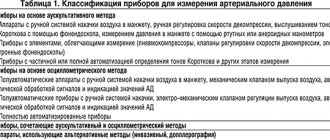
Home Articles How to measure blood pressure correctly
Adapting medical technologies to the needs of patients makes it possible to monitor blood pressure (BP) values independently. To do this, you need to buy a mechanical or electronic tonometer at the pharmacy. Knowing how to correctly measure blood pressure, you can assess your condition or provide assistance to a loved one. Regular monitoring of blood pressure is necessary for patients with cardiovascular pathologies, diabetics, elderly people, and bedridden patients.
Features of measuring blood pressure in children.
Before measuring blood pressure in children, be sure to consult a pediatrician!
During an individual consultation, the pediatrician will provide detailed information on the general rules of measurement, and will also determine the required measurement time, the level of air injection into the cuff and the acceptable intervals of blood pressure values for your child. Blood pressure standards for children have been developed for doctors, in accordance with their age, weight, height, and gender.
According to the recommendations of leading European pediatricians, it is necessary to periodically measure blood pressure in children over three years of age or even earlier, especially if there are any risk factors.
Your child’s blood pressure readings are very dependent on his mood, nutrition, physiological characteristics and may go beyond normal limits, which should not cause much panic. But if lethargy, drowsiness, refusal to eat, complaints of headache, nausea, etc. are added to pressure disorders, then you must immediately contact a pediatrician who will conduct additional research and, if necessary, prescribe adequate and effective treatment.
It is preferable to measure a child’s blood pressure in the first half of the day, an hour after a hearty lunch, active physical exercise, games or school activities.
To measure blood pressure in children in medical institutions, aneroid tonometers are used (auscultatory measurement method). At home, it is preferable to use automatic and semi-automatic tonometers, which are based on the oscillometric measurement method with a special children's cuff with an internal chamber size of 9x16 cm (corresponding to size S). As a rule, a special table of cuff sizes is attached to the tonometer passport. If high blood pressure is detected by an electronic device, control is carried out in a medical institution with an aneroid blood pressure meter.
The procedure for measuring blood pressure should be repeated three times with an interval of three minutes, since a single measurement is not enough to assess the real picture.
Blood pressure in newborns is measured using oscillographic and ultrasound methods, which make it possible to determine pressure indicators, regardless of the baby’s mobility and restlessness.
Pressure Diary
For people suffering from arterial hypertension, the doctor advises keeping a blood pressure diary. “This is not done to somehow burden the patient, but to evaluate the effectiveness of treatment. If the indicators, for example, during treatment are kept at 110-130, and the lower bar is within 60-80 mm Hg. Art., which means the therapy is working,” says the specialist.
If the pressure reaches 140 and 90 mm Hg. Art. or stays at 130 and 80 mm Hg for a long time. Art., and there are also risk factors such as bad habits, night shifts at work, frequent episodes of high blood pressure (> 150-170/90-100), obesity, heart pain, shortness of breath, etc., you should visit a doctor . “Self-medication in such a situation is unacceptable, because arterial hypertension is the best-known, most common disease, with proper treatment of which a person can live a long time and feel comfortable,” sums up Azizkhon Askarov.
Measuring blood pressure in older people.
In an elderly person, it is more difficult to achieve complete and lasting normalization of blood pressure.
There may be several reasons. With age, the severity of arterial hypertension and the number of concomitant diseases increase; it is more difficult to persuade an elderly person to undergo treatment regularly, especially with decades of experience of high blood pressure. In older people, instability of blood pressure is more common. This is influenced by a decrease in the elasticity of the walls of blood vessels and atherosclerosis due to aging, as well as disturbances in the functioning of blood flow regulation systems. When measuring blood pressure in the elderly, it is especially important to take several consecutive measurements (at least 3) and record their average value. This procedure is greatly simplified by electronic blood pressure meters with MAM technology (Microlife Average Measurement), which perform sequential triple measurements with calculation of an optimized result.
In the elderly, episodes of a sudden drop in blood pressure are common - postural hypotension (a sharp drop in pressure during the transition from the “lying” state to the “sitting” or “standing” state). It is recommended that arterial blood measurements be taken both while sitting and standing, especially in the presence of hypotension or during antihypertensive therapy. In persons over 65 years of age, with concomitant diabetes mellitus and antihypertensive therapy, blood pressure should also be measured after 2 minutes of standing.
About pressure
Blood pressure indicators are a digital assessment of the force with which circulating blood presses on the inner wall of the vessel. The upper value is recorded at the moment of systole (contraction of the heart muscle), the lower value at the moment of diastole (relaxation of the myocardium). The systolic indicator reflects the strength of muscle tension at the moment of blood ejection, the diastolic indicator reflects the tone of the blood vessels. A decrease, and more often an increase in blood pressure, occurs:
- due to physical and nervous overload;
- against the background of chronic diseases;
- due to age-related changes in the body.
In a healthy person, a compensatory mechanism can cope with the “jump” in blood pressure in half an hour. People with heart and vascular diseases require medication assistance, so they need to measure their blood pressure twice a day. Elderly relatives living separately should be taught self-control skills. If a person cannot use a blood pressure monitor for health reasons, a specially trained caregiver can be hired.
Measuring blood pressure in people with arrhythmia.
Arrhythmia is a violation of the frequency, rhythm and sequence of contractions of the heart. In people with arrhythmias, systolic pressure can vary significantly from beat to beat.
To assess the level of blood pressure in such a situation and obtain a reliable result, it is necessary to perform several consecutive measurements (at least 3), and then calculate the average value of the measurements. Modern devices with MAM (Microlife Average Measurement) technology allow you to do this by pressing only one button. When using mechanical blood pressure monitors, deflate the cuff more slowly.
Today, there are electronic blood pressure meters with PAD (Pulse Arrhythmia Detection) technology, which makes it possible to obtain an accurate result in individuals with pulse arrhythmia.
St. Petersburg State Budgetary Healthcare Institution "Polyclinic No. 98"
Blood pressure level is one of the clearest indicators of health status. True, most often the need to monitor blood pressure is remembered in diseases of the cardiovascular system. In fact, everyone should know everything about their blood pressure, because it changes for various reasons.
What is blood pressure?
Blood pressure (BP) is the pressure that blood exerts on the walls of the arteries. It is uneven and fluctuates depending on the phase of the heart. During systole, when the heart contracts and releases another portion of blood into the vessels, the pressure increases. And in diastole, when the heart relaxes and fills with blood, the pressure in the arteries decreases. The blood pressure on the walls of the arteries in systole is called “upper” or systolic, and in diastole – “lower” or diastolic. It is customary to write the blood pressure value using a fraction: the first is the upper, the second is the lower.
Blood pressure is one of the most important indicators of the cardiovascular system. In most healthy people it is relatively constant. But under the influence of stress, physical activity, overwork, drinking large amounts of liquid and under the influence of other factors, its value may change. Typically, such changes are either not too frequent or not too strong, and do not exceed 20 mm during the day. rt. Art. – for systolic, 10 mm. rt. Art. – for diastolic. But, a repeated or persistent decrease or increase in pressure beyond the normal range may be an alarming signal of illness and requires immediate consultation with a doctor.
Blood pressure standards according to WHO classification
| Blood pressure (category) | Upper blood pressure (mm Hg) | Lower blood pressure (mm Hg) |
| Hypotension (low) | below 100 | below 60 |
| Optimal pressure | 100–119 | 60–79 |
| Normal pressure | 120–129 | 80–84 |
| High normal pressure | 130–139 | 85–89 |
| Moderate hypertension (increased) | 140–159 | 90–99 |
| Moderate hypertension | 160–179 | 100–109 |
| Severe hypertension | more than 180 | more than 110 |
The ideal “cosmonaut pressure” is 120/80 mm. rt. Art. However, many doctors agree that everyone has their own ideal, and therefore often ask about the patient’s “working” pressure. Working blood pressure is the usual constant blood pressure interval that provides a person with good health. Since this interval is individual, for someone 115/80 with a working 130/90 may be lower, although it falls within the normal range. And, conversely, with a working level of 110/80, 130/90 may become elevated. Knowing the working pressure helps the doctor to timely identify pathology, make a more accurate diagnosis and choose the right treatment.
However, it is worth remembering that pressure beyond the lower and upper limits of the norm is not working for a healthy person. And feeling normal in this case is only an additional reason to seek advice from a specialist.
Who needs to monitor blood pressure levels and how?
One of the most common disorders of blood pressure regulation is hypertension. Often behind it lies hypertension, leading to myocardial infarction, stroke and other serious complications. Unfortunately, arterial hypertension is often asymptomatic, so everyone needs to monitor their blood pressure. People who are prone to increasing it, who are exposed to risk factors for developing hypertension and experiencing its symptoms should be especially careful and measure blood pressure from time to time. For the rest, annual monitoring during the medical examination period is quite sufficient. But for those who have been diagnosed with arterial hypertension, it would be good to make friends with a tonometer and check the pressure level at least twice a day - in the morning and in the evening.
It is imperative to measure blood pressure if you experience weakness, dizziness, headache, darkening, “veil” in the eyes, tinnitus, difficulty breathing, pain and heaviness in the heart area or behind the sternum, or when other symptoms appear that usually accompany an increase or decrease in pressure.
It is also worth monitoring blood pressure during exercise, especially when selecting a load.
How to measure blood pressure correctly?
If the blood pressure measurement is planned, then one hour before the measurement you should not drink alcohol, drinks containing caffeine (tea, cola, coffee) or smoke, and five minutes before the measurement, ensure yourself a state of rest.
At the first visit to the doctor, the pressure is measured on both arms alternately. If the results differ by more than 10 mm. rt. Art., then the subsequent measurement is carried out on the arm with a high blood pressure value. However, normally the readings are approximately the same. The difference between them exceeds 10 mm. rt. Art., indicates an increased risk of diseases of the cardiovascular system and death from them or an existing pathology.
Blood pressure is usually measured while sitting or lying down. The hand on which the measurement is taken should be freed from clothing and compressive objects, relaxed and motionless. To avoid unwanted tension, it can be placed on an object that provides a support point, such as a table or the edge of a bed. It is best to position the limb so that the elbow is at the level of the heart. The arm should not have arteriovenous fistulas for dialysis, traces of a section of the brachial artery, or lymphedema.
The cuff is placed on the shoulder 2 cm above the elbow. It is important that it fits your hand tightly, but does not squeeze it.
Ideally, blood pressure is measured twice with an interval of 2 minutes. If the result differs by more than 5 mm. rt. Art. – after 2 minutes, take the third measurement and calculate the average value.
The method of measuring pressure depends on the device used and is indicated in the operating instructions.
How to choose a pressure measuring device?
The device for measuring pressure is called a tonometer. There are two types of tonometers - mechanical and electronic (automatic and semi-automatic).
A mechanical tonometer is inexpensive, reliable, lasts a long time, guarantees high measurement accuracy, is easy to use, but requires certain skills and is more difficult to use without assistance.
The electronic tonometer is convenient and simple; you can easily use it yourself. In addition to devices that measure pressure on the shoulder, there are also those that measure it on the wrist. This tonometer can be carried with you, which is sometimes important for some hypertensive patients. And devices with large dials come in very handy for older people. Many of the electronic tonometers show the pulse, remember the data of the latest measurements and are equipped with some other functions, the quantity and quality of which largely depends on the price of the device. But automatic and semi-automatic devices are more expensive than mechanical ones, less accurate and may last slightly less. In addition, in some diseases, blood pressure is very difficult to measure with an electronic tonometer, for example, with atrial fibrillation.
When purchasing a tonometer, you must pay attention to the presence of instructions in Russian, a passport of the device, a warranty card and the absence of visible defects. And when purchasing an electronic device, it also depends on the country of origin. Japanese and German devices are traditionally considered the best.
If the choice falls on a mechanical tonometer, it is worth remembering that it requires a phonendoscope. It is often not included in the package.
It is best to buy pressure measuring devices at a pharmacy or specialty store. If the device is purchased secondhand, the accuracy of the measurement and its service life cannot be guaranteed.
The average width of the cuff should be 13–17 cm, for children - a little less, for overweight people - a little more.
Before use, the tonometer should be checked and, if necessary, adjusted. It is easier and more correct to do this with the help of a doctor.
How to measure blood pressure with a mechanical tonometer?
Not everyone can measure pressure independently with a mechanical tonometer, so the help of another person is advisable.
In addition to a tonometer, you will need a phonendoscope for measurements.
A phonendoscope is a device for listening to sounds accompanying the work of internal organs. It consists of a “head” that is applied to the body, tubes that conduct sound, and tips that are inserted into the ears.
Measurement procedure:
- A cuff is placed on the shoulder, 2 cm above the elbow.
- The pulse is determined at the radial artery at the wrist.
- Air is quickly inflated into the cuff. After the pulse disappears, the cuff is inflated by another 30–40 mm Hg. Art.
- The head of a phonendoscope is placed along the lower edge of the cuff in the elbow bend, slightly inward from the center of the ulnar fossa.
- The air from the cuff is slowly released at a speed of 2-3 mmHg. Art. in 1 s. In this case, the instrument scale is constantly under control. The scale value at which the first sound appears is considered the systolic pressure value, and the value at which it disappears is considered the diastolic pressure value.
- When the pulse wave beats become inaudible, the air from the cuff is quickly released.
Measuring blood pressure with an electronic tonometer for a specific device may have its own subtleties and is described in detail in the operating instructions.
Measuring blood pressure in people with a large upper arm circumference.
The measurement cuff must be selected according to the ruler supplied with the tonometer.
In persons with a large upper arm circumference (obesity, well-developed muscles) or those with a conical-shaped arm, it is difficult to position the cuff correctly, which makes it much more difficult to accurately measure blood pressure. In this case, you need to choose a larger cuff of 32-42 cm with an inner chamber of 15x30 cm (corresponding to size L) or a universal cuff of 22-42 cm.
Blood pressure monitors with a wrist cuff can be used, but the possible difference in pressure between the shoulder and the wrist should be taken into account (with age or disease, the elasticity of the wrist vessels decreases faster than the brachial vessels, which leads to lower blood pressure readings at the wrist).
How to measure pressure correctly?
There are certain rules for measuring pressure. “Blood pressure is measured either at home or at a doctor’s appointment by placing a blood pressure cuff on your right or left arm. When taking the first measurement, it is worth taking it on both arms,” says the cardiologist.
It is worth taking an average measurement. “To do this, we measure the pressure on both hands and the third - a control one. Then we take the average. For example, a person has 125 on his right hand, and 120 on his left, the top bar, but with the third measurement it turns out to be 123-125, then we take the larger number as the average. This will allow you to find out what the maximum pressure is for a person and focus on it,” advises the cardiologist.
“Different pressure readings on the arms indicate differences in blood flow. And in the future it will be necessary to measure the pressure on the arm where the indicator is higher,” says Azizkhon Askarov.
The best way to measure blood pressure is on the shoulder. Today there are devices that measure on the wrist, but they are not considered as informative as measurements in the shoulder area, emphasizes Azizkhon Askarov. The cuff must be applied in a certain way: it is located at the level of the elbow at a distance of two fingers, or 3-4 cm. At this distance, the lower edge of the cuff must be tightly applied so that one finger fits under it, says the cardiologist. The shoulder should be at the level of the heart in order to obtain more accurate measurement results.
There are other conditions for qualitative measurement. So, measurements should be taken after 15-20, or preferably 30 minutes of rest, for example, if a person came to the clinic or returned home from work. “Also, a person should not drink caffeine-containing drinks (tea, coffee) 30-40 minutes before measuring. It is advisable not to smoke for 40 minutes before measurement. In addition, you should wear loose clothing,” advises cardiologist Askarov.
In addition, the person should not experience discomfort before the measurement. For example, if he has a full bladder or a sore throat, you first need to eliminate the source of discomfort, and only then measure the pressure. The environment should be calm and relaxed. It is advisable for a person to sit on a chair with a back or on an armchair, leaning comfortably.
“It is better, of course, to measure with an automatic or semi-automatic device. Not all patients know how to use a mechanical tonometer,” says Azizkhon Askarov.
Before or after a meal is not so important. But at the same time, if you want to measure the pressure afterwards, you should wait half an hour. In general, as the specialist notes, it is better to measure blood pressure in the morning within 5 minutes after waking up and in the evening - 20-30 minutes before bedtime.
Blood pressure is under control. Why is it important to prevent hypertension Read more
Measuring blood pressure in pregnant women.
Blood pressure in pregnant women is one of the important indicators on which general and uterine blood circulation and the successful course of pregnancy depend.
The presence of arterial hypertension before pregnancy or that develops during pregnancy can often interfere with successful delivery. In order to minimize the likelihood of serious complications in the mother and child by normalizing blood pressure, there are modern control methods, including mandatory and repeated blood pressure measurements during pregnancy and training pregnant women in self-control skills.
Blood pressure in pregnant women should be measured in a reclining position. The “white coat effect” is observed in 30% of pregnant women. To avoid unnecessary treatment, you need to regularly monitor your blood pressure at home!
Attacks of suffocation
Allergy
52825 November 19
IMPORTANT!
The information in this section cannot be used for self-diagnosis and self-treatment.
In case of pain or other exacerbation of the disease, diagnostic tests should be prescribed only by the attending physician. To make a diagnosis and properly prescribe treatment, you should contact your doctor. Attacks of suffocation: causes of occurrence, under what diseases they occur, diagnosis and treatment methods.
Definition
Choking, or asphyxia, is a painful, life-threatening, pathological condition that is characterized by a lack of oxygen and the accumulation of carbon dioxide in the tissues.
Choking is an extreme degree of shortness of breath when a person feels a sudden lack of air, increased heart rate and fear.
Choking is a symptom of serious diseases and conditions, which are characterized by impaired airway patency, and is observed in certain pathologies of the cardiovascular, musculoskeletal and nervous systems.
Varieties of suffocation
According to the mechanism of occurrence and development, the following types of asphyxia are distinguished:
- mechanical asphyxia
is suffocation that occurs as a result of restriction or cessation of air flow into the airways when they are narrowed (for example, due to swelling of the subglottic space with the development of false croup in children), obstruction (or otherwise blockage) of the airways and their compression (for example, for tumors). - traumatic asphyxia
is suffocation that occurs due to severe compression of the chest. Often occurs during traffic accidents. - toxic asphyxia
is suffocation that develops as a result of depression of the respiratory center, paralysis of the respiratory muscles (diaphragm) or when the transport function of the blood is impaired (carbon monoxide poisoning).
Possible causes of suffocation
With the development of bronchial obstruction (a decrease in the diameter of the small bronchi due to spasm or swelling), the attack develops suddenly and may be accompanied by precursors: a feeling of pressure behind the sternum, anxiety, and itching.
Attacks of bronchial asthma often occur after contact with an allergen, during acute respiratory diseases.
Choking gradually increases, and it becomes difficult for a person to breathe, the breathing frequency increases, and exhalation lengthens. The condition is somewhat facilitated by taking a specific position: sitting or standing, resting your hands on a table, bed or windowsill. This way breathing is restored due to the involvement of auxiliary respiratory muscles. An attack of suffocation may be accompanied by pronounced wheezing, which can be heard at a distance, cyanosis (the skin color takes on a bluish tint) and swelling of the veins. The duration of the attack can vary from several minutes to several hours. At the end of the attack, a cough appears, followed by the discharge of colorless sputum.
Choking may be a manifestation of developing pulmonary edema in diseases of the cardiovascular system. Stagnation occurs in the circulatory system of the lungs due to a decrease in the pumping function of the heart, so the lung tissue becomes saturated with the liquid part of the blood. The accumulated liquid enters the respiratory tract, obstructs the movement of air, causing suffocation, and comes out in the form of pink foam.
Pulmonary edema is often a consequence of myocardial infarction.
The cause of suffocation in children is often the entry of a foreign body into the upper respiratory tract. This happens due to inattention and haste when eating, laughing, coughing and sneezing while eating. Children left unattended may swallow small toys or parts of them. In adults, foreign bodies often enter the respiratory tract during alcohol intoxication. For older people, dentures pose a danger.
Choking in children can be a consequence of the development of false croup. Due to inflammation of the mucous membrane, the larynx swells and the lumen of the airways narrows significantly. Associated symptoms are a barking cough, hoarseness, a rough voice, a slight rise in body temperature and the participation of accessory muscles in the breathing process.
With a thermal or chemical burn of the respiratory tract, a reflex spasm (narrowing) of the bronchi occurs, as a result of which a person cannot take a full breath.
Diseases that may cause asthma attacks
The main group of diseases that cause asthma attacks are diseases of the respiratory system:
- bronchial asthma,
- chronic obstructive pulmonary disease (COPD),
- pneumothorax (air entering the pleural cavity, causing the lung to compress),
- tumors of the mediastinal organs and respiratory tract (larynx, trachea, bronchi),
- acute stenosing laryngotracheitis, or false croup (typical of preschool children),
- epiglottitis (inflammatory disease of the epiglottis),
- lung cancer.
Other causes of suffocation include the following:
- pulmonary embolism (blockage by thrombotic masses of the vessel through which blood enters the lungs. Blood clots most often form in the veins of the lower extremities, and when they break off, they enter the pulmonary artery);
- pulmonary edema;
- traumatic brain injury;
- Quincke's edema (allergic reaction);
- burns of the upper respiratory tract;
- epilepsy;
- overdose of certain medications and drugs;
- panic attacks.
Which doctors should you contact if you have an attack of suffocation?
First of all, in the event of an attack of suffocation, you need to call an ambulance.
The selection of primary treatment to prevent further episodes of suffocation and shortness of breath is carried out by or. Depending on the accompanying symptoms, consultation with specialized specialists, for example, a pulmonologist, an endoscopist, an allergist, a toxicologist, may be required.
Diagnostics and examinations for asthma attacks
Depending on the accompanying symptoms, the following examinations may be prescribed:
- clinical blood test;
The problem of modern pathogenetic intensive therapy for intracranial hemorrhages of non-traumatic origin is the most important in clinical neuroreanimatology, which is associated with a high prevalence, mortality rate, disability and social maladaptation of patients who have suffered hemorrhagic stroke [1-3].
Changing the position of the angle of inclination of the head end of the bed in neurosurgical patients is a generally accepted and proven method for correcting increased intracranial pressure (ICP) [2, 4, 5]. In intensive care practice, positions from 15 to 60° are used, but preference is given to 30° [2, 5, 6]. To date, there is no consensus on which position most effectively and significantly reduces ICP without reducing cerebral blood flow. It is generally accepted that for most patients with cerebral pathology, regardless of the etiological factor, a position of 15-30° is preferable. Early work carried out on patients with various brain pathologies confirmed the effective reduction of ICP at various positions of the head end in the range from 15 to 60° [5-7]. This position is justified from a physiological point of view, since even a slight elevation of the head end of the bed improves venous and liquor outflow from the cranial cavity and leads to a decrease in ICP [4, 5, 8]. However, the choice of the position of the angle of inclination of the head end in case of intracranial hemorrhage after surgery remains a controversial issue [6].
The purpose of the study was to study the nature of the relationship between hemodynamic parameters (ICP, cerebral perfusion pressure (CPP), mean arterial pressure (MAP) at different positions of the head end of the bed in patients with intracranial hemorrhage.
Material and methods
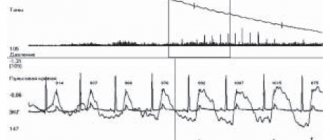
The study included 36 patients (11 men and 25 women) with intracranial hemorrhages of non-traumatic origin aged from 16 to 65 years (average - 52.9±10.5 years). Upon admission and over time, all patients underwent multislice computed tomography (MSCT) of the brain. Of these, 27 were diagnosed with subarachnoid hemorrhage using MSCT angiography due to rupture of an arterial aneurysm of cerebral vessels, and 8 were diagnosed with hemorrhagic stroke with the formation of an intracerebral hematoma of hemispheric localization. All patients were operated on on the 1st day from the onset of the disease. Treatment of patients was carried out taking into account the indicators of multimodal neurophysiological monitoring of ICP, blood pressure, CPP, cerebral blood flow (CBF) using transcranial Dopplerography (TCDG). ICP was measured using parenchymal sensors (Codman Microsensor “Johnson & Johnson”, USA). The sensor was installed on the opposite side of the lesion (on the intact side). The parameters of ICP, BP, and CPP were recorded using Philips MP 40 and MP 60 bedside monitors. Data were collected through an analog output on a personal computer and analyzed using the ICM Plus program. Radial artery catheterization was performed to measure invasive blood pressure. The invasive blood pressure sensor was placed at the level of the external auditory canal (in the projection of the foramen of Monroe) in order to correctly measure CPP. Doppler examination was performed according to standard methods using the Sono Scape S8 apparatus. When conducting a test with a change in the position of the head end of the bed, three consecutive measurements were taken, each lasting 5 minutes in positions 30-0-60°; in all cases, the initial ICP did not exceed 25 mm Hg. The study began in the standard position of the patient, when the angle of inclination was 30°. Subsequently, following the research algorithm, the patient was given a horizontal position with subsequent elevation of the head end to 60°. After stabilization of the condition at each point, the parameters of average ICP, blood pressure, and central pressure were recorded for 5 minutes. The study was carried out on days 1, 2, 3 and 5 after surgery. The criterion for inclusion in the study was survival of the operated patients for at least 1 week from the onset of the disease.
Statistical processing of the obtained data was carried out using the Statistica 6.0 software package in accordance with the main objectives of the study. The normality of the distribution of variables was checked using the Shapiro-Wilks method. Parametric and nonparametric statistical methods were used for analysis. Data are presented as medians and quartiles.
Results and discussion
Starting from the 1st day from the onset of the disease, a gradual increase in intracranial pressure figures was observed (Table 1)
.
The recorded ICP values in the standard position of the head end of the bed of 30° increased sharply and by the 3rd day of monitoring reached 27 (22-33) mm Hg, increasing by 22% compared to the initial parameters.
The greatest differences in ICP threshold values were recorded on the 5th day after surgery - on average 27% compared to the 1st day (from 21.5 (19-24) to 27 (20.5-36) mm Hg by the 5th day). At the same time, according to invasive monitoring data, the average ICP numbers from the 1st to the 5th day increased insignificantly. A sharp decrease in CPP was observed already on the 2nd day from the onset of the disease. Its values decreased by 18% compared to the initial ones - from 89.5 (84-101) to 73.5 (63.5-84) mm Hg. Further, the CPP indicators gradually increased, but by the 5th day they did not reach the initial level, equaling 83 (69.5-88.5) mm Hg, and on average became 7% lower than on the 1st day.
Also on the 2nd day there was a decrease in mean arterial pressure: from 105 (97-120.5) to 91 (81.5-100) mmHg, which was on average 13% lower than the initial values. Subsequently, the blood pressure readings began to gradually increase, but never reached the initial level, amounting to 97.5 (89.5-105) mm Hg. on the 5th day. Thus, the difference in the recorded blood pressure values between days 1 and 5 was 7%.
When performing a sequential change in the angle of inclination of the head end of the bed (30-0-60°) on the 1st day, the maximum ICP values (18 (16-22) mm Hg) were recorded in a horizontal position (Table 2)
.
ICP figures in the horizontal position were 33% higher than at 30 and 60°.
There were no significant differences between the 30 and 60° positions, and the average ICP values were 12 mmHg. The minimum CPP values on the 1st day from the onset of the disease were recorded in the 30° position, but did not differ significantly from the CPP figures in the horizontal position - 86 (78-99) and 87 (79.5-99.5) mm Hg . respectively. At the 60° position, the CPP was on average 5.5% higher than at 30° - 91 (81.5-99) mm Hg.
It was also noted that in a horizontal position in patients with non-traumatic hemorrhages, blood pressure increases by 5%, approaching 103.5 (98-117.5) mm Hg. At the same time, at the 30 and 60° positions the differences were insignificant: 98 (90.5-111) and 101 (94.5-113.5) mmHg. respectively. Thus, on the 1st day from the onset of the disease, the position of the head end of the bed 0° was the least preferable, since in this case a pronounced increase in ICP values was observed in combination with minimal perfusion of the brain parenchyma. The 60° position should be considered the most favorable on the 1st day after surgery, since it was in it that optimal CPP values were observed, ICP values remained relatively stable and the blood pressure level increased slightly (on average by 3% compared to the 30° position).
On the 2nd day from the onset of the disease, a similar pattern was observed: when the position of the head end of the bed changed from 30 to 0°, the maximum ICP and critically low CPP were recorded in the horizontal position: 20 (16-25) and 71.5 (60-83) mm Hg respectively. However, at the 60° position (compared to 30°), ICP was increased by an average of 3%, and CPP decreased by 5.5%. Blood pressure values were maximum in the horizontal position - 91.5 (83.5-105.5) mm Hg; When the head end of the bed was raised, the blood pressure readings remained stable. Thus, on the 2nd day from the onset of the disease, preference should have been given to an angle of inclination of the head end of the bed of 30°. It was in this position that optimal cerebral perfusion was ensured and intracranial hypertension did not increase.
On the 3rd day after surgery, there is a critical increase in ICP (an average increase of 7-14 mm Hg) in combination with low cerebral perfusion (a decrease of 5-7 mm Hg) and high systemic blood pressure ( an increase of 4-8 mm Hg) were still recorded in a horizontal position (see Table 2)
. However, by the 3rd day the difference in the values of hemodynamic parameters in the 30 and 60° positions disappeared. Therefore, both of these positions can be considered optimal.
On the 5th day, the horizontal position of the patient was again the least preferable. At the same time, the increase in ICP in the 0° position became less significant (6-8 mm Hg compared to 8-11 mm Hg on the 1st day), however, a longer period of time was required to restore ICP values to the original numbers When recording CPP, the minimum values were recorded at 60° - 77.5 (69-89.5) mm Hg. At the same time, a significant decrease in blood pressure in the 60° position was observed: from 99 (90.5-107) to 94.5 (88-102) mm Hg. Thus, changing the angle of inclination of the head end of the bed upward to 60° was just as undesirable as keeping the patient in a horizontal position. The optimal angle of inclination again became 30°.
It should be noted that an increase in the ICP level in a horizontal position leads to the formation of a Doppler pattern of difficult perfusion, characterized by a relative decrease in the average linear blood flow velocity and an increase in peripheral resistance indices. According to M. Rosner et al. [6], an elevated position of the head end can effectively reduce ICP in only 1/2 of patients with neurosurgical pathology. In our study, on the 1st day from the onset of the disease, a significant decrease in ICP figures when moving from the horizontal to the 60° position occurred in 78% of patients. However, by the 5th day, an effective decrease in intracranial pressure when changing the angle of inclination of the head end of the bed towards its increase was registered only in 62% of patients.
Despite the different etiological factors, in patients with hemorrhagic stroke with the formation of intracerebral hematomas and patients with subarachnoid hemorrhages due to rupture of cerebral arterial aneurysms, no significant differences were found in the studied parameters.
The conducted research gave grounds to formulate the following conclusions.
In patients with non-traumatic intracranial hemorrhage, the maximum increase in ICP was observed starting from the 3rd day from the onset of the disease in combination with reduced cerebral perfusion. Starting from the 2nd day after surgery, continuous monitoring of hemodynamic parameters is advisable to avoid the development of uncontrolled intracranial hypertension and ischemic brain damage.
On the 1st day from the onset of the disease, an angle of 60° should be considered optimal, since it was in this position of the head end of the bed that optimal cerebral blood flow was maintained and intracranial hypertension syndrome did not increase. On the 2nd day, the angle of 30° became the most favorable, and by the 3rd day, the differences in the values of hemodynamic parameters in the 30 and 60° positions disappeared, and both of these positions were optimal. On the 5th day after surgery, an inclination angle of 30° again became preferred.
Considering the critical increase in intracranial hypertension and a significant decrease in cerebral perfusion when the head end of the bed is positioned at 0°, regardless of the patient’s length of stay in the intensive care unit, it is necessary to ensure the short duration and maximum painlessness of invasive manipulations, which are possible only when the patient is in a horizontal position (tracheostomy, catheterization of central veins, changing the endotracheal tube, etc.).