a true overproduction of red blood cells.
General venous congestion
One of the most common types of general circulatory disorders is general venous congestion. It is a clinical and morphological manifestation of pulmonary heart failure.
Three main factors play a role in the pathogenesis of general venous congestion
- disturbance of heart activity;
- pulmonary diseases;
- chest injuries.
Cardiac dysfunction or heart failure may be associated with acquired and congenital heart defects. Other reasons could be:
- inflammatory heart diseases (myocarditis, endocarditis);
- cardiosclerosis of various etiologies (atherosclerotic, post-infarction);
- myocardial infarction.
Pulmonary diseases are accompanied by a decrease in the volume of vessels in the pulmonary circulation:
- pneumosclerosis of various etiologies;
- emphysema;
- chronic nonspecific pneumonia;
- pneumoconiosis.
In case of damage to the chest , as well as the pleura and diaphragm, the suction function of the chest is impaired:
- pleurisy;
- pneumothorax;
- chest deformities.
Acute venous congestion is a manifestation of the syndrome of acute heart failure and hypoxia . There may be several reasons, namely:
- myocardial infarction;
- acute myocarditis;
- pulmonary embolism;
- pneumothorax;
- all types of asphyxia.
As a result of hypoxia , the histohematic barrier can be damaged and capillary permeability increases. In addition, the following is observed in the tissues:
- venous stagnation;
- plasmorrhagia;
- edema;
- stasis in capillaries.
Dystrophic and necrotic changes appear in parenchymal organs. The cause of venous congestion of the lungs is left ventricular heart failure. Acute venous congestion causes dilation of the alveolar capillaries, which is accompanied by pulmonary edema. may also occur .
General anemia
Depending on the etiology and pathogenesis there are:
- acute anemia;
- chronic anemia.
General acute anemia develops with large blood loss, due to a decrease in circulating blood volume (CBV) in the general circulation in a short period of time.
Causes of acute anemia:
- injuries with damage to organs, tissues, blood vessels;
- spontaneous rupture of a large, pathologically altered vessel or heart;
- rupture of a pathologically altered organ (ectopic pregnancy, pulmonary tuberculosis, gastric ulcer).
Symptoms of the disease are expressed:
- pale skin;
- dizziness;
- frequent weak pulse;
- low blood pressure.
Patients die as a result of hypovolemic shock.
Chronic anemia (anemia) is a decrease in the number of red blood cells and/or hemoglobin content in a volumetric unit of blood. The total volume of circulating blood in the body does not change. Causes of general chronic anemia:
- diseases of the hematopoietic organs (anemia);
- infections (tuberculosis, syphilis);
- parasites (helminthic infestations);
- exogenous intoxication (poisoning with lead, benzene, carbon monoxide);
- endogenous intoxication (poisoning with nitrogen metabolism products).
- starvation;
- avitaminosis.
Clinical manifestations of the disease:
- pallor,
- weakness;
- decreased performance,
- dizziness,
- fainting states.
A blood test for anemia shows a decrease in the number of red blood cells and a decrease in hemoglobin content.
Thickening and thinning of blood
Blood thickening is characterized by a decrease in the content of water and some electrolytes in the peripheral blood. As a result, blood viscosity increases, rheological properties change, and the number of cells per unit volume increases relatively. Blood thickening develops when a large amount of fluid is lost. The reasons can be completely different:
- severe forms of dysentery;
- salmonellosis;
- poisoning with toxic substances;
- iatrogenic pathology.
Blood thinning (hydremia) is an increase in the amount of water in a person’s peripheral blood. It is observed quite rarely in patients with:
- kidney diseases;
- hypervolemia;
- when replacing BCC with plasma and blood substitutes after blood loss;
- in some cases of resuscitation and intensive care, if doctors administer large amounts of fluid intravenously for the purpose of detoxification.
Disseminated intravascular coagulation syndrome
DIC syndrome is characterized by widespread formation of small blood clots in the microvasculature of the entire body. Together with blood incoagulability, it leads to multiple massive hemorrhages. The disease requires early diagnosis and urgent treatment. It is based on discoordination of the functions of the coagulation and anticoagulation systems of the blood responsible for hemostasis.
Possible causes of DIC syndrome :
- infections (fungal infection; meningococcal sepsis, rickettsiosis);
- severe viremia (hemorrhagic fever);
- neonatal or intrauterine infections;
- gynecological diseases (placental abruption, amniotic fluid embolism);
- liver disease (cirrhosis);
- malignant tumors;
- injuries;
- fever;
- surgical interventions with artificial circulation;
- intravascular hemolysis;
- severe shock;
- snake bites.
Numerous blood clots in the microvasculature in disseminated intravascular coagulation syndrome lead to impaired tissue perfusion with the accumulation of lactic acid in them and the development of ischemia, as well as the formation of microinfarctions in the body organs.
Shock is a clinical condition that is associated with a decrease in effective cardiac output and impaired autoregulation of the microcirculatory system. Characterized by a decrease in blood supply to tissues, which leads to destructive changes in internal organs. The following types of shock are distinguished:
- hypovolemic;
- neurogenic;
- septic;
- cardiogenic;
- anaphylactic.
Local circulatory disorders
Local circulatory disorders may be as follows:
- arterial plethora;
- venous congestion;
- thrombosis;
- embolism;
- ischemia;
- heart attack;
- bleeding;
- blood stasis.
Local arterial plethora (arterial hyperemia) is an increase in the flow of arterial blood to an organ or tissue. Experts distinguish hypermia:
- physiological;
- pathological.
A striking example of physiological arterial hyperemia can be a blush of shame on the face, pink-red areas of the skin at the site of its thermal or mechanical irritation.
Angioneurotic hyperemia is observed in vasomotor disorders and is characterized by an acceleration of blood flow not only in normally functioning, but also in opening reserve capillaries. The skin and mucous membranes become red, slightly swollen, and feel warm or hot to the touch. Usually this hyperemia passes quickly, leaving no marks on the body. Collateral hyperemia occurs when the main artery is closed by an atherosclerotic plaque. The inflowing blood rushes through the collaterals, which expand. The rate of closure of the great vessel and the level of blood pressure are of great importance in the development of collateral arterial hyperemia.
Postanemic hyperemia develops in cases of fluid accumulation in the cavities, causing ischemia. The vessels of previously bloodless tissue expand sharply and fill with blood. The danger of arterial hyperemia is that overcrowded vessels can rupture and lead to bleeding and hemorrhage. Brain anemia may occur.
Vacate hyperemia develops due to a decrease in barometric pressure. An example of such plethora is skin hyperemia under the influence of medical cups. Inflammatory hyperemia is one of the important clinical signs of any inflammation.
Local venous congestion
Venous hyperemia develops when the outflow of venous blood from an organ or part of the body is disrupted. Experts distinguish between hypermia:
- obstructive venous;
- compression venous hyperemia;
- collateral venous hyperemia.
Blood stasis is a slowdown, up to a complete stop, of blood flow in the vessels of the microvasculature in the capillaries. Blood stasis may be preceded by:
- venous congestion (stasis);
- ischemia.
Blood stasis is characterized by stopping blood in capillaries and venules with expansion of the lumen and gluing of red blood cells into homogeneous columns (this distinguishes stasis from venous hyperemia). Hemolysis and blood clotting do not occur.
Stasis is observed in the following diseases:
- angioedema crises (hypertension, atherosclerosis);
- acute forms of inflammation;
- viral diseases (flu, measles).
The cerebral cortex is sensitive to circulatory disorders and hypoxia Stasis can lead to microinfarction . Extensive stasis in areas of inflammation carry with them the danger of tissue necrosis, which can radically change the course of the inflammatory process.
Bleeding
Bleeding is the release of blood from the lumen of a vessel or the cavity of the heart. If blood is shed into the environment, then we talk about external bleeding, if in the cavity of the body - about internal bleeding. Examples of external bleeding may include:
- hemoptysis;
- nosebleeds;
- vomiting blood;
- discharge of blood in feces.
With internal bleeding, blood can accumulate in the pericardial cavity, pleura, and abdominal cavity. Hemorrhage is a special type of bleeding. The causes of bleeding (hemorrhage) can be rupture, corrosion and increased permeability of the vessel wall. Hemorrhages are distinguished:
- point;
- bruise;
- hematoma;
- hemorrhagic infiltration.
Thrombosis is intravital blood clotting in the lumen of a vessel, in the cavities of the heart, or loss of dense masses from the blood. The resulting blood clot is called a thrombus. In addition to the coagulation system, there is a system that ensures the regulation of hemostasis: the liquid state of blood in the vascular bed under normal conditions. Based on this, thrombosis is a manifestation of dysregulation of the hemostatic system.
Factors influencing thrombus formation :
- damage to the vascular endothelium;
- changes in blood flow;
- changes in the physical and chemical properties of blood.
The causes of thrombosis can be:
- infections;
- malignant tumors;
- postoperative period;
- diseases of the cardiovascular system.
The location of the thrombosis determines subsequent treatment; thrombosis exists:
- arterial;
- cordial;
- venous (thrombophlebitis, phlebothrombosis).
Thrombosis does not always have certain manifestations. Symptoms occur if the clot grows in size and rises above the calf (this can cause swelling and pain in the leg).
Diagnosis of vascular diseases of the lower extremities
To identify obliterating diseases of the arteries of the lower extremities (LOAD) and aneurysms, the patient is referred to a vascular surgeon. After a physical examination, the patient may be prescribed the following tests:
- determination of the ankle-brachial index;
- Doppler and duplex ultrasound scanning;
- digital angiography;
- CT angiography and MRI angiography;
- blood tests for the level of lipoproteins VP, NP and SNP, SC myoglobin and C-reactive protein, the level of total cholesterol and triglycerides, sugar, atherogenicity coefficient.
To find out the root cause of the disease and prevent complications, the patient may be recommended to consult other highly specialized specialists: cardiologist, neurologist, endocrinologist, hematologist, ophthalmologist. If necessary, the examination of the patient is supplemented by ECG, Echo-CG, Dopplerography of the vessels of the head and neck, renal arteries, etc.
Varicose veins are usually detected during an objective examination and special tests. If necessary, the examination is supplemented with duplex ultrasound scanning of the leg veins.
Treatment of obliterating atherosclerosis and superficial aneurysms of peripheral vessels
Treatment of OZANK is carried out depending on the nature and severity of the manifestations of the disease. If there is a slight disturbance in the structure of blood vessels, the patient is prescribed conservative therapy and dynamic observation.
All patients are recommended to eliminate the factors that provoke the progression of the pathology:
- to give up smoking;
- weight normalization;
- treatment of arterial hypertension and control of blood pressure;
- sufficient physical activity: walking, walks, physical therapy;
- changing your diet to reduce bad cholesterol and triglycerides;
- blood sugar control;
- the use of pneumatic cuffs and stockings to eliminate stress on blood vessels.
Drug treatment is aimed at reducing thrombus formation, normalizing blood flow and treating pathologies that increase the risk of stroke and myocardial infarction. For this purpose, the patient is prescribed antiplatelet agents (Aspirin, Cardiomagnyl, etc.), Pentoxifylline, ACE inhibitors, blood thinners (for example, Clopidogrel, Cilostazol, etc.).
If it is impossible to restore normal blood flow, patients with stage II-III OZANK can undergo the following types of surgical operations:
- thromboendarterectomy - performed to eliminate short localized lesions of the aorta, common or deep femoral, iliac arteries;
- artery bypass - an additional vessel (shunt) is created to bypass the blocked artery to normalize blood supply;
- artery replacement – the affected area of the artery is replaced with an artificial vascular prosthesis;
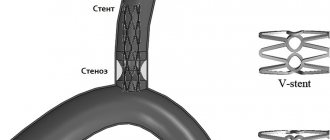
- endovascular operations (balloon angioplasty and artery stenting) - the lumen of the artery is expanded using a special balloon, which is inserted into the lumen of the artery and inflated; if necessary, a cylindrical wire structure (stent) can be installed at the site of narrowing, restoring normal blood flow.
The choice of surgical treatment method is determined by the clinical manifestations of the pathology. Endovascular interventions are less invasive and therefore doctors try to give preference to their implementation.
If surgical techniques turn out to be ineffective and the patient still develops gangrene, then to save his life, operations to amputate the limb (full or partial) are performed.
Also, for the treatment of patients with chronic ischemia of the lower extremities, angiogenesis stimulators (from autologous CD133+ endothelial progenitor cells) and Angiostimulin (a gene preparation of the vascular endothelial growth factor VEGF165) can be used.
Surgical removal of peripheral aneurysms of the vessels of the legs is indicated when the artery is dilated more than 2 times, and for protrusions in the arteries of the arms, operations are performed in all cases. To eliminate them, the affected area of the arterial vessel is excised and replaced with a graft. Sometimes an endovascular stent graft is used to repair aneurysms - a woven polyester tube covered with a metal frame is installed into the aneurysm without open surgery. This technique is used for patients who cannot undergo other types of surgery. Its purpose is to strengthen the vessel wall and prevent its rupture.
Lecture 5 viol.peripheral blood flow complete
4
Prepared by teacher N.E. Malle
Lecture 5
Peripheral circulation disorders
The following main forms of peripheral circulatory disorders are distinguished: arterial and venous hyperemia (plethora), ischemia, stasis, thrombosis, embolism, bleeding and hemorrhage. These disorders are a manifestation of the reaction of the entire organism and cause not only local disorders, but also severe general disorders in the body.
Arterial hyperemia
- increase in blood supply to the organ due to excess blood flow through the arterial vessels. The cause of arterial hyperemia is mental, chemical, biological, mechanical factors; increased load on the organ. Signs: redness, dilation of small arteries, veins and capillaries; an increase in the number of visible vessels and their pulsation; an increase in the volume of the affected area, an increase in local body temperature; increased pressure in arterioles, capillaries, veins; acceleration of blood flow, arterialization of venous blood; increased lymph formation; increased metabolism; strengthening organ function. Arterial hyperemia can be physiological - working (hyperemia of skeletal muscles during contraction, intestines during digestion) and pathological, occurring under the influence of pathogenic irritants (infectious rash, redness of the face during neuralgia, etc.).
The positive significance of arterial hyperemia is to enhance the delivery of nutrients and oxygen and remove metabolic products. The harmful consequences of arterial hyperemia are ruptures of blood vessels, the occurrence of hemorrhages, especially dangerous in the central nervous system.
Venous hyperemia
or stagnant - an increase in blood supply to an organ or tissue due to obstructed blood outflow through the veins.
Signs: dark red color (cyanosis); an increase in the volume of a tissue or organ, a decrease in local temperature, an increase in pressure in the veins and capillaries, a slowdown in blood flow, pendulum-like movements, edema, hemorrhages (erythrocyte diapedesis), decreased function; oxygen starvation of tissues, disruption of tissue metabolism and, as a result, proliferation of connective tissue; dystrophic changes, up to cell necrosis. Venous stagnation can be local (in the veins of the extremities when they are blocked by blood clots) and general (a manifestation of heart failure).
Ischemia
- local anemia - a decrease or complete cessation of arterial blood flow to a tissue or organ. Signs: paleness or disappearance of previously visible small vessels; decrease in organ volume, decrease in local temperature, slowdown in blood flow, decrease in blood pressure below the obstruction, sensory disturbances (numbness, sensation of “crawling goosebumps”), dysfunction, pain.
Depending on the cause of ischemia, the following types are distinguished:
- Angiospastic
- occurs as a result of mental (pallor of the face from fear), chemical, physical factors leading to a reflex spasm of small arteries.
- Obstructive,
caused by complete closure (thrombus) or partial (obliterating endarteritis, atherosclerosis) narrowing of the lumen of the vessel.
- Compression
- occurs as a result of compression of the adductor artery (tumor, scar, etc.).
The consequences of ischemia are determined by the degree of oxygen starvation of tissues and depend on the rate of development of ischemia, its type, location, duration, anatomical and functional features of collateral circulation.
Stasis
- slowing down and stopping blood flow in the vessels of the microvasculature. There are 3
type of stasis:
- ischemic
— occurs during venous stagnation, when the blood flow into the capillaries stops;
- venous
- with venous stagnation, when the outflow of blood stops;
- true
- caused by pathological changes in the capillaries or disturbances in the properties of the blood.
The cause of true stasis is the effect on tissues and blood vessels of damaging factors - physical, chemical, mechanical. Intracapillary aggregation (sticking together) of red blood cells occurs, which impedes blood flow. If the cause is eliminated and there are no deep changes in the tissue, blood circulation can be restored, otherwise necrosis develops in the tissue.
Thrombosis
- the process of intravital blood coagulation in the lumen of a vessel or the cavities of the heart. The blood clot that forms is called a thrombus.
There are 3 main factors in the formation of a blood clot: changes in the vascular wall (inflammation, ulceration, trauma, atherosclerosis); blood flow disturbances (slowdown, stagnation) and changes in blood quality: an increase in the number of coagulation factors - thromboplastin, prothrombin or a decrease in the number of anti-coagulation factors - heparin, fibrinolysin; an increase in the number of formed elements in the blood and its thickening.
Such changes occur with atherosclerosis, inflammatory and infectious diseases, burn disease, malignant tumors, blood transfusion, etc. Old age, obesity, immobility, and injuries contribute to thrombus formation.
By appearance, blood clots are divided into white, red, mixed and hyaline.
White thrombus
consists of an accumulation of platelets, fibrin with a more or less significant admixture of leukocytes. Usually white are slow-forming blood clots that are localized in the arteries.
Red blood clot
also consists of platelets, fibrin and leukocytes, but with a greater admixture of erythrocytes, which give the thrombus a dark red color.
They occur when blood flows slowly (usually in the veins). Subsequently, the entire mass of the red blood clot, as hemoglobin is washed out from the destroyed red blood cells, gradually becomes white. Mixed blood clots
are more common than others. The composition is the same. The appearance of a mixed thrombus presents a motley picture of alternating red and white stripes. A mixed thrombus has a head (the structure of a white thrombus), with which it is attached to the wall of the vessel, a body (the actual mixed thrombus) and a tail (the structure of a red thrombus). The thrombus grows from the tail.
Hyaline thrombi
found in MCR vessels. They consist of destroyed red blood cells, platelets, plasma proteins, rarely contain fibrin, and the thrombotic masses resemble hyaline.
Favorable outcomes of thrombosis include aseptic autolysis
- melting of the blood clot under the action of proteolytic enzymes. In small vessels, blood circulation is restored. Large blood clots are replaced by connective tissue (organization). Calcification (petrification) of the thrombus is possible. Calcified blood clots in the veins are called phleboliths (vein stones).
Adverse outcomes include thromboembolism and septic autolysis. Purulent melting of a blood clot can lead to thrombobacterial embolism, which is observed in sepsis.
The significance is determined by the speed of its formation, prevalence, localization and outcome. An occluding thrombus in an artery can cause tissue necrosis. A blood clot in a vein can obstruct the flow of blood from the affected area of the body. Each blood clot poses a danger to the body, because at any moment (physical activity, increased blood pressure, etc.) its complete or partial rupture may occur, followed by thromboembolism and blockage of another vessel, therefore depriving some part of the body of nutrition.
Embolism
- the process of transport by blood and lymph flow and blockage of small-caliber vessels by masses that are not usually found normally in the bloodstream. Particles carried by blood and lymph flow are called emboli.
According to their physical properties, emboli can be solid (blood clots, microorganisms, parasites, foreign bodies, malignant tumor cells, tissue particles), liquid (fat, amniotic fluid) and gaseous (air, gas).
Thromboembolism is more common in the clinic. There are arterial and venous thromboembolism. With arterial thromboembolism, blood clots are localized on the valves of the left heart and in the aorta, with venous thromboembolism - in the veins, mainly of the lower extremities, pelvis, and, breaking off, enter through the right half of the heart into the pulmonary circulation.
Fat embolism
occurs when droplets of fat enter the vessels of the lungs, for example, due to injury to long tubular bones, or intravenous administration of oily medications.
Air embolism
occurs when veins located close to the heart are injured, where its suction effect is more pronounced. The second factor causing air embolism is the gaping of veins, in particular the veins of the neck. Therefore, air embolism is more often observed during operations in the neck area, sometimes during intravenous administration of drugs, etc. In all cases, air bubbles enter the cavities of the right heart, accumulate in them and stretch the heart. Sudden death occurs.
Gas embolism
occurs when a person quickly transitions from a zone of high to normal barometric pressure or from a zone of normal to low pressure.
The significance of emboli is that they complicate the course of many diseases; only gas embolism is considered a manifestation of an independent disease - decompression sickness.
Thromboembolic complications, especially pulmonary embolism, leading to sudden death, are of great clinical importance. Thromboembolism of the arteries of the systemic circulation is a common cause of the development of infarctions of the brain, kidneys, spleen, gangrene of the intestines and extremities. Bacterial embolism is no less important for the clinic as the mechanism of spread of purulent embolism by malignant tumor cells is the basis of the metastasis process. The significance of fat embolism is not so great, but in some cases it can cause death.
DIC syndrome.
Syndrome of disseminated intravascular coagulation is an acquired process of impaired hemostasis, morphologically characterized by the formation of multiple blood clots in the vessels of the central nervous system with simultaneous incoagulability of the blood, leading to massive hemorrhages. The cause of the development of DIC is the pronounced activation of the hemostasis polysystem by endogenous (tissue thromboplastin, tissue breakdown products and blood cells) and exogenous (microorganisms, viruses, drugs) factors. As a result of hemodynamic disorders, dystrophic and necrotic changes in various organs and tissues occur with disruption of their function. Histologically, blood thickening (sludge), erythrocyte agglutination, platelet aggregation, and hemorrhages are detected. The following organ changes are most often observed: “shock lung”, necrotic nephrosis, hemorrhages and erosions along the gastrointestinal tract, hemorrhages and necrosis in the adrenal glands, brain, myocardium, pancreas.
Hemorrhage (bleeding
) is the release of blood beyond the vascular bed into the environment (external bleeding), into the body cavity or the lumen of a hollow organ (internal bleeding).
According to the source, they are divided into arterial, venous, mixed, capillary, parenchymal and cardiac. Hemorrhage is
an extravascular accumulation of blood in tissues.
Varieties: hematoma
- hemorrhage with disruption of tissue integrity and the formation of a cavity;
bruise
– planar hemorrhage in the skin, subcutaneous tissue, mucous membranes.
petechiae
– pinpoint hemorrhages in the skin, membranes of internal organs.
Multiple confluent petechiae – hemorrhagic purpura, bruising up to 2 cm – ecchymosis
.
The tendency to bleed out of proportion to the degree of damage is called hemorrhagic diathesis.
Diapedesis
– blood leakage due to increased permeability of intact vessels during hypoxia, intoxication, infections, hemostasis disorders;
Treatment of varicose veins
To eliminate varicose veins, both conservative and surgical techniques are used. The patient is recommended to wear compression products (stockings, tights or knee socks) and periodically take medications to strengthen the walls of venous vessels (Troxevasin, Detralex, Cyclo 3 Fort, etc.). For local application, agents such as Lyoton, Curiosin, Venoruton, Heparin ointment, etc. are used. To normalize the condition of veins and blood flow, physiotherapy can be prescribed: amplipulse therapy, local darsonvalization, intermittent pneumocompression, magnetic therapy, hyperbaric oxygenation, laser therapy, balneo- and hydrotherapy.
As a minimally invasive technique for minor manifestations of varicose veins, sclerotherapy can be performed - the introduction of a sclerosant drug (for example, Fibro-Vein, Athoxysclerol, Sodium tetradecyl sulfate, Sclerowein, etc.) into the dilated areas of the veins, causing “gluing” of the pathologically dilated vessel. Other minimally invasive techniques can be used to remove varicose veins - ablation using laser or radiofrequency ablation. These procedures seem to seal the dilated vessels. In other cases, traditional surgical interventions are performed to remove veins, consisting of ligation or removal of the large and sometimes small saphenous veins. They are performed using different methods (stripping, miniphlebectomy, crossectomy) and can be supplemented with minimally invasive methods. The patient may also be prescribed some endoscopic types of interventions: endoscopic dissection and transluminal phlebectomy.