Possible complications
The consequences of fluid accumulated in the lungs can be quite serious.
Exacerbation of chronic pulmonary edema or advanced exudative pleurisy is life-threatening. The bronchopulmonary system cannot fully function due to increasing oxygen starvation. Lack of timely medical care leads to a number of the following complications:
- Compression of the mediastinum. The mediastinum is a group of organs lying between the two pleural cavities.
- Airway obstruction due to excessive foam.
- Formation between the pleural layers of purulent contents or contents mixed with blood.
- Choking – difficult and depressed breathing.
- Worsening heart failure with rhythm disturbances and periodic hypertensive crises.
Treatment of pleurisy
Pleura is a thin film that covers the lung and the inner surface of the chest wall. The cavity between the lung and the chest wall is called the pleural cavity. Normally, it contains a small amount (3-5 ml) of fluid to reduce friction between the lung and the inner surface of the chest during breathing. This fluid is constantly secreted and simultaneously absorbed by the pleura, thereby maintaining its constant amount.
In some lung diseases (tuberculosis, inflammation, tumors), systemic connective tissue diseases, kidney, liver, and heart failure, the processes of absorption and release of fluid may be disrupted, which leads to its excessive accumulation. The volume of fluid can be up to several liters, which leads to compression of the lung and severe shortness of breath in the patient.
Symptoms
Pleurisy (pleural effusion) in most cases is only a symptom of a disease, and not an independent disease. In total, there are more than fifty diseases that can be accompanied by the accumulation of fluid in the pleural cavity. In this case, symptoms of pleurisy in the form of the appearance and increase of shortness of breath, weakness, in some cases dry cough and even fever, may appear long before the symptoms of the disease that led to the appearance of fluid in the pleural cavity. A special group of pleurisy is represented by lesions of the pleura associated with tumors. In this case, the pleura is affected by metastases, and the primary tumor can be localized in the stomach, intestines, lung, uterus, ovary, and lymph nodes.
Diagnosis of pleurisy
To detect fluid, a chest x-ray is sufficient. In some cases, when the fluid in the pleural cavity is unevenly distributed, your doctor may order an ultrasound of the pleural cavity and/or a CT scan of the chest.
The basis for diagnosing pleurisy is pleural puncture. After local anesthesia, the doctor will use a special needle to remove fluid from the pleural cavity for examination. The removal of fluid itself makes the patient feel better, reduces shortness of breath and chest pain.
The program for further examination is determined after a comprehensive examination of the fluid (biochemical analysis of pleural fluid, study of its cellular composition, tests for tuberculosis, search for tumor cells). It is especially important that the clinic has an immunocytochemical study - this is a complex cytological test that increases the reliability of the diagnosis of tumor pleurisy from 50% with conventional cytology to 97-99%.
In case of repeated accumulations of fluid and an unknown cause, the most reliable and shortest way to diagnose is a diagnostic operation - video thoracoscopy. It is performed using 2 or 3 small incisions on the chest wall under general anesthesia. Using a miniature video camera inserted into the pleural cavity, the condition of the lung and pleura is visually assessed. Then a biopsy of the pleura, altered lymph node or neoplasm is performed for histological and immunohistochemical examination.
Treatment
In case of recurrent pleurisy, thoracoscopic surgery is performed to prevent the accumulation of fluid in the pleural cavity - pleurectomy (removal of the pleura from the inner surface of the chest) and talc pleurodesis (spraying powdered talc into the pleural cavity), which leads to adhesions and fusion of the pleural cavity.
To make an appointment for a consultation and examination by phone: +7 (921) 919-07-49
What causes fluid to accumulate in the lungs during cancer?
Fluid in the lungs due to malignant neoplasms occurs for various reasons. If we are talking about pulmonary edema, then we can indicate 2 main groups of root causes: cardiogenic and non-cardiogenic. Cardiogenic (associated with cardiac dysfunction) include exacerbations of chronic heart problems, pulmonary embolism, and cardiomyopathies. Non-cardiogenic causes - septic process, congestive pneumonia, side effects of chemotherapy drugs, exposure to ionizing radiation. In oncopathology, both options occur.
Exudative pleurisy is a characteristic feature of the late stage of cancer. Most often, pleurisy occurs with neoplasms of the lungs, mammary glands, and ovaries. The effusion emerges between the layers of the pleura in the following cases:
- metastatic foci appeared in the lymph nodes located near the bronchi;
- the tumor blocks the bronchial lumen;
- Oncology provoked pneumonia.
Fluid in the lungs can accumulate after irradiation of the chest or treatment with certain chemotherapy drugs (methotrexate, cyclophosphamide).
Memo to a patient who has undergone cardiac surgery
Memo to a patient who has undergone cardiac surgery
After heart surgery, you may feel that you have been given another chance to prolong your life, and you will want to get the maximum results from the operation. If it was coronary bypass surgery, then it is important to change your lifestyle, for example, lose extra 5-10 kg, start regular exercise, change eating habits that lead to high cholesterol and weight gain, etc. The days ahead will not always be easy, but you must steadily move forward to regain your strength and health.
Emotions
It is normal if you feel upset or depressed after discharge. Temporary low mood is normal and will gradually go away as you get back into your regular life and work.
However, sometimes a depressed mood can slow you down in returning to normal life. If your depressed mood only gets worse and is accompanied by other symptoms that accompany you every day for more than a week, you need treatment from a specialist.
Without treatment, depression will only get worse. For heart patients, depression can result in the development of a heart attack. Your doctor may refer you to a specialist to determine the treatment you need.
Diet
Because you may initially experience loss of appetite and good nutrition is important in wound healing, you may be discharged on an ad libitum diet. After 1-2 months, you need to switch to a diet with a small amount of animal fats, sugar and salt. Products high in fiber, complex carbohydrates, and healthy vegetable oil (corn, olive, sunflower, flaxseed) are beneficial.
Anemia is a common condition after surgery. It can be partially eliminated by foods high in iron: liver, red meat, rose hips, pomegranate, etc. If you have been prescribed an iron-containing drug, remember that it can turn the stool black and cause constipation, as well as dyspepsia. In this case, take the medicine with food.
How to care for a seam
The following is very important:
- Keep the seam area clean and dry.
- Use only soap and water to wash the area.
- Do not use ointments, oils, rubs or compresses until you are specifically told to do so.
Shower: Wet your palm or washcloth with soapy water and gently scrub up and down the seam area. Do not rub the seam area with a washcloth until all the crusts come off and the seam is completely healed. The water should be warm - not hot and not cold. Water that is too hot or too cold can cause you to faint.
Contact your doctor if signs of infection appear:
- Increased discharge from the wound
- The edges of the wound have separated
- Redness and swelling appeared in the suture area.
- Increased body temperature (above 38 degrees Celsius)
- If you have diabetes and your sugar levels are much higher than usual.
Pain relief
At first, you will experience discomfort in the chest muscles, in the suture area and in the chest as a whole with active movement. Itching, a feeling of stiffness in the suture area, or loss of sensitivity are normal after surgery. You should not have chest pain similar to what you experienced before surgery. Before discharge, you will be advised to take painkillers and anti-inflammatory medications. If you have had CABG surgery, then in addition to pain in your chest, you will also have pain in your leg, where the vein for the bypass was taken from. Daily walks, moderate activity and time will help you manage your leg discomfort.
Be sure to consult a doctor if you experience mobility or clicking in the sternum when moving.
Swelling
You will return home with some swelling in your legs and feet, especially if you had a vein removed for bypasses. If you notice swelling:
- While resting, try to keep your leg(s) in an elevated position. The easiest way to do this is to lie on a sofa or bed and prop your feet up on some pillows, or lie down on the floor and prop your feet up on a sofa. Do this three times a day for an hour and the swelling will noticeably decrease.
(Important: just lying on your back does not elevate your legs enough).
- Don't cross your legs when sitting.
- Walk daily, even if your feet are swollen.
- Use compression stockings.
Contact your doctor if your legs become swollen and become painful, especially if you experience shortness of breath when moving.
Activity
Gradually increase your activity every day, week, month. Listen to what your body says: rest if you are tired, have shortness of breath, or have chest pain.
First week at home
Walk on level ground 2-3 times a day. Start with the same time and distance as the last days in the hospital. You can do 150-300 meters. If necessary, stop for a short rest. Always take these walks before meals. You are shown quiet activities: drawing, solving crosswords, reading, etc. Try walking up and down stairs. Go out with someone in the car for a short distance.
Second week at home
Lift and carry light objects (up to 5 kg). The weight should be evenly distributed on both hands. Increase your walking to 600-700 meters. Do light housework: wipe the dust, set the table, wash the dishes, cook while sitting.
Third week at home
You can do chores in the yard, but avoid straining and prolonged bending or working with your arms raised. Start walking at a distance of 800-900 meters.
Fourth week at home
Gradually increase your walk to 1 km. You can lift things up to 7 kg. If your doctor allows it, you can start driving on your own. Do things like sweeping, vacuuming, washing the car, cooking.
Fifth to eighth week at home
At the end of the 6th week, the sternum should have healed. Continue to continually increase your activity. You can lift weights up to 10 kg. Play tennis, swim. On a personal plot you can weed and work with a shovel, at home you can move furniture (light). If your job does not involve heavy physical activity, you can return to it. It all depends on your physical condition and type of work.
Medications
You will need to take medications after surgery. Your doctor will tell you how long you will have to take the medications - just for the first time or for life. Make sure you understand the names of the medications, what they do and how often you should take them. Take only those medications that have been prescribed to you. Discuss with your doctor whether you need to take the medications you took before surgery. Do NOT take new medications (dietary supplements, pain relievers, cold medications) or increase the dosage of old ones without consulting your doctor. If you forget to take a pill today, do not take two at once tomorrow. It is recommended that you carry a list of your medications with you at all times.
Here is a list and characteristics of the most commonly prescribed drugs:
Antiplatelet agents are medications to prevent the formation of blood clots. They affect platelets, reducing their ability to stick together and attach to damaged artery walls. These include aspirin and clopidogrel. The drugs have a negative effect on the mucous membrane of the stomach and intestines and can cause the formation of erosions and ulcers. If you have a high risk of developing gastrointestinal ulcers, you need to take gastroprotectors : pantoprazole, lansoprazole, omeprazole, etc.
Medicines that lower cholesterol levels: statins (atorvastatin, rosuvastatin, simvastatin, lomestatin), fibrates (fenofibrate). They reduce the level of “bad” fractions of blood lipids and can increase “good” cholesterol. It is especially important to take these drugs for patients after coronary artery bypass surgery.
Beta blockers . By reducing heart rate, blood pressure, and the force of contraction of the heart muscle, these medications reduce the load on the heart. These include metoprolol, bisoprolol, nebivolol, carvedilol, etc. When taking them, it is necessary to monitor the pulse. The optimal frequency is 60±5 per minute at rest. The dose of such a drug is increased gradually, and withdrawal should not be abrupt. When prescribing this group of drugs, it is necessary to take into account the presence of diabetes and asthma.
Angiotensin-converting enzyme inhibitors (enalapril, lisinopril, monopril, perindopril, ramiril): reduce blood pressure, help reduce the load on the heart, and prevent thickening of the walls of blood vessels. The most common side effect is a dry cough. When it appears, it is possible to use sartans that do not have this side effect (valsartan, losartan, candesartan).
Calcium channel blockers : amlodipine, lercanidipine, nifedipine sustained release. They relax the walls of blood vessels and reduce blood pressure. When taking them, swelling in the legs, dizziness, and headache are possible.
Diuretics (diuretics ). Designed to remove excess fluid and salt from the body. Used to treat arterial hypertension and heart failure. The most commonly prescribed drugs are furosemide, hydrochlorothiazide, indopamide, torasemide, and spironolactone. If you have signs of heart failure and are taking diuretics, be sure to weigh yourself regularly; weight gain may be due to excess fluid in the body. Possible side effects - convulsions, spasms.
IMPORTANT! If you have had heart valve surgery, you need to prevent any type of infection to prevent the development of infective endocarditis. This includes taking antibiotics before you have any invasive procedure, dental procedure, or surgery. Your doctor will explain in more detail how to reduce the risk of complications.
So: follow your doctor's recommendations, lead a healthy lifestyle, eat right, be positive, and you will help your heart beat confidently and for a long time!
Prepared by S.A. Brishteleva, a cardiologist at the RCC of the Central District.
Diagnostic methods in Medscan
The doctor determines the pathological condition using physical methods - percussion and auscultation. With increasing edema, a phonendoscope can be used to hear wheezing over the entire surface of the lungs.
The Medscan diagnostic center uses the following methods to determine excess fluid in the lungs due to oncology:
- X-ray of the chest cavity. The examination will show a significant amount of fluid.
- CT, MRI are more accurate methods. They allow you to assess the condition of the lung tissues and identify the affected lymph nodes near the bronchi or in the mediastinum.
- Immunohistochemical analysis. It is carried out to study the pleural effusion in detail. Immunohistochemistry helps identify and characterize malignant cells based on the interaction of the immune complex of antibodies and antigens.
- Thoracoscopy is a method that allows you to examine the chest using a special tube (thoracoscope). In combination with an immunohistochemical study, it diagnoses a malignant neoplasm in almost 100% of cases.
The Medscan diagnostic center has expert-level equipment. We offer our patients modern and highly accurate laboratory and instrumental diagnostic methods.
Prevention of ventilator-associated pneumonia after myocardial revascularization operations
Nosocomial pneumonia (NP) ranks third in the structure of all hospital infectious complications after soft tissue and urinary tract infections, significantly increasing the duration and cost of hospital treatment, as well as mortality. The latter figure, in the case of NP, is, according to various authors, from 20 to 50% [2, 4, 5, 16]. According to studies conducted by JY Fagon et al. (1993), in patients in intensive care units (ICU), NP develops 5–10 times more often than in patients in general surgery departments; The average incidence of NP in the ICU is 25%.
Ventilator-associated pneumonia (VAP) is considered to be NP that occurs 48 hours or more after tracheal intubation and mechanical ventilation (ALV) in the absence of signs of pneumonia at the time of intubation [13]. VAP is an independent prognostic sign of unfavorable outcome in critically ill patients requiring mechanical ventilation [5]. The serious consequences of VAP, especially in surgical patients, are associated with the fact that pulmonary infection is a complication that develops against the background of the patient’s already existing critical condition, which required replacement of respiratory function.
It is obvious that optimizing the prevention of NP can significantly improve the prognosis in severely ill patients who are on mechanical ventilation for a long time.
In connection with the above, the purpose of this work is to demonstrate the effectiveness of the preventive use of ambroxol against the development of ventilator-associated pneumonia in patients with developed complications who require long-term mechanical ventilation after coronary artery bypass surgery under cardiopulmonary bypass (CPB).
The study involved 53 patients who underwent surgery for existing coronary artery disease. The operations were performed under conditions of artificial circulation.
All patients immediately after transfer from the operating room to the ICU and throughout the entire postoperative period underwent standard monitoring of the state of the cardiovascular system, acid-base and water-electrolyte balance. Artificial ventilation of the lungs was carried out with a microprocessor ventilator “Puritan Bennet 7200a” from Puritan Bennet, USA.
This study included only those patients whose severity of condition did not meet the standard criteria for extubation, as a result of which mechanical ventilation was required for more than 48 hours. All patients were divided into two groups. The first of them consisted of 32 patients; The scheme for preventing the development of nosocomial pneumonia in this group was generally accepted for intensive care units. The second group included 21 patients; the protocol of preventive measures included ambroxol (ambrobene ampoules, Ratiopharm) at a dose of 15 mg intravenously 3 times a day.
There were no significant differences between the two groups (Table 1).
Due to acute cardiovascular failure, patients received infusion of catecholamines in various combinations (of which 10 patients of the first group and 9 patients of the second group - in combination with intra-aortic balloon counterpulsation).
The main reasons for long-term mechanical ventilation were acute heart failure, cerebrovascular complications, and pulmonary complications.
In most patients after coronary bypass surgery, extubation is possible within a few hours, and after 7–10 days they can be discharged from the clinic. At the same time, the number of initially severe patients with concomitant chronic diseases is increasing; treatment of such patients in the postoperative period requires long-term mechanical ventilation.
The reasons for prolonged mechanical ventilation are varied: hematological, respiratory, neurological, cardiovascular (see Table 2). In addition, in a given patient, the cause may change over time. For example, a patient could not be extubated initially due to increased blood flow through the drains; later, secondary causes may be hemodynamic instability, cardiogenic pulmonary edema, non-cardiogenic pulmonary edema due to massive blood transfusion, repeated anesthesia if rethrocotomy is necessary. Respiratory failure as a component of multiple organ failure in the structure of postoperative complications in coronary patients is of great clinical importance and is associated with a high risk of mortality.
As a result of the analysis, it was found that in the first group of patients, the incidence of VAP development was 31% (10 patients). Since the use of preventive administration of ambroxol in practice for the treatment of complications in patients on long-term mechanical ventilation, the incidence of VAP in this category of patients has decreased and amounted to 9.5% (2 patients).
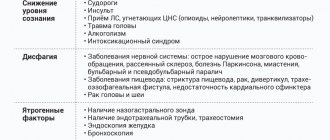
The problem of VAP has been intensively studied for 20 years. It has been proven that tracheal intubation is the cause of the development of this type of pneumonia [3, 11]. Risk factors for the development of VAP are considered to be chronic obstructive pulmonary diseases, mechanical ventilation lasting more than 48 hours, repeated intubation and aspiration, position of the patient on the back without raising the head, use of antibiotics, age over 60 years, multiple organ failure (three components or more), enteral nutrition and coma, aerosol therapy, male gender, tracheostomy, transportation of the patient outside the ICU [3, 9].
The problem of VAP remains relevant as long as invasive mechanical ventilation is used in medicine with the need to intubate the patient, since tracheal intubation itself creates conditions for the occurrence of pneumonia [3, 9, 11].
Low-cost methods of preventing pneumonia (compliance with the anti-epidemic regime, sanitizing the hands of personnel, proper patient care) significantly reduce the risk of developing pneumonia, but are not able to prevent it completely [9].
Prevention of VAP should be based on a clear understanding of risk factors, as well as the mechanisms of pathogenesis.
Anti-infective protection of the lower respiratory tract is carried out due to mechanical factors (aerodynamic filtration, branching of the bronchi, epiglottis, coughing and sneezing, oscillatory movements of the cilia of the ciliated epithelium of the bronchial mucosa), as well as cellular humoral mechanisms of nonspecific and specific immunity. The reasons for the development of an inflammatory reaction in the respiratory parts of the lungs can be either a decrease in the effectiveness of the protective mechanisms of the macroorganism, or the massive doses of microorganisms and/or their increased virulence. Four pathogenetic mechanisms can be distinguished that, to one degree or another, determine the development of pneumonia: aspiration of oropharyngeal secretions, inhalation of an aerosol containing microorganisms, hematogenous spread of microorganisms from an extrapulmonary source of infection, direct spread of infection from neighboring affected areas [9].
However, it should be noted that the main one of these mechanisms is aspiration of microorganisms. Instrumental studies of the respiratory tract and gastrointestinal tract, impaired consciousness and mechanical ventilation significantly increase the likelihood of aspiration. Aspiration of the contents of the oropharynx is the main route of infection of the respiratory parts of the lungs, and therefore the main pathogenetic mechanism for the development of pneumonia. Colonization of the oropharynx of hospitalized patients with gram-negative flora is a factor predisposing to NP. Colonization increases significantly when antibiotics are prescribed, in coma, in patients with hypotension, acidosis, azotemia, diabetes, chronic lung diseases, endotracheal and nasogastric intubation. The intensity and duration of colonization are significantly influenced by the virulence of microorganisms and impaired resistance of the macroorganism [9]. Under normal conditions, a number of microorganisms can colonize the oropharynx, but the lower respiratory tract remains sterile.
When the “self-cleaning” mechanisms of the tracheobronchial tree are damaged, favorable conditions are created for the development of pneumonia. For example, the presence of an endotracheal tube in the trachea, a nasogastric tube, and reflex hypersalivation ultimately lead to the appearance of a viscous secretion in the lumen of the trachea and large bronchi, creating conditions for bronchial obstruction. Contamination of this content leads to tracheobronchitis and bronchopneumonia.
We have developed preventive therapy, the effectiveness of which is demonstrated by a significant reduction in the incidence of nosocomial pneumonia in patients on mechanical ventilation for more than 48 hours. Patients with complications in the postoperative period, as a result of which were on mechanical ventilation for a long time, were prescribed ambrobene (ambroxol) for prophylactic purposes. Thus, thanks to the administration of Ambrobene, only two patients developed pneumonia, which was 9.5% in relation to the equally severe group of ICU patients who were on mechanical ventilation for up to 45 days. Otherwise, pneumonia as a serious infectious complication developed in 31% of patients.
Ambroxol stimulates the formation of low-viscosity tracheobronchial secretions due to the depolymerization of acidic mucopolysaccharides of bronchial mucus and the production of neutral mucopolysaccharides by goblet cells. Important is the ability of the drug to restore mucociliary clearance by stimulating the motor activity of the cilia of the ciliated epithelium [8]. Ambroxol improves mucociliary transport, which, in combination with the mucokinetic effect, causes a pronounced expectorant effect.
When used in combination with antibiotics, ambroxol enhances their penetration into the bronchial secretions and bronchial mucosa, increasing the effectiveness of antibacterial therapy and reducing its duration [12, 14].
In addition to its effect on mucus production in the respiratory tract, ambroxol also has anti-inflammatory [1, 5] and antioxidant [7] properties, which can be explained by its effect on the release of oxygen radicals and interference with the metabolism of arachidonic acid at the site of inflammation.
But the most significant advantage of the drug is its stimulating effect on type 2 alveolocytes, which leads to increased synthesis and secretion of surfactant [18]. The drug is able to block its decay under the influence of unfavorable factors. Being one of the components of the local lung defense system, surfactant prevents the penetration of pathogenic microorganisms into epithelial cells. Surfactant also enhances the activity of the cilia of the ciliated epithelium, which, in combination with improving the rheological properties of bronchial secretions, leads to effective cleansing of the respiratory tract and helps the patient to cough properly.
In the work of R. R. Wauer et al. [17] were able to show that the administration of ambroxol significantly reduces the risk of developing pneumonia in children with RDS, and also improves pulmonary mechanics. Our study also demonstrated that the administration of ambroxol to patients on long-term mechanical ventilation after cardiac surgery affects several parts of the pathogenesis of pneumonia and helps prevent the development of VAP.
Parenteral administration of ambroxol is optimal in ICU conditions. From this point of view, the most convenient are drugs produced in various forms. Our department used the drug Ambrobene (Ratiopharm), which is available in tablets, capsules, solution for oral administration and inhalation, and in ampoules for parenteral administration.
Based on all of the above, we can conclude that the developed method for the prevention of ventilator-associated pneumonia significantly reduces the incidence of this infectious complication in patients after open-heart surgery who are on mechanical ventilation for more than 48 hours.
E. S. Nikitin , Doctor of Medical Sciences M. M. Zhadin , Candidate of Medical Sciences G. V. Lobacheva , Candidate of Medical Sciences E. P. Eliseeva, E. Nikolaeva, I. M. Makrushin Scientific Center for Cardiovascular Surgery named after. A. N. Bakuleva RAMS, Moscow
Treatment methods in Medscan
The Medscan clinic provides all the necessary treatment used for oncology of the lungs, pelvic organs and other internal organs:
- Surgical intervention.
- Radiotherapy.
- Chemotherapy.
- Targeted therapy.
- Immunotherapy.
- Hormone therapy.
Treatment of excess fluid in the lungs during acute pulmonary edema involves intravenous diuretics and the use of an oxygen mask. The patient is recommended cardiological and vascular drugs to stabilize chronic heart diseases.
If fluid in the lungs is a side effect of radiation therapy or chemotherapy, we will resolve this issue as quickly as possible. Our specialists will select the safest oncological treatment options for your health.