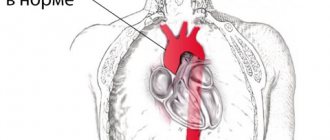
It branches like a tree, first into large branches (trunks), then into smaller branches and twigs, and is conventionally divided into several parts or sections:
- 1. The ascending aorta is the area from the aortic valve to the brachiocephalic trunk.
- 2. The aortic arch is a short section from which all the vessels supplying the arms and head (brachiocephalic arteries) depart. They anatomically form an arch connecting the ascending and descending aorta.
- 3. The descending (thoracic) aorta begins from the mouth of the left subclavian artery and continues to the diaphragm.
- 4. Below the diaphragm and before the bifurcation of the aorta (bifurcation) is the abdominal aorta.
Dividing the aorta into sections is very important for assessing risk and choosing optimal treatment tactics in patients with aortic aneurysms.
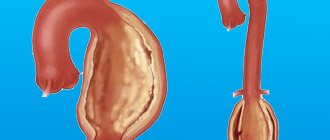
An aortic aneurysm is an area of local expansion.
Causes of aortic enlargement
Congenital systemic connective tissue diseases: Marfan syndrome, Ehlers-Danlos syndrome, caused by genetic changes in which the aortic wall has an abnormal structure, can cause the development of an aneurysm.
Acquired diseases that cause aneurysmal changes in the aortic wall: most often this is atherosclerosis. About 80% of all complicated aortic aneurysms are aneurysms caused by an atherosclerotic process, which leads to weakening of the vessel wall and the inability to withstand normal blood pressure, and as a result, to its expansion.
Less commonly, an aortic aneurysm develops in inflammatory diseases caused by external agents (syphilis, fungal infection, tuberculosis) or in autoimmune diseases (nonspecific aortoarteritis).
Ultrasound of the aorta in the abdominal cavity
Ultrasound of the abdominal aorta: indications, performance, interpretation of results
Ultrasound is used to diagnose the abdominal aorta. The technique makes it possible to find out about the presence of blood flow disturbances, damage or changes in the walls of the vessel. This procedure is performed with Doppler ultrasound.
Ultrasound of the abdominal aorta: what is it?
During the procedure, the ultrasound doctor will examine the area from the last thoracic vertebra to the sacrum. Standard ultrasound does not make it possible to assess the condition of the vessels in full, so Doppler sonography is used to diagnose the aorta. It is based on the possibility of reflecting ultrasound waves from objects in motion.
During Dopplerography, the branches of the aorta and the aorta itself are painted in different colors, which helps the ultrasound specialist make a conclusion about the state of the blood flow.
In what cases is aorta diagnosed?
The main task of this procedure is to detect the aneurysm. It is characterized by thinning of the vessel wall and the appearance of a sac. This leads to improper blood flow in the vessel. The disease is dangerous due to rupture of the vessel wall and heavy bleeding.
Diagnosis of the abdominal aorta is carried out in the following cases:
- The appearance of throbbing pain in the head;
- The patient has arterial hypertension;
- Severe pain in the abdomen on the left side, spreading to the lower back;
- The patient has memory problems;
- Changing the shape of the abdomen;
- Unreasonable nausea and repeated vomiting;
- The presence of blood in the stool;
- Presence of pulsation in the middle part of the abdomen;
- Decrease or increase in pressure;
- Previously suffered a heart attack or stroke;
- Suspicion of an aneurysm in a smoking patient.
How to properly prepare for the procedure?
If you have been prescribed an ultrasound examination of the abdominal aorta, then you should properly prepare for it. Before such an ultrasound, it is imperative to cleanse the intestines and prevent flatulence. In the absence of preparation, the study may be uninformative, since the object being examined is located behind the intestines, and if it is full, it will be almost impossible to see the artery.
You should start preparing for an ultrasound 3 days before the intended examination. During this time, you should adhere to certain dietary rules and also take certain medications. From the diet you need to completely exclude foods that can cause gas: fermented milk products, legumes/peas, bread (black), cabbage.
If necessary, 2 days before the test, the doctor will recommend medications that improve digestion.
1 day before the ultrasound in the evening, you should cleanse the intestines naturally or with an enema.
The last time you can eat is 8 hours before the ultrasound. You can drink for the last time 2 hours before the test.
Preparation is not carried out only if the patient is admitted to the hospital with complaints of acute pain in the abdominal area. In this case, emergency care may be required, and the preparation time may adversely affect the patient's health.
How is ultrasound of the aorta performed?
Do not be afraid, the examination is completely painless and safe, it is carried out in the same way as a simple ultrasound. During the ultrasound, the patient lies on his back. An ultrasound technician moves an ultrasound probe across the abdomen to diagnose the abdominal aorta. The duration of the procedure is about half an hour.
The patient can watch the procedure on a large screen located opposite the couch. If necessary, the ultrasound doctor asks the necessary questions and comments on what is happening on the screen. Immediately after the study, a conclusion is issued. To prescribe treatment or adjust it, you must contact the attending doctor who referred you for an ultrasound scan.
Diseases that can be detected during ultrasound examination of the abdominal aorta: aortic dissection (which is characterized by a rupture of the walls); aneurysm (depletion of the wall of the abdominal artery will be clearly noticeable); occlusion (impaired vascular patency; a break in blood flow can be seen on the image); atherosclerosis (the appearance of cholesterol plaques, an ultrasound specialist diagnoses them by thickening the artery wall); stenosis (the main branch of the aorta narrows); calcification (formation of calcium salts).
How to decipher the research?
Thanks to Doppler ultrasound, it is possible to obtain information about the exact sizes of blood vessels, identify certain pathologies, determine the possibility of a risk of their occurrence, understand the speed of blood flow and study in detail places with obstructed blood flow.
The abdominal aorta should not be more than 3 centimeters in thickness. With a smaller diameter, there is a high probability of atherosclerosis or stenosis. If the diameter is more than 3 centimeters, an aneurysm is suspected. The ultrasound doctor examines the aorta; the diagnosis is made only by the doctor who prescribed the diagnosis.
If the size of the abdominal aorta exceeds 5 centimeters, surgery will be prescribed to remove the cause of the pathology. Otherwise, it may be dangerous to the patient's life.
The procedure is prescribed for patients predisposed to cardiovascular diseases, as well as for the elderly. By identifying pathology at an early stage of its development and prescribing appropriate treatment, the chances of a speedy recovery increase.
Advanced blood flow pathologies are quite difficult to treat and in most cases require surgery.
Ultrasound of the abdominal aorta in Nizhny Novgorod.
In Nizhny Novgorod, diagnostics of the aorta using ultrasound is carried out at the VIP Academy clinic. The examination is performed on the latest ultrasound machine by a certified specialist.
Cost of ultrasound examination Ultrasound of the abdominal aorta.
The price for an ultrasound of the aorta in a medical clinic is the average city price. The availability of this diagnostic method makes it possible to timely identify and prevent life-threatening diseases. Pathologies of the abdominal aorta are characterized by blood loss, as well as damage to vital organs of the body. It was thanks to timely, high-quality ultrasound diagnostics and the work of surgeons that in many cases patients were able to save their lives.
If a doctor prescribes this procedure, it should not be ignored under any circumstances.
You can sign up for an ultrasound of the abdominal aorta at the VIP Academy clinic through the administrators at: +7 (831) 200-47-38.
Symptoms of aortic aneurysm
Unfortunately, the diagnosis of aortic aneurysm cannot always be established during the “cold period” (before complications develop), since this disease is usually asymptomatic. Most often, it is discovered accidentally during fluorography, ultrasound or tomography studies performed in connection with other diseases. Treatment of an aneurysm of the ascending aorta before complications develop is much safer for the patient, therefore, in the early diagnosis of an aortic aneurysm, routine medical examination is important.
It is worth noting that every hundredth patient who died suddenly dies from aortic dissection.
Complaints usually appear when the aneurysm begins to stratify or, enlarging, compresses surrounding organs and tissues. Pain or dysfunction of those organs located in the area of the aneurysm appears. At first, this is not of a bright nature and, therefore, does not alarm either the patient or the doctor.
However, the pain intensifies as these deadly complications of an aortic aneurysm develop—it is some of the most severe pain a person can experience. It is localized in the chest if the aneurysm is located in the ascending, descending sections or in its arch, or in the abdomen if it formed in the abdominal section. Characterized by severe weakness, pallor, and often the person loses consciousness.
Impaired blood supply to organs located in the area of aneurysm rupture or aortic dissection (brain or spinal cord, kidneys, intestines, upper or lower extremities) leads to loss of function of these organs, and a large volume of blood loss during aortic rupture represents the most serious danger. To save a life, minutes count. If early surgical treatment is not available, the first-day mortality rate for aortic dissection is 1% per hour (one person in a hundred dies every hour). Within the first 24 hours, 33% of patients die from aortic dissection, 50% of patients within 48 hours and 75% within two weeks. Only early surgical intervention makes it possible to save a significant proportion of patients.
How is MSCT of the aorta performed?
The duration of the study itself is approximately 15-20 minutes. The examination is usually performed in the supine position. You cannot move during the examination. You need to breathe calmly and evenly. You may be asked to hold your breath for a short time. Holding your breath is very important for obtaining high-quality images. The contrast agent is administered intravenously in a volume of up to 50-150 ml using a special injector device synchronized with the operation of the computed tomograph.
Sometimes, when a contrast agent is administered, nausea, a feeling of heat, anxiety, and skin reactions at the injection site may occur. These reactions usually disappear without a trace after the study and do not require any treatment.
Diagnosis of aortic aneurysm
In the diagnosis of aortic aneurysms, the so-called imaging techniques (ultrasound, MRI, CT, AG) are of greatest importance. In the ascending aorta, its arch and in the abdominal section, an aneurysm can be detected using ultrasound methods (ultrasound). To diagnose an aneurysm of the descending (thoracic) aorta, X-ray methods (x-ray, computed tomography) are required. To establish a final diagnosis and select a treatment method, contrast research methods are performed. Currently, the optimal diagnostic method, which provides the most complete information about the location, extent, diameter of the aneurysm and its relationship to nearby organs, is multislice computed tomography - aortography.
Material and methods
The study was conducted on 123 hearts taken at autopsy in city pathological and forensic departments from the corpses of patients of both sexes aged from 28 to 87 years (35 men and 57 women) who died from causes not related to diseases and injuries of the heart. The hearts were removed as a single complex along with the lungs, mediastinum, diaphragm and organs of the upper abdominal cavity. The heart chambers were washed with warm water to remove blood clots and blood clots. Through a cannula inserted into the thoracic aorta, after ligation of the large vessels of the aortic arch and coronary arteries, a solution of warm water was injected under a constant hydrostatic pressure of 0.18 bar, equivalent to 140 mmHg. to determine AA deficiency. In cases where the pressure in the aorta dropped rapidly, such hearts were assigned to the group with aortic valve insufficiency (group 2), which consisted of 15 hearts. The remaining hearts were assigned to the control group with preserved valve closure function (group 1), amounting to 108 hearts. Fixation of the preparations was carried out by continuous perfusion of an 8% formalin solution injected through a cannula into the aorta under a pressure of 0.18 bar (140 mm Hg) and into the superior vena cava under a pressure of 0.02 bar (15 mm Hg). within 5 days.
For the study, morphometric methods were used on freshly fixed preparations, on preparations made by silicone plastination at room temperature, as well as on preparations of hearts in which the chambers and large vessels were filled with a polymerized colored silicone composition with the addition of radiopaque red lead. In addition to morphometry, injected and plastinated hearts were examined using computed tomography and magnetic resonance imaging.
To prepare an injectable colored radiopaque silicone composition, a mixture of 92 parts by mass of SKTN E grade silicone, 5 parts by mass of red lead and 3 parts by mass of hardener K-1 was used. All components were thoroughly mixed until a homogeneous mass was obtained immediately before injection. A radiopaque composition was injected through a cannula installed into the ascending aorta at a pressure of 100 mmHg. Art., which contributed to the closure of A.K. The left ventricle and left atrium were filled through a cannula inserted into the left atrial appendage at a pressure of 20 mm Hg, which allowed filling the left chambers of the heart and maintaining their natural shape. To accelerate the polymerization of silicone, the organocomplex of the heart and lungs was immersed in warm water for 3-4 hours. This injection technique made it possible to maintain the relationship between the original geometry of the aortic root and the intracardiac structures of the left parts of the heart with the A.C. closed. After the silicone hardened, computed tomography of the injected heart was performed, after which modified preparation and morphometry techniques were used.
In all preparations, the circumference of the cross section of the ascending aorta, sinotubular junction (SJ), basal ring of the aorta, the length of the base and height of the intercuspid triangle of the aorta were measured (Fig. 1).
Rice. 1. Photograph of the parameters of the interleaf triangle by A.K. The aorta and left chambers are injected with silicone. 1 — length of the base of the inter-flap triangle; 2 — height of the inter-flap triangle. as well as the magnitude of the deflection angle of the inter-flap triangle (Fig. 2).
Rice. 2. Three-dimensional reconstruction of the AC on a multislice computed tomogram. The angle of deviation (α) of the inter-valvular triangle of the AC from the plane of the longitudinal section of the ascending aorta. The area of the intervessel triangle and AC regurgitation were also calculated using the formulas:
S
tr.=
p
(
p
–
a
)(
p
–
b
)(
p
–
c
),
S
reg.=π·
r
2,
where S
tr.
- area of a triangle; a
,
b
,
c
- sides of the triangle;
p
is the semi-perimeter of the triangle;
where S
reg.
- area of regurgitation; r
is the radius of regurgitation.
Measurement of the angle of deviation of the inter-valvular triangles of the AC from the plane of the longitudinal section of the aortic root was carried out using multislice computed tomography (MSCT) preparations (see Fig. 2). The base of the inter-valvular triangle is a straight line drawn from the lower point of attachment of one semilunar valve to the aortic wall to the lower point of attachment of the other. The apex of the inter-flap triangle is the upper point of the commissure of the AK flap.
After the measurements, the AC valves were assessed for the presence of commissural fenestrations. Particular attention was paid to the areas of the valves at the site of their attachment to the aortic wall and to the apex of the inter-valve triangle. Morphological changes were assessed according to the degree of degenerative changes: degree I - the presence of changes only in the semilunar valves (thinning, discoloration, atherosclerotic changes) without their calcification; II degree - the presence of changes in the semilunar valves (thinning, discoloration, atherosclerotic changes) in combination with fenestrations in the commissural areas of the valves and/or the presence of calcification of the aortic wall; III degree - the presence of changes in the semilunar valves (thinning, discoloration, atherosclerotic changes) in combination with fenestrations in the commissural areas of the valves and the presence of calcification in the inter-valve triangles.
Statistical processing of the obtained data was carried out using the IBM SPSS (Statistical Package for the Social Sciences) program version 20.0 for Windows. The method of multiple logistic regression analysis was used. The level of statistical significance of the differences was taken as 0.05.
Treatment methods for aortic aneurysm
The main method of treating an aneurysm of any part of the aorta is surgical. The point of the method is to replace the dilated section of the aorta in order to prevent its further stretching and rupture. To replace the aorta, two methods are used - the endovascular (intravascular) method using a special intravascular prosthesis (stent graft), and open surgery - aortic replacement.
Each method has its own indications, and each of them has its own advantages and disadvantages.
The advantages of the surgical method lie in its versatility, that is, the ability to correct all disorders associated with an aortic aneurysm, regardless of the department and nature of the lesion. For example, in case of an aneurysm of the ascending aorta and damage to the aortic valve, aortic and aortic valve replacement is performed in combination with coronary bypass surgery.
To perform surgery on the ascending aorta and its arch, it is necessary to use artificial circulation, systemic hypothermia, and often complete circulatory arrest.
Indications for surgical treatment
- transverse size of the aneurysm,
- aneurysm growth rate;
- the formation of complications of this disease.
For each section of the aorta, there is a cutoff limit for the transverse size of the aorta, after which the risk of aortic rupture statistically significantly increases. Thus, for the ascending and abdominal aorta, the transverse diameter of the aneurysm is 5 cm dangerous in terms of rupture, for the thoracic aorta - 6 cm. If the diameter of the aneurysm increases by more than 6 mm in 6 months, then this is also an indication for surgery. Also threatening in terms of rupture and dissection of the aorta are the saccular form of the aneurysm and expansion of the aorta, which is smaller than the diameter that is the indication for surgery, but accompanied by pain at the site of expansion and dysfunction of the presenting organs. Dissections and completed ruptures of aneurysms are absolute indications for emergency surgery.
Statistical method. Statistical methods were used to identify and evaluate risk factors for the following prognoses: annual mean aneurysm growth, complication rates (acute dissection and/or rupture), mortality, and long-term survival.
Survival analysis. Five-year survival estimates were calculated by life table analysis (Kaplan-Meier). Differences in survival were tested using the LIFEREG procedure in SAS version 6.07, 1994 (SAS Institute, Inc, Kari NS).
Kaplan-Meier survival plot. Five-year survival estimates are illustrated for patients with thoracic aortic aneurysms (TAAs) versus the general (age- and sex-matched) population (EA).
Results and discussion. Joyce JW et al. [21] reported a 5-year survival rate of 61% for ascending thoracic aortic aneurysms with a diameter of 6 cm or less; aneurysms larger than 6 cm had a five-year survival rate of 38% of cases. Complete five-year survival in our series was observed in 64% of cases. Mortality is expected to be related to the aneurysm in the vast majority of cases, although adequate details for this distinction have often been unavailable. Survival was significantly lower for descending aortic aneurysms (39% at 5 years) (p=0.031). Patients with dissection had lower survival (46% at 5 years).
Growth parameters. The estimated annual growth rate for thoracic aortic aneurysms was 0.29 cm/year. This is in close correlation with the results reported by Dapunt OE et al. [26] (0.32 cm/year). Masuda Y. et al. [27] reported a growth rate for thoracic aortic aneurysms of 0.13 cm/year. Hirose Y. et al. [28] report a high annual growth rate of 0.42 cm/year for thoracic aortic aneurysms. In a subsequent study, however, Hirose Y. et al. [28] gave a significantly lower rate.
The discrepancy between the two studies [28] may well explain the different strategies used to estimate growth. In recent studies by Hirose Y. [28], the regressions used are close to those used by Dapunt OE et al. [26] and in the current study, when assessing the growth of a thoracic aortic aneurysm. Earlier studies by Hirose Y.'s group [28] calculated that height is equal to the difference between the last and first measured size divided by the duration between studies.
Size has traditionally been considered an important risk factor for complications (ie, acute dissection and/or rupture) in patients with thoracic aneurysms, and it has been considered the most important independent factor in the decision to undergo elective surgery. The effect of size on the rate of growth of aneurysms is a matter of debate. Dapunt OE et al. [26] note that more intense dilations were found in those patients whose aortic diameter at diagnosis was >5 cm. On the other hand. Hirose Y. et al. [28] found no significant effect of size on growth rate.
Dapunt OE et al. [26] reported that the presence of hypertension correlates with a large aortic diameter, but does not significantly affect the rate of aortic enlargement growth. Masuda Y. et al. [27] reported a direct relationship between the magnitude of diastolic pressure and the degree of aortic dilatation.
Possibility of complications. It is important to consider the natural history of patients with thoracic aneurysms, e.g. cases of acute dissection and/or rupture in this population. Pressler V., McNamara JJ [22] reported that in eight of nine cases of ruptured descending thoracic aortic aneurysms, the aortic size was greater than 10 cm. Subsequent studies reported complications with much smaller sizes. A study by Gott VL et al [11] of ascending aortic aneurysms in patients with Marfan syndrome reported a mean size of 7.8 cm at the time of dissection.
However, in seven of 26 patients (26.9%), dissections were observed with aneurysms measuring 6.5 cm or smaller. In addition, Crawford ES et al. [9] reported a mean size at rupture of 8.0 cm among 117 patients with descending thoracic and thoracoabdominal aneurysms. Dapunt OB et al. [26] report ruptures of thoracic aneurysms occurring in even smaller sizes, with an average size of 6.1 cm.
These observations indicate dissections or ruptures as aneurysms expand in size. The average size at the time of rupture or dissection was 6.0 cm for ascending aneurysms and 7.2 cm for descending aneurysms. A multivariate retrospective analysis was performed to isolate risk factors for acute dissection or rupture, which showed that a size greater than 6.0 cm increased the likelihood of dissection or rupture by 32.1% for ascending aneurysms (p=0.005). For descending aneurysms, this probability increased by 43% for sizes greater than 7.0 cm (p=0.006). Frist WH et al. [33] provide the following data for ascending and descending aneurysms: 6 cm for the ascending aorta and 7 cm for the descending aorta.
Criteria for surgical intervention.
Below we have attempted to demonstrate the importance of the thoracic size of the aneurysm in dire complications such as aortic rupture and dissection. Our observations attempt to demonstrate a clearly increasing incidence of complications with increasing aortic size. These observations indicate that the average size at rupture and dissection is 6.0 cm for ascending aneurysms and 7.2 cm for descending aneurysms. Multivariate analysis of risk factors affecting acute dissection and/or rupture shows that size greater than 6.0 cm is a significant risk factor (p=0.005). Logistic analysis indicated a 32.1% increase in the likelihood of dissection or rupture for ascending aneurysms with a mean size greater than 6.0 cm (p=0.005) and a 43.0% increase for descending aneurysms greater than 7.0 cm (p=0.006).
These data strongly call for the use of a size criterion for surgical replacement of aneurysmal aorta to prevent complications of rupture and dissection. Additionally, these data suggest that a lower size criterion than previously recommended should be used.
If the average size at the time of complication (in this case: 6.0 cm for the ascending and 7.2 cm for the descending aorta) is used as an intervention criterion, then half of the patients are likely to experience serious complications during the intervention. Accordingly, the authors suggest intervention for slightly below average size criteria at the time of complication. It is suggested that surgical intervention be used for 5.5cm ascending and 6.5cm descending aortic aneurysms. These above criteria allow intervention to occur before the catastrophically increased likelihood of rupture and/or delamination.
These recommendations indicate that elective surgery is much safer than emergency surgery. For ascending aneurysms and aortic arch aneurysms, elective surgery was very safe (mortality rate 4.3%). These mortality results are broadly consistent with those reported by other centers. Although surgery on the descending aorta has a higher risk (19%), the number of patients in this category is relatively smaller to influence the final outcome.
Many of the above data have shown that surgery on the ascending aorta is safer. CPB via left atriofemoral cannulation using a centrifugal pump has been shown to be a safe and reliable method for preventing postoperative complications such as ischemic complications such as renal failure and spinal cord injury. In addition, the advent of a protease inhibitor (aprotinin) led to a significant reduction in blood loss as a result of the protection of platelet wall receptors at the beginning of CPB. The introduction of a collagen-impregnated Dacron graft has led (Hemashield Meadox Medicals Inc, Oakland, NJ) to improve surgical hemostasis, essentially eliminating bleeding through the graft wall. These facts support priority selective intervention to avoid rupture and dissection of aneurysms.
For descending aortic aneurysms, the risk of paraplegia should be considered as a significant intraoperative complication. The risk of paraplegia (spinal origin) in the literature remains between 2 and 20%, in this case it is 4.0%. Obviously, advanced age and concomitant diseases can lead to frequent complications for which surgical intervention is not indicated. Thus, each patient must be assessed individually, and the expected risk of complications (especially paraplegia in descending aortic aneurysms) must be weighed to avoid complications such as rupture and dissection. In addition, the level of doctors in the medical center in question must be taken into account. The size criteria presented here are suggested for less severely ill patients treated at more experienced centers.
Studies of patients with Marfan syndrome.
More than 90% of deaths in Marfan syndrome are due to complications of ascending aortic aneurysms. Because most patients with Marfan syndrome have some degree of aortic regurgitation (aortic root 6.0 cm), Gott, Lima et al recommend prophylactic treatment for aneurysms that reach 5.5 to 6.0 cm. We recommend an intervention criterion of 5.0 cm for patients with Marfan syndrome, other hereditary collagen vascular diseases, or familial cases of aortic regurgitation.
This size criterion is slightly lower than the recommendations for intervention for atherosclerotic aneurysms of the ascending aorta. Experience has shown that in several patients with Marfan syndrome the dissection or rupture occurred at sizes less than 5.0 cm. These young patients were often in severe clinical condition. Thus, prophylactic surgical treatment can significantly improve their clinical condition and prognosis.
Developing intervention criteria is a complex research endeavor. Research into this problem is important to improve patient survival. To determine appropriate size criteria for the intervention, we used statistical analysis. These intervention criteria should take into account the patient's age, physical condition, life expectancy, that is, approach the intervention criteria using statistical methods in terms of preventing complications (dissection and rupture). Organ pressure from the aneurysm, concomitant aortic regurgitation, and acute aortic dissection are widely accepted common indications for surgical intervention regardless of aortic size.
Some points of view are still debated in the surgery of chronic ascending aortic disease: which technique to use in treatment (open or wrap technique, direct or indirect reimplantation of the coronary arteries), how to protect the brain during the restoration of the aortic arch. When the aortic root was included in the surgical plan, implantation of a valved conduit was typically performed using a wrap technique with coronary artery reimplantation and a Dacron graft (8mm). Valve replacement alone does not protect against recurrence of ascending aortic aneurysm, leading to reoperation. However, repeated operations have a high mortality rate.
Some authors have used the wrapper technique. Regarding bleeding, the probability of early reoperation is low - 4.5% in this series and can be compared with the data of Kouchoukos N. (2% - open technique). In the studied patients there was no need for repeated operations for pseudoaneurysms of the ascending aorta.
Coronary reimplantation using a Dacron graft (8mm) appears to be more reliable and technically feasible than direct reimplantation or reimplantation with aortic buttons. Kouchoukos N. [7] Taniguchi K. et al. [12] reported the appearance of pseudoaneurysms in the coronary ostium after these operations [12,13].
It is therefore believed that the use of a Dacron graft prevents these complications (as shown by standard coronary angiography). The resulting right atrial fistulas closed, with the exception of one case where reoperation was required. Nine cases in which a tubular graft was implanted resulted in sudden death of unknown cause (no autopsy was performed). The possibility of false aneurysms or fistulas leading to death was not excluded.
Aortic arch repair is always indicated when the aneurysm extends into the aortic arch, when the dissection extends into the arch, or when the intimal tear is localized to the arch (2 cases in this series). The authors believe that stopping hypothermic CPB leads to neurological complications. Griepp RB et al. reported a rate (5.6%) of neurological complications in 87 patients [15]. The authors prefer stopping hypothermic CPB during selective catheterization of the great vessels of the brain.
30-day mortality was observed in 7.6% of patients and 6% in patients with prosthetics (valve-containing conduits were used). Galloway AC et al. [6] reported similar case fatality rates of 5.3 and 5%, respectively.
Many analyzes also indicate that concomitant coronary artery transplantation and older age are major risk factors, as has been shown by other authors. Survival is poor in patients undergoing surgery for chronic ascending aortic disease: 48% at 12 years in Kouchoukos NT et al. [13] and 57% over 7 years in Culliford AT [34]. In this series, complete survival was 59.6% ± 3.7% over 9 years for all patients and 66.3% ± 4.5% over 9 years for patients with prosthetics with a valve-containing conduit (intraoperative mortality was also included).
The predominant cause of late mortality was not found in this series. Factors that increase risk as shown by univariate analysis are: CPB time, aortic arch repair, chronic aortic dissection, and older age.
Conclusion
Types of open surgical operations for aortic aneurysms:
- Bentalla-De Bono operation (replacement of the ascending aorta with a valve-containing conduit with a mechanical prosthetic aortic valve);
- David's operation (replacement of the ascending aorta while preserving the native aortic valve);
- Supracoronary aortic replacement;
- Prosthetics of the ascending aorta and its arch (Borst technique, the use of oblique aggressive anastomosis and other techniques);
- Thoracic aortic replacement;
- Abdominal aortic replacement.
Endovascular interventions
They allow you to dramatically reduce the amount of surgical trauma, shorten hospitalization periods and reduce the inevitable suffering of the patient associated with surgical approaches. One of the main disadvantages of the method is the need for repeated interventions.
Types of endovascular operations for aortic aneurysm:
- implantation of a stent graft into the abdominal aorta,
- implantation of a stent graft into the ascending (thoracic) aorta.
The most modern method of treating aortic aneurysm is a hybrid method, which allows achieving optimal treatment results with the least surgical trauma.
Hybrid surgeries combine the advantages of open and endovascular interventions.
To prevent the development of aortic aneurysms, the most important thing is the need to control risk factors, namely arterial hypertension. In addition to arterial hypertension, the most significant risk factors are age (over 55 years), male gender, smoking, the presence of aneurysms in direct relatives, and high cholesterol levels.