Mitral valve plastic surgery is performed for pathologies of this part of the heart that cannot be cured with conservative methods. Reconstruction of the valve allows you to restore all its functions, prevent heart failure, and save the patient’s life. During the operation, plastic structures are used to completely rehabilitate the heart and avoid repeated problems with the valve. The procedure has its own characteristics, preparation and recovery rules.
Causes of development of mitral valve defects
The disease may be based on fundamentally different defects in the valve structures. To choose effective treatment tactics, it is important to accurately determine the form of the defect and the cause of its development.
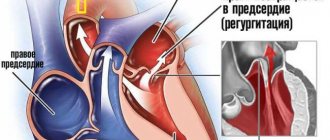
- Valve leaflet defects often occur with infective endocarditis and myocarditis, and rheumatic heart disease. Perforated, loosely closing leaflets are not able to hold blood in the left ventricle during heart contractions. The blood is pumped back into the left atrium and then into the lungs.
- Fusion of valve leaflets . The most common cause of mitral stenosis is rheumatism (acute rheumatic fever); less commonly, this defect develops after infective endocarditis or heart injury. The calcified valves, welded together, impede the normal flow of oxygen-enriched blood into the left ventricle and further to the tissues and organs.
- Rupture of the chordae tendineae most often occurs in systemic connective tissue diseases and acute endocarditis. The valve leaflets move (prolapse) into the atrium, reducing the efficiency of the heart.
- Rupture or sclerosis of the papillary muscles is an acute, life-threatening condition that develops with infarction of the papillary muscles against the background of coronary heart disease (CHD) or heart tumors. When the papillary muscles are damaged, the valve leaflets lose their fixation point, and the valve completely stops functioning.
Restoring mobility of valves and chords
Limitation of the movement of the leaflets is caused by fibrous thickening of the subvalvular apparatus, the leaflets themselves, commissure fusion and calcification. In most patients, with pronounced changes in these structures, valve replacement is necessary, but in some patients with limited calcification of the leaflets and fibrosis of the subvalvular structures, open commissurotomy can be performed. The dissection of fused leaflets along the commissures should end 2 mm from the annulus, since a more extensive commissurotomy can lead to mitral insufficiency. Additionally, to increase the mobility of the valves, fenestration of the primary chordae and papillary muscles is performed, as well as resection of the secondary chordae.
Fenestration of the primary chordae and papillary muscles Mobilization of the subvalvular structures significantly increases leaflet mobility and the effective orifice area of the mitral valve. If a hydraulic test after completion of the manipulation reveals regurgitation, additional implantation of a corrective ring may be necessary.
Approaches to the treatment of mitral valve defects
The first step in treating clinically significant mitral valve disease is drug therapy. It includes drugs that slow down the heart and reduce the force of its contractions (beta blockers), antiplatelet agents and anticoagulants, antibacterial and anti-inflammatory drugs for infectious etiologies of the defect. Drug therapy improves the patient’s condition to a certain extent, but only high-quality surgical correction of the mitral valve can radically eliminate the cause of the disease.
Depending on the form of the defect, cardiac surgeons use one of the following procedures:
- Annuloplasty is the replacement or reconstruction of the support ring that surrounds the mitral valve and securely fixes it between the left atrium and the ventricle.
- Chordplasty – restoration of the integrity of damaged tendinous chords or their lengthening.
- Commissurotomy is the surgical separation of fused valve leaflets.
- Valve leaflet plastic surgery – correction of the shape, size or anatomical position of the valve leaflets.
- Prosthetics is the complete replacement of a damaged mitral valve with a biological or mechanical prosthesis.
According to the results of multicenter clinical studies and practical experience of leading cardiac surgery centers, preference is given to robotic surgery using the daVinci system and catheter surgical techniques.
Annuloplasty
Typically, dilatation of the mitral valve annulus occurs due to its posterior part, since the anterior part of the annulus is connected to a rigid structure - the interventricular septum. Revision of the mitral valve makes it possible to determine the possibility of performing plastic surgery: the valves must be sufficiently mobile without pronounced prolapse. To select the size of the ring, a special calibration device (template) is used, which allows, based on measuring the length of the base of the anterior leaflet of the mitral valve, to determine the required size of the plastic ring. Subsequently, mattress sutures are placed along the entire perimeter of the valve ring and parallel to it to a depth sufficient to capture the fibrous ring. In this case, it is necessary to avoid damage to structures located in direct contact with the mitral valve annulus. Different types of rings are used: rigid, flexible, full or partial. The use of rigid rings is mandatory for mitral regurgitation of ischemic origin, especially with ischemic cardiomyopathy, since the rigid structure is more reliable in the isolated postoperative period. For the same purpose, rings of small (No. 26-28) sizes (hypercorrection) have recently been more often used for plastic surgery for ischemic mitral insufficiency. The ring is fixed according to the marks dividing it in accordance with the normal anatomical ratio of the length of the base of the anterior (1\3) and posterior (2\3) cusps of the mitral valve.
Technique of annuloplasty on a rigid ring: 1 – determination of ring size; 2 – suturing along the perimeter of the mitral valve; 3 – ring fixation For annuloplasty, it is possible to use incomplete rings (rigid or flexible) or a strip of biological or synthetic material 46-52 mm long with fixation along the posterior 2/3 of the circumference of the mitral valve. Mattress sutures are carried out by capturing the fibrous ring and overlapping each other by 1/2, which provides additional strength of fixation.
Technique of annuloplasty on a half ring: 1,2 – diagram of sutures; 3.4 – fixation of the half ring At the final stage, the tightness of the valve must be monitored by injecting saline solution under pressure into the cavity of the left ventricle. Detection of significant regurgitation during the test requires revision of the subvalvular structures, since regurgitation is a consequence of incomplete cooptation of the leaflets due to prolapse of one of them.
Carrying out a hydraulic test of valve tightness It is possible to apply an additional suture according to O. Alfieri at the site of regurgitation. It must be remembered that this method can lead to stenosis of the atrioventricular orifice if the ring for plastic surgery is selected in a small size (No. 26-28). Dissatisfaction with the results of plastic surgery is an indication for prosthetic replacement already at this stage of the operation. Additional monitoring of the effectiveness of the plastic procedure is carried out using transesophageal echocardiography after restoration of cardiac activity.
daVinci Robotic Surgery - a combination of surgeon experience and robotic precision
Robotic surgery using the daVinci system allows you to successfully perform both reconstructive surgeries and complete mitral valve replacement. Such interventions combine the advantages of minimally invasive surgery and high precision of manipulation due to computer control of endoscopic instruments.
Patients receive a number of important benefits when using the daVinci robot:
- Shorter hospitalization period (up to 7 days).
- Short stay in the intensive care unit.
- Low risk of bleeding, no need for transfusion of blood and its components.
- Low risk of reactive postoperative pericarditis and pleurisy.
- Rapid restoration of physical activity (the next day after surgery, the patient can move around the clinic).
- Invisible postoperative scars measuring 1-2 cm, the chest is not opened.
The daVinci robot has over 20 years of experience. During this time, the system has undergone a number of modifications to improve the functional and aesthetic results of treatment. Modern cardiac surgery centers use the latest modification of the robot – da Vinci Xi®. To date, it is the only robotic device approved by the FDA for mitral valve surgery.
Relative limitations to the use of the daVinci system include the high cost of the equipment and the small number of qualified cardiac surgeons who are fluent in the technique of working with it. Also, endoscopic interventions are not performed in patients with pulmonary hypertension, aortic stenosis or insufficiency, severe liver dysfunction.
Rehabilitation period
After replacing the mitral valve using catheterization, the patient is transferred to the intensive care unit. Within a few hours he can get out of bed and walk independently. The average length of hospital stay after surgery is about 5-7 days. To prevent the formation of thrombosis, regardless of the type of transplant, a course of blood thinning drugs is prescribed. It is recommended to avoid intense physical activity and stress for a month.
An individual cardiac rehabilitation program is developed for each patient, including a course of physical activity aimed at stabilizing the functioning of the cardiovascular system, the formation of a dietary menu, and psychological support.
In our clinic you are guaranteed high-quality medical care and individual solutions for creating treatment programs for cardiovascular diseases for each patient.
NeoChord – plastic surgery of chordae tendineae on a beating heart
The development of the NeoChord DS1000 system was the result of numerous clinical studies that demonstrated the superiority repair over complete replacement . NeoChord DS1000 has been successfully used for repair of chordae tendineae in patients with severe mitral regurgitation due to mitral valve prolapse.
The procedure is performed under general anesthesia, through a mini-thoracotomy access (incision length no more than 5-6 cm). In this case, the patient is not connected to a heart-lung machine; the heart maintains its natural rhythm.
Under strict visual guidance using 2D or 3D transesophageal echocardiography, the NeoChord DS1000 system is inserted into the left ventricle. The cardiac surgeon replaces the damaged chord with an artificial one and controls its tension. At the same time, the movement of the valve leaflets is reflected on the echocardiograph monitor in real time - this allows you to immediately evaluate the result of the operation and, if necessary, correct the position or tension of the chord.
To date, the NeoChord procedure has been successfully performed on more than 1,000 patients in Europe and the USA. The results of long-term postoperative follow-up confirm the safety of the technique and its effectiveness in the correction of mitral valve prolapse.
Reviews from doctors
Professor Ran Kornovsky, Director of the Institute of Invasive Cardiology at Beilinson Hospital: “I am very pleased that we were able to perform valve replacement surgery quickly and gracefully, with minimal harm to the patient. To date, less than 20 such procedures have been registered worldwide and none in Israel. In this way, we continue to build on the already extensive experience we have acquired in the field of heart valve replacement through catheterization and other varied and complex procedures.”
Professor Alik Sagi, Director of the Institute of Echocardiography (Echography) and the Valve Diseases Clinic at Beilinson Hospital: “This is a real revolution. Repeated surgical interventions on the heart in patients who have previously undergone similar operations are associated with a long and difficult recovery process, sometimes stretching for several months. Two days after our procedure, the patient was already moving around the department, and we observed a significant improvement in her clinical condition.
MitraClip – gentle one-stage reconstruction of the mitral valve leaflets
MitraClip technology is also used as part of the “Respect when you can, resect when you should” approach to cardiac surgery, which demonstrates the benefit of reconstructing a patient's native mitral valve over replacing it with an artificial prosthesis.
The MitraClip system allows you to firmly connect deformed or damaged valve leaflets using a microsurgical clamp made from an alloy of durable and metabolically inert metals - cobalt and chromium. During the procedure, the MitraClip is inserted into the femoral vein and moved into the left atrium under echocardiography guidance. This method of inserting a catheter into the heart does not require opening the chest and significantly reduces operational risks.
MitraClip securely fixes the valve leaflets in the required position, restoring normal blood flow from the left atrium to the ventricle. Using intraoperative echocardiography, the cardiac surgeon immediately assesses the quality of the reconstructed valve and, if necessary, installs an additional clamp.
Thanks to the successful results of clinical studies (European COAPT and EVEREST II studies), the MitraClip technique has been included in updated medical guidelines for the surgical treatment of mitral regurgitation. The MitraClip system is recommended for use in older patients with high surgical risks - such an operation is easier to tolerate compared to classic open cardiac surgery, but cannot fully replace complex reconstruction of the mitral valve.
Resection of valves
Manipulation is carried out mainly on the posterior leaflet, since it most often prolapses with myxomatous valve degeneration. During echocardiography and during intraoperative revision of the mitral valve, the prolapsed part of the leaflet is detected (most often this is the P2 portion - PM). Its quadriangular resection is performed along with elongated or torn chords. The resulting gap in the ring is closed with 1 or 2 seams on spacers. Ring plication is the most important technical point of the operation, since it should not only reliably ensure the approximation of the resected parts of the valve, but also not lead to deformation of the a.circumflexa. When tying ring plicating sutures, care must be taken to ensure that the edges of the sash are not overly stretched. The sash is sewn with a continuous seam using 5\0 thread. The mitral ring after quadriangular resection is necessarily strengthened with a hard or soft corrective ring.
Quadriangular resection of the posterior mitral valve leaflet Sliding resection of the posterior mitral valve leaflet was proposed by A. Carpentier to prevent left ventricular outflow tract obstruction syndrome caused by anterior systolic movement of the anterior mitral valve leaflet. This syndrome develops in 5-10% of patients after quadriangular resection of the posterior leaflet. It is caused by the excess volume of tissue in the wing sails. After resection of the posterior leaflet and implantation of the ring, the cooptation line moves forward, as a result of which the long anterior leaflet narrows the outflow tract from the left ventricle. More often, the syndrome develops after implantation of rigid correction rings. Left ventricular outflow tract obstruction syndrome is provoked by hypovolemia, vasodilation and the use of inotropic drugs. In uncomplicated cases, volume loading, increased afterload, and withdrawal of inotropes are sufficient to reduce or eliminate the hemodynamic consequences of this syndrome, which undergoes regression over time. The best strategy in patients with a potential development of left ventricular obstruction syndrome is to supplement quadriangular resection with a sliding resection of the posterior leaflet. In patients with excess leaflet tissue (posterior leaflet height greater than 1.5 cm), the goal of performing a sliding resection of the posterior leaflet is to reduce its height in order to move the leaflet cooptation line posteriorly. After quadriangular resection, the base of the posterior leaflet is separated from the ring at a distance of 1.5-2 cm on both sides of the resection site. Plicating sutures are placed on the mitral valve annulus, after which the leaflet is sutured to the reduced posterior part of the mitral valve annulus with 4/0 suture. The operation is complemented by implantation of a corrective ring. This procedure virtually eliminates the risk of left ventricular outflow tract obstruction syndrome in patients with degenerative mitral valve disease.
Technique for performing sliding resection of the posterior leaflet. 1 - the arrow indicates the location of obstruction of the left ventricular outflow tract; 2,3,4 - stages of the operation In Barlow's disease, bullous deformity and prolapse of not only the posterior but also the anterior leaflet of the mitral valve often develop. In this situation, simultaneously with quadriangular resection of the posterior leaflet, a triangular resection of the anterior leaflet of the mitral valve is performed, followed by suturing the edges with a continuous 5\0 suture. An integral element of the operation is strengthening the created structure with a soft or hard ring.
Resection of the anterior (triangular) and posterior (quadriangular) mitral valve leaflets In patients with mitral annulus calcification, decalcification is necessary to facilitate implantation of a corrective ring. To facilitate debridement, the posterior leaflet can be separated from the ring as in a sliding resection. After removal of calcifications when there is a threat of formation of a dissecting aneurysm of the left ventricle, the area where debridement was performed is covered with a pericardial patch, to which the bases of the mitral valve leaflets are sewn.
Clinics and treatment costs
For successful minimally invasive mitral valve reconstruction, two main points are important: the availability of equipment and sufficient experience of the surgeon. Among the multidisciplinary and cardiology clinics that accept patients from all over the world, it is worth noting the following:
- University Hospital Oldenburg, Department of Cardiac Surgery
- University Hospital Essen, Department of Cardiothoracic Surgery
- University Hospital Ulm, Department of Cardiothoracic Surgery
- University Clinic named after. Goethe Frankfurt am Main, Department of Cardiothoracic Surgery
- University Hospital Tübingen, Department of Adult and Pediatric Cardiothoracic Surgery
The estimated cost of treatment is:
- Diagnosis of mitral valve insufficiency or prolapse – from €467
- Treatment of mitral valve insufficiency or prolapse with minimally invasive reconstruction – from €10,025
- Treatment of mitral valve insufficiency or prolapse using minimally invasive prosthetics – from €10,082
- Treatment of mitral valve insufficiency or prolapse using the Mitralign system – from €29,066
- Treatment of mitral valve insufficiency or prolapse using the Carillon system – from €27,326
- Cardiac rehabilitation – from €566
The exact cost of treatment can be determined after an initial consultation, assessment of the patient’s condition and selection of surgical technique. The cost of treatment is also affected by the presence of concomitant diseases and the need for rehabilitation after completion of the main course of treatment.
Send a request for treatment
Indications and contraindications for surgery
Indications:
- congenital heart defects;
- lack of results of drug treatment for chronic heart failure accompanying mitral valve stenosis;
- fainting with aortic stenosis;
- aortic valve stenosis, manifested after coronary artery bypass grafting;
- valve calcification.
Contraindications:
- heart attack;
- stroke;
- extreme degree of heart failure with mitral valve stenosis;
- endocarditis.
Competent choice of clinic and cardiac surgeon is the basis for successful treatment
One of the keys to successful mitral valve surgery is a thorough preoperative examination and selection of an appropriate surgical technique. This is possible in a specialized cardiac surgery center or a large multidisciplinary university-level clinic, where doctors are not limited in equipment for carrying out innovative interventions. Most often, clinics in European countries with developed healthcare systems have such capabilities.
If you have chosen a prestigious foreign clinic, then you should take into account the specifics of registering for treatment for foreign patients - the need to receive an invitation from the clinic, preparation and translation of medical documentation, waiting for hospitalization for several months, paying for medical services at a higher rate, and so on. . To go through all stages of the medical program more comfortably and safely, you can use the services of Booking Health.
Booking Health is the only certified medical tourism operator in the world (ISO 9001:2015 certificate), which has been organizing treatment for patients from 75 countries in leading clinics in the world for more than 10 years. Booking Health specialists will help you with such important points:
- Choosing the right clinic based on the annual qualification profile
- Direct communication directly with the attending physician
- Preliminary preparation of a treatment program without repeating previously conducted examinations
- Ensuring favorable prices for clinic services, without surcharges and coefficients for foreign patients (savings up to 50%)
- Make an appointment for the desired date
- Control of the medical program at all stages
- Assistance in purchasing and shipping medications
- Communication with the clinic after completion of treatment
- Control of invoices and return of unspent funds
- Organization of additional examinations
- Service of the highest level: booking hotels, plane tickets, transfers
Leave a request with medical and contact information on the official Booking Health portal, and a competent consulting doctor or medical coordinator will contact you on the same day.
Edge-to-edge plastic surgery
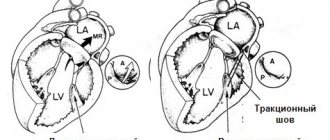
O. Alfieri et al. (2001) proposed a method for eliminating prolapse of the anterior leaflet of the mitral valve using a suture attaching the prolapsed part of the anterior leaflet to the unchanged posterior leaflet (Fig.). This maneuver creates a double-lumen atrioventricular opening, limits the mobility of the anterior leaflet and ensures the tightness of the valve. Subsequently, the O. Alfieri suture began to be used as an addition to create better MV competence in case of inadequacy of other plastic procedures on the mitral valve.
Technique for performing edge-to-edge plastic surgery according to O. Alfieri