Medical significance of the oscillometric method of measuring blood pressure
Unfortunately, these so-called “major vascular diseases” are very common in Western European countries.
In the United States, the annual number of cases of myocardial infarction reaches 900 thousand, in the UK - 225 thousand;
in Germany - 275 thousand people suffer from this acute coronary disease. 40 - 50% of all these patients die during the initial 4 weeks of the post-infarction period. About 420 thousand patients in the United States, about 100 thousand in the UK and about 125 thousand patients in Germany suffer from stroke. 50% of them cannot continue their professional activities due to brain damage. Stroke and myocardial infarction account for 45% of all deaths in Western Europe. To prevent many diseases and maintain your health, along with such measures as a healthy lifestyle, balanced diet, control of cholesterol levels in the blood, quitting smoking, it is necessary to prevent an increase in blood pressure for as long a period of time as possible.
High blood pressure, however, is quite common. In developed countries, the overall prevalence of this disease reaches 20%. In the United States, for example, 56 million people suffer from this disease. The corresponding figures for Great Britain are 13 million, and for Germany about 16 million. Fortunately, modern medicine offers a wide range of therapeutic measures, including diet, physical activity, and pharmaceutical interventions. Any therapy, however, requires, first of all, a correct diagnosis of arterial hypertension. Only a doctor can make a correct diagnosis. Unfortunately, results obtained in the doctor's office alone are not sufficient to accurately diagnose hypertension: First, patients in the doctor's office are often subject to the so-called "white coat effect", which leads to an artificial increase in the patient's blood pressure level. Secondly, working patients do not have the opportunity to visit a doctor frequently. Therefore, when assessing blood pressure levels during the day, patients need to measure their blood pressure themselves. Measurements can be taken both at the workplace and at home. Measurement data should be entered into a “measurement diary” and presented to the doctor during visits. Today, there are two methods for measuring blood pressure: using automatic tonometers that measure pressure using the oscillometric method and using devices that measure pressure using the auscultatory method. The auscultatory method of measuring blood pressure, also called the Riva-Rocci method, is based on the detection of arterial pulsation sounds, heard as the blood tone passes under a cuff wrapped around the patient's shoulder. Most auscultatory devices are hand-held devices, that is, patients use a stethoscope to listen to the sounds of the pulse and determine the systolic and diastolic pressure based on the nature of the sound. This method only works well if patients are properly trained and have the appropriate experience. Unfortunately, many patients suffering from arterial hypertension are elderly. They often have reduced hearing and are unable to properly use hand-held auscultation devices. There are several automatic auscultatory tonometers on the market. Their disadvantage is their high sensitivity to noise interference. The microphone, which is part of these devices, perceives various sound signals that interfere with correct measurements. More than 10 years have passed since the oscillometric measurement method began to be used in devices for measuring blood pressure. This technique allows you to assess the level of arterial pressure using a cuff placed on any limb. When measuring at home, pressure is measured either at the shoulder or at the wrist. Shoulder devices show more accurate results. There is a camera inside the cuff that detects pulse changes in the flow of blood passing just under the cuff. All changes in pressure are recorded during the measurement. The oscillometric method has two main advantages:
- patients do not need to have the skills to interpret the nature of pulse changes
- patients do not have to engage in self-assessment of sound signals
In this case, it is important to observe some basic conditions: take measurements only at rest, any movements should be excluded, and the cuff should be at the level of the heart. No special skills are required for these measurements. Today, the buyer is offered a wide range of oscillometric instruments. The accuracy of these devices is very high, but it is not the same among different manufacturers, which is due to the design features of the devices and the use of technology in their production.
This refers to the degree of possibility:
- suppression of extraneous noise
- correct interpretation of heart rate changes
- low heart rate measurements
- measuring very low or very high pressure
Due to incorrect behavior of patients during measurement, in particular due to lack of rest, the result of one measurement differs from another. Such errors are not a technology error; they are caused by the instability of the pressure level itself. Since the pressure level changes dynamically, one-time measurements should not be practiced. To find out the true level of pressure, it is necessary to take a series of repeated measurements. It is very important that patients undergoing treatment for high blood pressure prepare materials with measurement data for their treating physicians (keeping measurement diaries). They play a significant role in prescribing further treatment.
Conclusion: Oscillometric blood pressure measurement technology is reliable for accurately assessing blood pressure levels in patients suffering from hypotension or hypertension. Despite some technical and psychological limitations, this technology has important medical significance and is unique. Klaus Forstner
Doctor, MD cd Dipl.-Ing. Tamm, May 16th, 2002
Challenges and advances in blood pressure measurement
U
blood pressure level is one of the main indicators of central and regional hemodynamics, reflecting the blood supply to vital organs.
An increase in blood pressure is observed already in childhood and adolescence (in 1–14% of children). Subsequently, a third of these children develop persistent arterial hypertension. The prevalence of arterial hypertension in the Russian Federation among adults reaches 40%, and in older age categories exceeds 80%
. The presence of arterial hypertension causes a high risk of developing coronary heart disease, heart failure and cerebrovascular disease and increases overall mortality and mortality from cardiovascular diseases by 2–8 times. Arterial hypertension leads to the formation of renal failure, contributes to damage to peripheral arteries, retinal vessels, and the development of pathology in pregnant women and newborns. At the same time, there is unsatisfactory awareness of the population about the presence of the disease, a low percentage of patients receiving treatment, and an insufficient effect of antihypertensive therapy. At the same time, data from numerous clinical studies (ELSA, EWPHE, FACET, HOT, LIFE, MRC, PROGRESS, SHEP, UKPDS, etc.) have convincingly proven that achieving an optimal level of blood pressure during treatment and influencing other risk factors improves the quality life, reduces mortality from complications of arterial hypertension.
Currently, international and national recommendations have been developed for the prevention and treatment of patients with arterial hypertension. Depending on the level of blood pressure, approaches to the examination and management of such patients, as well as the course and outcome of the disease, change. Emergency conditions in the clinic of internal diseases (cardiogenic shock, coma, syncope, hypertensive crisis, eclampsia in pregnancy), hemodynamic control during anesthesia and resuscitation, and functional tests require an accurate assessment of systolic (SBP) and diastolic (DBP) blood pressure. Thus, the determination of blood pressure must be strictly regulated, which imposes certain requirements both on the conditions for its measurement and on the recording devices themselves.
According to the recommendations of WHO/IOG (1999) and VNOK (2001), when measuring blood pressure, the following conditions must be met:
the patient should be in a sitting position, in a comfortable position, the measurement is carried out at rest after a 5-minute rest. It is advisable to avoid drinking coffee and strong tea (within an hour before the test), smoking (within 30 minutes), and using sympathomimetics (including nasal and eye drops). The cuff should be placed on the shoulder at the level of the heart so that its lower edge is located 2 cm above the elbow. The rubber part of the cuff must be at least 2/3 of the length of the forearm and at least 3/4 of the circumference of the arm. Blood pressure measurements on each arm should be carried out at least 3 times with an interval of at least a minute, and the average of the last two measurements is taken as the final blood pressure. Before measurement, the air in the cuff is quickly inflated to a value exceeding systolic blood pressure by 30 mm Hg. (by disappearance of the pulse), and the decompression rate is 2 mm Hg. per second. During the initial examination, the pressure is determined on both arms; subsequently, the measurement is made on the arm with higher blood pressure. In elderly patients (over 65 years of age), patients with diabetes mellitus and those receiving antihypertensive therapy, blood pressure should also be measured in a standing position to exclude orthostatic hypotension.
Methods for measuring blood pressure
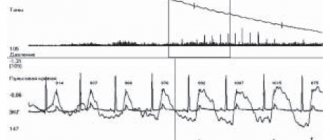
The invasive (direct) method of measuring blood pressure is used only in inpatient settings during surgical interventions, when the introduction of a probe with a pressure sensor into the patient’s artery is necessary to control the pressure level. The advantage of this method is that the pressure is measured continuously, displayed as a pressure/time curve. However, patients with invasive blood pressure monitoring require constant monitoring due to the risk of severe bleeding in case of probe disconnection, hematoma formation or thrombosis at the puncture site, or infectious complications.
Invasive
Non-invasive methods have become more widespread in clinical practice.
methods for determining blood pressure. Depending on the principle underlying their work, palpation, auscultation and oscillometric methods are distinguished.
Palpation
the method involves gradual compression or decompression of the limb in the area of the artery and palpation of it distal to the site of occlusion. One of the first devices, proposed in 1876 by S. Basch, made it possible to determine systolic blood pressure. In 1896, S. Riva–Rocci proposed the use of a circumferential compression cuff and a vertical mercury manometer for the palpation method. However, a narrow cuff (only 4–5 cm wide) led to an overestimation of the obtained blood pressure values by up to 30 mmHg. After 5 years, F. Recklinghausen increased the width of the cuff to 12 cm and in this form this method exists to this day. The pressure in the cuff rises until the pulse stops completely, and then gradually decreases. Systolic blood pressure is determined by the pressure in the cuff at which the pulse appears, and diastolic blood pressure is determined by the moments when the filling of the pulse noticeably decreases or an apparent acceleration of the pulse occurs (pulsus celer).
Auscultatory
the method of measuring blood pressure was proposed in 1905 by N.S. Korotkov. A typical Korotkoff blood pressure device (sphygmomanometer or tonometer) consists of an occlusive air cuff, an air inflation bulb with an adjustable deflation valve, and a device that measures the pressure in the cuff. As such a device, either mercury pressure gauges, or aneroid-type pointer pressure gauges, or electronic pressure gauges are used. Auscultation is performed with a stethoscope or membrane phonendoscope, with the sensitive head located at the lower edge of the cuff above the projection of the brachial artery without significant pressure on the skin. SBP is determined during cuff decompression at the moment the first phase of Korotkoff sounds appears, and DBP is determined at the moment they disappear (fifth phase). The auscultatory technique is currently recognized by WHO as a reference method for non-invasive determination of blood pressure, despite the slightly underestimated values for SBP and overestimated values for DBP compared to the figures obtained with invasive measurements. Important advantages of the method are higher resistance to heart rhythm disturbances and hand movements during measurement. However, the method also has a number of significant disadvantages associated with high sensitivity to noise in the room, interference that occurs when the cuff rubs against clothing, as well as the need for precise placement of the microphone over the artery. The accuracy of blood pressure registration is significantly reduced with low tone intensity, the presence of an “auscultatory gap” or an “endless tone”. Difficulties arise when teaching a patient to listen to tones and hearing loss in patients. The error in measuring blood pressure using this method consists of the error of the method itself, the pressure gauge and the accuracy of determining the moment of reading the indicators, amounting to 7–14 mm Hg.
Oscillometric
the method for determining blood pressure, proposed by E. Marey back in 1876, is based on determining pulse changes in the volume of the limb. For a long time it was not widely used due to technical complexity. Only in 1976, the OMRON Corporation (Japan) invented the first bedside blood pressure meter, which worked using a modified oscillometric method. According to this technique, the pressure in the occlusion cuff is reduced in steps (the speed and amount of bleeding is determined by the device algorithm) and at each step the amplitude of pressure micropulsations in the cuff, which occurs when arterial pulsations are transmitted to it, is analyzed. The sharpest increase in pulsation amplitude corresponds to systolic blood pressure, the maximum pulsations corresponds to average pressure, and the sharp weakening of pulsations corresponds to diastolic blood pressure. Currently, the oscillometric technique is used in approximately 80% of all automatic and semi-automatic devices that measure blood pressure. Compared to the auscultatory method, the oscillometric method is more resistant to noise and movement of the cuff along the arm, allows measurements through thin clothing, as well as in the presence of a pronounced “auscultatory dip” and weak Korotkoff sounds. A positive point is the registration of blood pressure levels in the compression phase, when there are no local circulatory disorders that appear during the period of air bleeding. The oscillometric method, to a lesser extent than the auscultatory method, depends on the elasticity of the vascular wall, which reduces the frequency of detection of pseudo-resistant hypertension in patients with severe atherosclerotic lesions of the peripheral arteries. The technique turned out to be more reliable for 24-hour blood pressure monitoring. The use of the oscillometric principle makes it possible to assess the level of pressure not only at the level of the brachial and popliteal arteries, but also at other arteries of the extremities. This was the reason for the creation of a whole series of professional and household measuring instruments with their fixation on the shoulder, wrist (devices like Omron R series; M, meeting the requirements of the BHS protocol) and simplified the measurement of blood pressure in an outpatient setting, on the road, etc.
The use of the oscillometric method makes it possible to reduce the influence of the human factor on the pressure recording process, which allows reducing the measurement error.
Ultrasonic
The blood pressure recording method is based on recording the appearance of minimal blood flow in the artery after the pressure created by the cuff becomes lower than the blood pressure at the site of compression of the vessel. Using Doppler ultrasound, only the systolic level of regional blood pressure is determined.
Types of devices that measure blood pressure
Currently, pressure gauges must comply with AAMI/ANSI and/or BHS protocols, which require comparison of the mercury sphygmomanometer data by two examiners with the instrument being tested. According to the protocol of the American Association for the Implementation of Medical Devices, the average difference in absolute values of blood pressure recorded by experts and the device being tested should not exceed 5 mm Hg. The British Hypertension Society protocol evaluates the percentage of agreements and differences in blood pressure measured by the device and by experts, and allows the use of devices with accuracy classes A, B or C. The types of measuring devices and their main advantages and disadvantages are presented in Tables 1 and 2.
There are manual, semi-automatic and automatic types of devices that measure blood pressure.
In semi-automatic devices,
the cuff is inflated by pumping air with a rubber bulb, and the speed of air release from the cuff is adjusted automatically. Semi-automatic devices are compact, low in price and have a long battery life.
Automatic devices
characterized by the presence of a built-in compressor that ensures automatic inflation of the cuff; electronic air release valve, which allows you to maintain the rate of air deflation from the cuff during measurement and release air from the cuff after the end of the measurement. They are distinguished by high reliability and accuracy of readings. They are equipped with batteries; an AC adapter can also be purchased at the patient’s request.
Omron Corporation, professionally engaged in the development and implementation of oscillometric devices, has in its assortment automatic blood pressure meters with the Intellisense function, as well as models of devices that measure pressure in the compression phase, which is the latest, exclusive development of the corporation. Intellisense is an advanced technology from Omron that provides the user with the following benefits:
- determining the compression level taking into account the systolic pressure of each patient, which makes the measurement process more comfortable, as well as reduces the measurement time, preventing prolonged excess pressure on the underlying tissues;
- the rate of air bleeding is automatically changed, while the heart rate is analyzed, which reduces the likelihood of errors when measuring blood pressure in patients with severe heart rhythm disturbances (frequent extrasystole, tachyarrhythmias). Also, recently it has been possible to reduce the error during blood pressure measurement in case of cardiac arrhythmias through the use of improved methods for analyzing oscillograms;
- devices with this function allow you to use 3 types of cuffs (children's, standard, adult), automatically determining the bleeding speed depending on the connected cuff;
- Thanks to the Intellisense function, energy consumption is reduced, which increases battery life.
Omron's many years of clinical research have contributed to the creation of a unique blood pressure measurement algorithm. This algorithm allows you to measure blood pressure with equal accuracy in both young and elderly people, as well as in those who have diseases of the cardiovascular system.
Omron instruments undergo clinical evaluation in accordance with the strict professional requirements of the AAMI and BHS protocols to confirm measurement accuracy and algorithm performance. Clinical trials are conducted at reputable clinics in Europe, the USA, and Japan. The World Hypertension League (WHL) recommends regularly measuring blood pressure with clinically proven devices.
The advantages of automatic devices are high accuracy, ease of use, reliability, maximum comfort, and speed of blood pressure determination. Unlike semi-automatic and mechanical models, the absence of physical effort when pumping air with a pear allows you to increase the accuracy of the obtained values. The ability to record the exact date and time of blood pressure measurement, heart rate, indication of errors made during measurement, as well as the possibility of combining the oscillometric measurement method with auscultation (Omron 907) has become practically valuable. Storing from 14 to 350 measurements in the device’s memory, the ability to print out or transfer the obtained data to a computer led to the creation of a method of 24-hour blood pressure monitoring and the emergence of household blood pressure meters, which have found their application in the developing direction of medical science - telemedicine.
The disadvantages of automatic devices include the relatively high cost of the device and the need to replace batteries.
24-hour blood pressure monitoring
A single measurement of blood pressure with a sphygmomanometer, most often used in everyday clinical practice, does not always accurately reflect the value of blood pressure and does not give an idea of its daily dynamics, which complicates both the diagnosis of arterial hypertension and the assessment of the effectiveness of selected therapy. In this regard, it seems advisable to use multiple automatic measurements (monitoring) of blood pressure during the day, which allows obtaining information about the level and fluctuations of blood pressure, identifying patients with nocturnal hypertension and abnormal blood pressure variability, and assessing the adequacy of blood pressure reduction while taking antihypertensive drugs.
According to the recommendations of WHO and the International Society of Arterial Hypertension (1999), indications for 24-hour blood pressure monitoring (ABPM) are:
– clarification of the diagnosis of arterial hypertension in patients with unusual fluctuations in blood pressure during one or more visits;
– symptoms that suggest the presence of episodes of hypotension;
– identification of the “white coat” reaction in patients with a high risk of cardiovascular diseases;
– suspicion of symptomatic arterial hypertension;
– monitoring the effectiveness of antihypertensive therapy;
– arterial hypertension, resistant to therapy according to traditional blood pressure measurements.
For the first time, invasive (direct) 24-hour blood pressure monitoring was used in the mid-60s by D. Shaw et al. However, this technique has not been widely used in clinical practice due to the impossibility of its use in an outpatient setting, the risk of complications and technical complexity. In the early 70s, devices for non-invasive 24-hour blood pressure monitoring appeared. Their work is based on auscultatory or oscillographic methods of measuring blood pressure. Both methods of determining blood pressure give a large error in the presence of cardiac arrhythmias (primarily atrial fibrillation), so the most promising is the use of blood pressure monitoring systems that combine both oscillometric and auscultatory methods.
When analyzing the daily blood pressure profile obtained from monitoring, four main groups of indicators are used.
Towards averages
These include the average values of systolic and diastolic blood pressure per day, as well as separately for daytime and nighttime.
To quantify the amount of “pressure load”, time index indicators
(percentage of measurements with elevated blood pressure) and
area index
(the area of the figure bounded by the elevated blood pressure curve and the normal blood pressure line).
Indicators of circadian blood pressure rhythm
assessed by the degree of nocturnal decrease in blood pressure or by the daily index.
Short-term arterial blood pressure variability
determined by the value of the standard deviation from the average value, calculated automatically.
Additionally, such 24-hour monitoring indicators as morning blood pressure dynamics and the hypotension time index can be assessed.
Currently, the market is saturated with various modifications of tonometers from domestic and imported companies, which makes it difficult for a patient or a medical worker to choose. The experience gained first by our employees, and then by patients, in the use of semi- and automatic blood pressure meters from Omron allows us to recommend tonometers from this company for use in clinical practice and self-monitoring of blood pressure levels.
For self-monitoring, it is preferable to use the following devices: with a shoulder cuff Omron M4–I, universal cuff (22–42 cm) – Omron 773; with the ability to connect to a computer – Omron–705–IT; with wrist cuff – Omron R5–I, Omron–637–IT.
In conclusion, it should be noted that the requirements for any measuring equipment are generally universal.
These are measurement accuracy, reproducibility, simplicity and ease of maintenance, a convenient form of recording the obtained data, an optimal price-quality ratio, and environmental safety. As for devices that measure blood pressure, in the future it is planned to abandon the use of mercury tonometers, increase the percentage of use of automatic devices operating on the “press of one button” principle, and, of course, develop new methods for monitoring blood pressure. Literature:
1. Almazov V.A., Shlyakhto E.V. Cardiology for general practitioner // St. Petersburg; v.1; 127
2. Aronov D.M., Lupanov V.V. “Functional tests in cardiology” // M.; 2002; 296
3. Arterial hypertension. Recommendations for the prevention, diagnosis and treatment of arterial hypertension VNOK // 2001; 22
4. Arterial hypertension. WHO and ITF recommendations // 1999; 18
5. Brittov A.N. Arterial hypertension. Guide to Cardiology edited by G.I. Storozhakova, A.A. Gorbachenkova, Yu.M. Pozdnyakova // M.; vol.2, 286–346
6. Glezer G.A., Glezer M.G. Arterial hypertension // M.; 1996; 216
7. Gogin E.E. Hypertension // M., 1997; 400
8. Kabalava Zh.D., Kotovskaya Yu.V. Blood pressure monitoring: methodological aspects or clinical significance // M.; 1999; 234
9. Marini J.J., Wheeler A.P. Medicine of critical conditions // M.; Medicine; 2002; 992
10. Moiseev V.S., Sumarokov A.V. Heart diseases. Guide for doctors // M.; 2001; 463
11. Oganov R.G. Preventive cardiology: from hypotheses to practice // Cardiology; 1999; 39(2); 4–9
12. Oganov R.G. Epidemiology of arterial hypertension in Russia and possibilities of prevention // Ter. archive, 1997; vol.97, no.8; 66–69
13. Prevention, diagnosis and treatment of primary arterial hypertension in the Russian Federation (DAH-1) // Clinical pharmacology and therapy; 2000; 9(3); 1–24
14. Alderman MH, Cohen H., Madhava S. Distribution and determinants of cardiovascular events during 20 years of successful antihypertensive treatment // J. Hypertens., 1998; 16:761–769
15. Alison TG, Cordeiro MA, Miller TG et al. Prognostic significance of exercise–induced systemic hypertension in healthy subjects // Am.J.Cardiol. – 1999 – Vol.83 – P.371–375
16. Gifford RW An Algorithm for the Management of Resistant Hypertension // Hypertension – 1998, Vol.11, No. 3, Suppl.II, p.101–105
17. Joint National Committee on Detection Evaluation and Treatment of High Blood Pressure. The sixth report of the Joint National Committee on Prevention, Detection and Treatment of High Blood Pressure (JNC VI) // Arch.Intern.Med., 1997, 157, p.2413–2446
18. Konnel WB Fifthy years of Framingbam Study contributions to understanding hypertension // J.Hum.Hypertens., 2000, 14, 83–90
19. Spyckerelle Y., Deschamps J.–P. Le “risque” cardio-vascular chez l'enfant et l'edolescent // Coeur, 1984, 15, 6, p.715–737
20. Stamler J., Stamler R. Intervention for the Prevention and Control of Hypertension and Atherosclerotic: United States and International Experience // Amer.J.Med., 1984, 76, 2A, p.13–36
The official representative of Omron Healthcare Europe BV in Russia is KomplektServis CJSC
127006, Moscow, Vorotnikovsky lane 7., building 3
tel/fax: (095) 299–40–64, 209–37–31.
www.omron–med.ru