Lipoproteins are a complex of lipids with proteins that are part of any living organism. Lipoproteins take part in the functions of transport and storage of lipids and are considered an integral component of the morphological structure of the cell.
During diagnostic testing to identify various diseases, specialists often pay attention to the percentage of lipid-protein complexes in the body.
In addition, beta lipoproteins and alpha lipoproteins can be used in establishing paternity or in forensic practice to identify physical evidence. Lipoproteins can be free, soluble in an aqueous environment, or structural.
Functions and meaning
Lipids play an important role in the human body. They are found in all cells and tissues and participate in many metabolic processes.
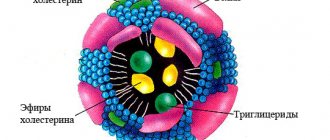
lipoprotein structure
- Lipoproteins are the main transport form of lipids in the body
. Since lipids are insoluble compounds, they cannot independently fulfill their purpose. Lipids bind in the blood to proteins - apoproteins, become soluble and form a new substance called lipoprotein or lipoprotein. These two names are equivalent, abbreviated as LP.
Lipoproteins occupy a key position in the transport and metabolism of lipids. Chylomicrons transport fats that enter the body with food, VLDL deliver endogenous triglycerides to the site of disposal, cholesterol enters cells with the help of LDL, HDL has anti-atherogenic properties.
- Lipoproteins increase the permeability of cell membranes.
- LPs, the protein part of which is represented by globulins, stimulate the immune system, activate the blood coagulation system and deliver iron to the tissues.
Classification
Blood plasma lipids are classified by density
(using the ultracentrifugation method). The more lipids a drug molecule contains, the lower their density. There are VLDL, LDL, HDL, and chylomicrons. This is the most accurate of all existing drug classifications, which was developed and proven using a precise and rather painstaking method - ultracentrifugation.
The size of the LP is also heterogeneous.
The largest molecules are chylomicrons, and then in decreasing size - VLDL, LPSP, LDL, HDL.
Electrophoretic classification
LP is very popular among clinicians. Using electrophoresis, the following classes of lipid were identified: chylomicrons, pre-beta lipoproteins, beta lipoproteins, alpha lipoproteins. This method is based on the introduction of an active substance into a liquid medium using a galvanic current.
Fractionation
LPs are carried out to determine their concentration in the blood plasma. VLDL and LDL are precipitated with heparin, and HDL remains in the supernatant.
Kinds
Currently, the following types of lipoproteins are distinguished:
HDL (high density lipoprotein)
HDL transports cholesterol from body tissues to the liver.
HDL contains phospholipids, which keep cholesterol in suspension and prevent it from leaving the bloodstream. HDL is synthesized in the liver and provides reverse transport of cholesterol from surrounding tissues to the liver for disposal.
- An increase in HDL in the blood is observed in obesity, fatty hepatosis and biliary cirrhosis of the liver, and alcohol intoxication.
- A decrease in HDL occurs in hereditary Tangier disease, caused by the accumulation of cholesterol in tissues. In most other cases, a decrease in the concentration of HDL in the blood is a sign of atherosclerotic vascular damage.
The HDL level differs between men and women. In males, the LP value of this class ranges from 0.78 to 1.81 mmol/l, the norm in women for HDL is from 0.78 to 2.20, depending on age.
LDL (low density lipoprotein)
LDLs are carriers of endogenous cholesterol, triglycerides and phospholipids from the liver to tissues.
This class of drugs contains up to 45% cholesterol and is its transport form in the blood. LDL is formed in the blood as a result of the action of the enzyme lipoprotein lipase on VLDL. When there is an excess of it, atherosclerotic plaques appear on the walls of blood vessels.
Normally, the amount of LDL is 1.3-3.5 mmol/l.
- The level of LDL in the blood increases with hyperlipidemia, hypothyroidism, and nephrotic syndrome.
- A reduced level of LDL is observed with inflammation of the pancreas, hepatic-renal pathology, acute infectious processes, and pregnancy.
infographics (click to enlarge) – cholesterol and LP, role in the body and norms
VLDL (very low density lipoprotein)
VLDL is formed in the liver. They transport endogenous lipids, synthesized in the liver from carbohydrates, to tissues.
These are the largest LPs, second in size only to chylomicrons. They are more than half triglycerides and contain small amounts of cholesterol. When there is an excess of VLDL, the blood becomes cloudy and takes on a milky tint.
VLDL is a source of “bad” cholesterol, from which plaques form on the vascular endothelium. Gradually, the plaques increase, and thrombosis occurs with the risk of acute ischemia. VLDL is elevated in patients with diabetes and kidney disease.
Chylomicrons
Chylomicrons are absent in the blood of a healthy person and appear only in cases of lipid metabolism disorders
. Chylomicrons are synthesized in the epithelial cells of the small intestinal mucosa. They deliver exogenous fat from the intestine to peripheral tissues and the liver. Most of the transported fats are triglycerides, as well as phospholipids and cholesterol. In the liver, under the influence of enzymes, triglycerides break down and fatty acids are formed, some of which are transported to muscles and adipose tissue, and the other part is bound to blood albumin.
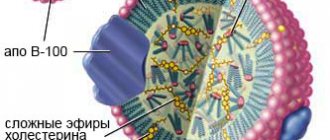
what do major lipoproteins look like?
LDL and VLDL are highly atherogenic
– containing a lot of cholesterol. They penetrate the artery wall and accumulate there. When metabolism is disrupted, LDL and cholesterol levels rise sharply.
HDL are the safest against atherosclerosis
. Lipoproteins of this class remove cholesterol from cells and promote its entry into the liver. From there, it enters the intestines along with bile and leaves the body.
Representatives of all other classes of drugs deliver cholesterol into cells. Cholesterol is a lipoprotein that is part of the cell wall. It is involved in the formation of sex hormones, the process of bile formation, and the synthesis of vitamin D, necessary for the absorption of calcium. Endogenous cholesterol is synthesized in liver tissue, adrenal cells, intestinal walls and even in the skin. Exogenous cholesterol enters the body along with animal products.
Categories of lipoproteins
Molecules loaded with cholesterol are much larger than those that lack it. The mass of cholesterol affects the density of the molecule. The higher the mass, the greater the density. According to the level of density, lipoproteins are divided into the following categories:
LDL cholesterol - what is it?
- Chylomicrons. What it is? Molecules of a super-volumetric structure that are formed in the intestines and disintegrate in the circulatory system under the influence of a certain category of enzymes on cholesterol and the residue utilized by the liver. Chylomicrons are able to ensure the fullest degree of digestibility of cholesterol in the intestine.
- Extremely low density lipoproteins are similar to chylomicrons. The main difference is the transportation of cholesterol by lipoproteins, which is formed in the liver, and not what is absorbed into the digestive tract. Once in the circulatory system, this category of lipoproteins begins to break down into low-density lipoproteins, which release cholesterol for the needs of the tissue.
- Low-density lipoproteins (LDL) are the main carriers of cholesterol in the body. Despite their lightness and mobility, lipoproteins are capable of carrying a large percentage of cholesterol. The transformation of this category of lipoproteins from the previous one occurs through the stage of intermediate-density lipoproteins. The latter are not able to perform significant functions in the body due to their short lifespan.
- High-density lipoproteins (HDL) are among the fastest and lightest compounds of transport proteins and cholesterol. The compound is able to be synthesized in the liver and transport cholesterol in the blood plasma. There were no significant differences in functioning between low- and high-density lipoproteins.
High blood cholesterol may be a consequence of taking sex hormones or contraceptives
A disturbance in the exchange of HDL and LDL should be a reason to visit a doctor.
What do beta lipoproteins do?
The main purpose of lipoproteins is considered to be the transportation of cholesterol in the body. However, in addition to this, they take an active part in the transport of carotenoids and triglycerides. Due to the dissolution of beta lipoproteins in the blood plasma, a precipitate is formed, which begins to settle on the walls of blood vessels.
With a normal amount of cholesterol in the body, the sediment can be independently processed and removed from the circulatory system. With elevated cholesterol levels, atherosclerotic plaques begin to appear and grow, leading to stroke and heart attack.
Dyslipoproteinemia is a diagnosis for disorders of lipoprotein metabolism
Dyslipoproteinemia develops when two processes are disrupted in the human body: the formation of lipoproteins and the rate of their elimination from the blood. An imbalance in the ratio of LP in the blood is not a pathology, but a factor in the development of a chronic disease,
in which the arterial walls become denser, their lumen narrows and the blood supply to the internal organs is disrupted.
When cholesterol levels in the blood increase and HDL levels decrease, atherosclerosis develops, leading to the development of deadly diseases.
Etiology
Primary
dyslipoproteinemia is genetically determined.
Causes of secondary
dyslipoproteinemias are:
- Physical inactivity,
- Diabetes,
- Alcoholism,
- Kidney dysfunction
- Hypothyroidism,
- Hepatic-renal failure,
- Long-term use of certain medications.
The concept of dislipoproteinemia includes 3 processes - hyperlipoproteinemia, hypolipoproteinemia, alipoproteinemia. Dyslipoproteinemia is quite common: every second inhabitant of the planet experiences similar changes in the blood.
Hyperlipoproteinemia is an increased level of lipoproteins in the blood due to exogenous and endogenous causes.
The secondary form of hyperlipoproteinemia develops against the background of the underlying pathology. In autoimmune diseases, drugs are perceived by the body as antigens to which antibodies are produced. As a result, antigen-antibody complexes are formed, which are more atherogenic than the drugs themselves.
- Type 1 hyperlipoproteinemia is characterized by the formation of xanthomas - dense nodules containing cholesterol and located above the surface of the tendons, the development of hepatosplenomegaly, and pancreatitis. Patients complain of a deterioration in their general condition, a rise in temperature, loss of appetite, and paroxysmal abdominal pain, which intensifies after eating fatty foods.
Xanthomas (left) and xanthelasmas (center and right) are external manifestations of dyslipoproteinemia
- In type 2, xanthomas are formed in the area of the tendons of the feet and xanthelasmas in the periorbital zone.
- Type 3 – symptoms of cardiac dysfunction, the appearance of pigmentation on the skin of the palm, soft inflamed ulcers over the elbows and knees, as well as signs of damage to the blood vessels of the legs.
- With type 4, the liver enlarges, coronary heart disease and obesity develop.
Alipoproteinemia is a genetically determined disease
with an autosomal dominant type of inheritance. The disease is manifested by enlarged tonsils with an orange coating, hepatosplenomegaly, lymphadenitis, muscle weakness, decreased reflexes, and hyposensitivity.
Hypolipoproteinemia –
low levels of LP in the blood,
often asymptomatic. The causes of the disease are:
- Heredity,
- Poor nutrition
- Passive lifestyle,
- Alcoholism,
- Pathology of the digestive system,
- Endocrinopathy.
Dyslipoproteinemias are: organ or regulatory,
toxigenic, basal - study of the level of LP on an empty stomach, induced - study of the level of LP after eating, drugs or exercise.
Diagnostics
It is known that excess cholesterol is very harmful for the human body. But a lack of this substance can lead to dysfunction of organs and systems. The problem lies in hereditary predisposition, as well as in lifestyle and dietary habits.
Diagnosis of dyslipoproteinemia is based on medical history, patient complaints, clinical signs - the presence of xanthoma, xanthelasma, lipoid arch of the cornea.
The main diagnostic method for dyslipoproteinemia is a blood lipid test. The atherogenicity coefficient and the main indicators of the lipid profile - triglycerides, total cholesterol, HDL, LDL - are determined.
A lipidogram is a laboratory diagnostic method that identifies lipid metabolism disorders that lead to the development of heart and vascular diseases. A lipidogram allows the doctor to assess the patient’s condition, determine the risk of developing atherosclerosis of the coronary, cerebral, renal and hepatic vessels, as well as diseases of the internal organs. Blood is donated to the laboratory strictly on an empty stomach, at least 12 hours after the last meal. One day before the test, avoid drinking alcohol, and an hour before the test, avoid smoking. On the eve of the analysis, it is advisable to avoid stress and emotional overstrain.
The enzymatic method for studying venous blood is the main one for determining lipids. The device records samples pre-stained with special reagents. This diagnostic method allows you to conduct mass examinations and obtain accurate results.
It is necessary to take tests to determine the lipid spectrum for preventive purposes, starting from youth, once every 5 years. Persons over 40 years of age should do this annually.
Blood tests are carried out in almost every district clinic. Patients suffering from hypertension, obesity, heart, liver and kidney diseases are prescribed a biochemical blood test and a lipid profile. Family history, existing risk factors, monitoring the effectiveness of treatment are indications for prescribing a lipid profile.
The results of the study may be unreliable after eating food the day before, smoking, stress, acute infection, pregnancy, or taking certain medications.
Diagnosis and treatment of pathology is carried out by an endocrinologist, cardiologist, therapist, general practitioner, and family doctor.
Low-density lipoproteins are the main carriers of cholesterol (cholesterol) in the body. The cholesterol they contain is considered “harmful”, since its excess increases the risk of plaques appearing in the arteries, which can lead to blockage and cause a heart attack or stroke.
Synonyms Russian
LDL, low-density lipoprotein, LDL, LDL-C, low-density lipoprotein cholesterol, beta-lipoprotein cholesterol, beta-lipoprotein, beta-LP.
English synonyms
LDL, LDL-C, low-density lipoprotein cholesterol, Low-density lipoprotein.
Research method
Colorimetric photometric method.
Units
mmol/l (millimoles per liter).
What biomaterial can be used for research?
Venous blood.
How to properly prepare for research?
- Do not eat for 12 hours before the test.
- Avoid physical and emotional stress and do not smoke for 30 minutes before the test.
General information about the study
Cholesterol (CH, cholesterol) is a fat-like substance vital to the body. The correct scientific name for this substance is “cholesterol” (the ending -ol indicates that it belongs to alcohols), however, the name “cholesterol” has become widespread in the popular literature, which we will use later in this article. Cholesterol is involved in the formation of cell membranes of all organs and tissues of the body. Cholesterol is used to create hormones that are necessary for the development of the body and the reproduction function. Bile acids are formed from cholesterol, with the help of which fats are absorbed in the intestines.
Cholesterol is insoluble in water, so to move around the body it is “packed” into a protein shell consisting of apolipoproteins. The resulting complex (cholesterol + apolipoprotein) is called lipoprotein. Several types of lipoproteins circulate in the blood, differing in the proportions of their components:
- very low density lipoproteins (VLDL),
- low density lipoproteins (LDL),
- high density lipoproteins (HDL).
LDL cholesterol is considered “bad” because when it is in excess, plaques appear in the walls of blood vessels, which can restrict the movement of blood through the vessel, which threatens atherosclerosis and significantly increases the risk of heart disease (coronary artery disease, heart attack) and stroke.
The liver produces enough cholesterol for the body's needs, but some of it comes from food, mainly fatty meat and fatty dairy products. If a person has a genetic predisposition to high cholesterol or eats too much animal fat, LDL levels in the blood can rise to dangerous levels.
What is the research used for?
- To assess the likelihood of atherosclerosis and heart problems (this is the most important indicator of the risk of developing coronary disease).
- To monitor the effectiveness of a diet with a reduced amount of animal fats.
- To monitor lipid levels after taking cholesterol-lowering medications.
When is the study scheduled?
An LDL test is usually part of a lipid profile, which also includes the determination of total cholesterol, VLDL cholesterol, HDL cholesterol, triglycerides and atherogenicity coefficient. A lipidogram may be prescribed during routine preventive examinations or when the concentration of total cholesterol increases, in order to find out which fraction is responsible for the increase.
In general, a lipid profile is recommended for all people over 20 years of age at least once every 5 years, but in some cases even more often (several times a year). First, if the patient is prescribed a diet limited in animal fats and/or is taking cholesterol-lowering medications, then it is checked whether he achieves the target level of LDL and total cholesterol and, accordingly, whether his risk of cardiovascular disease is reduced diseases. And, secondly, if the patient has one or more risk factors for developing cardiovascular diseases in his life:
- smoking,
- certain age (men over 45, women over 55),
- high blood pressure (from 140/90 mm Hg),
- high cholesterol or cardiovascular disease in family members (heart attack or stroke in a close male relative under 55 years of age or a female relative under 65 years of age),
- coronary heart disease, previous myocardial infarction or stroke,
- diabetes,
- excess body weight,
- alcohol abuse,
- eating large amounts of food containing animal fats,
- low physical activity.
If a child in the family had cases of high cholesterol or heart disease at a young age, then it is recommended that he take a lipid profile for the first time between the ages of 2 and 10 years.
What do the results mean?
Reference values:
The concept of “normal” is not entirely applicable to the level of LDL cholesterol. Different people with different numbers of risk factors in their lives will have different LDL levels. LDL cholesterol testing is used to determine the risk of cardiovascular disease, but to accurately determine it for any person, all factors must be taken into account.
Elevated LDL cholesterol levels may be the result of a hereditary predisposition (familial hypercholesterolemia) or excess dietary intake of animal fats. In most people with high cholesterol, both factors are involved to some extent.
According to clinical guidelines1, the level
“Diagnostics and correction of lipid metabolism disorders for the purpose of prevention and treatment of atherosclerosis. Russian recommendations, VII revision. 2020".
"2019 ESC/EAS Guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk."
Possible causes of elevated LDL cholesterol levels:
- cholestasis - stagnation of bile, which can be caused by liver disease (hepatitis, cirrhosis) or gallstones,
- chronic inflammation of the kidneys leading to nephrotic syndrome,
- chronic renal failure,
- decreased thyroid function (hypothyroidism),
- poorly treated diabetes mellitus,
- alcoholism,
- obesity,
- prostate or pancreatic cancer.
Reduced LDL cholesterol levels are not used in diagnosis due to low specificity. However, its reasons may be:
- hereditary hypocholesterolemia,
- severe liver disease,
- oncological diseases of the bone marrow,
- increased thyroid function (hyperthyroidism),
- inflammatory joint diseases,
- B12 or folate deficiency anemia,
- common burns,
- acute diseases, acute infections,
- chronic obstructive pulmonary disease.
What can influence the result?
Cholesterol concentrations may change from time to time, this is normal. A single measurement does not always reflect normal levels, so sometimes it may be necessary to retake the test after 1-3 months.
Increases very low-density lipoprotein cholesterol levels (VLDL cholesterol):
- pregnancy (lipid profile should be done at least 6 weeks after birth),
- long fasting,
- donate blood while standing,
- anabolic steroids, androgens, corticosteroids,
- smoking,
- eating food containing animal fats.
Reduce VLDL cholesterol levels:
- being in a lying position,
- allopurinol, clofibrate, colchicine, antifungal drugs, statins, cholestyramine, erythromycin, estrogens,
- intense physical activity,
- a diet low in cholesterol and saturated fatty acids and, conversely, high in polyunsaturated fatty acids.
Treatment
Diet therapy plays a huge role in the treatment of dyslipoproteinemia.
Patients are advised to limit the consumption of animal fats or replace them with synthetic ones, and eat up to 5 times a day in small portions. The diet must be enriched with vitamins and dietary fiber. You should avoid fatty and fried foods, replace meat with sea fish, and eat plenty of vegetables and fruits. General restorative therapy and sufficient physical activity improve the general condition of patients.
Figure: useful and harmful “diets” from the point of view of drug balance
Lipid-lowering therapy and antihyperlipoproteinemic drugs are intended to correct dyslipoproteinemia. They are aimed at reducing cholesterol and LDL levels in the blood, as well as increasing HDL levels.
Among the drugs for the treatment of hyperlipoproteinemia, patients are prescribed:
- Statins - Lovastatin, Fluvastatin, Mevacor, Zocor, Lipitor. This group of drugs reduces the production of cholesterol by the liver, reduces the amount of intracellular cholesterol, destroys lipids and has an anti-inflammatory effect.
- Sequestrants reduce cholesterol synthesis and remove it from the body - Cholestyramine, Colestipol, Cholestipol, Cholestan.
- Fibrates reduce triglyceride levels and increase HDL levels - Fenofibrate, Ciprofibrate.
- B vitamins.
Hyperlipoproteinemia requires treatment with lipid-lowering drugs “Cholesteramine”, “Nicotinic acid”, “Miscleron”, “Clofibrate”.
Treatment of the secondary form of dyslipoproteinemia consists of eliminating the underlying disease.
Patients with diabetes are advised to change their lifestyle, regularly take antihyperglycemic drugs, as well as statins and fibrates. In severe cases, insulin therapy is required. In case of hypothyroidism, it is necessary to normalize the function of the thyroid gland. For this purpose, patients undergo hormone replacement therapy.
Patients suffering from dyslipoproteinemia are recommended after the main treatment:
- Normalize body weight,
- Dose physical activity
- Limit or eliminate alcohol consumption,
- If possible, avoid stress and conflict situations,
- Stop smoking.
Cholesterol – low density lipoproteins (LDL)
Low-density lipoproteins are the main carriers of cholesterol in the body. The cholesterol they contain is considered “harmful”, since its excess increases the risk of plaques appearing in the arteries, which can lead to blockage and cause a heart attack or stroke.
Synonyms Russian
LDL, low-density lipoprotein, LDL, LDL-C, low-density lipoprotein cholesterol, beta-lipoprotein cholesterol, beta-lipoprotein, beta-LP.
English synonyms
LDL, LDL-C, low-density lipoprotein cholesterol, Low-density lipoprotein.
Research method
Colorimetric photometric method.
Units
mmol/l (millimoles per liter).
What biomaterial can be used for research?
Venous blood.
How to properly prepare for research?
- Do not eat for 12 hours before donating blood.
- Avoid physical and emotional stress and do not smoke for 30 minutes before the test.
General information about the study
Cholesterol is a fat-like substance vital to the body. It is involved in the formation of cell membranes of all organs and tissues of the body. Hormones are created on the basis of cholesterol, which are necessary for the development of the body and the implementation of the reproduction function. Bile acids are formed from it, with the help of which fats are absorbed in the intestines.
Cholesterol is insoluble in water, so to move around the body it is “packed” into a protein shell consisting of apolipoproteins. The resulting complex (cholesterol apolipoprotein) is called a lipoprotein. Several types of lipoproteins circulate in the blood, differing in the proportions of their components:
- very low density lipoproteins (VLDL),
- low density lipoproteins (LDL),
- high density lipoproteins (HDL).
LDL cholesterol is considered “bad” because when it is in excess, plaques appear in the walls of blood vessels, which can restrict the movement of blood through the vessel, which threatens atherosclerosis and significantly increases the risk of heart disease (coronary disease, heart attack) and stroke.
The liver produces enough cholesterol for the body's needs, but some of it comes from food, mainly fatty meat and fatty dairy products. If a person has a genetic predisposition to high cholesterol or eats too much animal fat, LDL levels in the blood can rise to dangerous levels.
What is the research used for?
- To assess the likelihood of atherosclerosis and heart problems (this is the most important indicator of the risk of developing coronary disease).
- To monitor the effectiveness of a diet with a reduced amount of animal fats.
- To monitor lipid levels after the use of cholesterol-lowering drugs.
When is the study scheduled?
The LDL test is usually part of a lipid profile, which also includes the determination of total cholesterol, VLDL cholesterol, HDL cholesterol, triglycerides and atherogenicity coefficient. A lipidogram may be prescribed during routine preventive examinations or when the concentration of total cholesterol increases, in order to find out which fraction is responsible for the increase.
In general, a lipid profile is recommended for all people over 20 years of age at least once every 5 years, but in some cases even more often (several times a year). First, if the patient is prescribed a low-fat diet and/or is taking cholesterol-lowering medications, then they are tested to see if they are achieving target LDL and total cholesterol levels and thus reducing their cardiovascular risk. diseases. And, secondly, if the patient has one or more risk factors for developing cardiovascular diseases in his life:
- smoking,
- certain age (men over 45, women over 55),
- high blood pressure (from 140/90 mm Hg),
- high cholesterol or cardiovascular disease in family members (heart attack or stroke in a close male relative under 55 years of age or a female relative under 65 years of age),
- coronary heart disease, previous myocardial infarction or stroke,
- diabetes,
- excess body weight,
- alcohol abuse,
- eating large amounts of food containing animal fats,
- low physical activity.
If a child in the family had cases of high cholesterol or heart disease at a young age, then it is recommended that he take a lipid profile for the first time between the ages of 2 and 10 years.
What do the results mean?
Reference values: 0 - 3.3 mmol/l.
The concept of “normal” is not entirely applicable to the level of LDL cholesterol. Different people with different numbers of risk factors in their lives will have different normal levels of LDL cholesterol. LDL cholesterol testing is used to determine the risk of cardiovascular disease, but to accurately determine it for any person, all factors must be taken into account.
Increased LDL cholesterol levels may be the result of a hereditary predisposition (familial hypercholesterolemia) or excess dietary intake of animal fats. In most people with high cholesterol, both factors are involved to some extent.
LDL cholesterol levels can be assessed as follows:
- less than 2.6 mmol/l – optimal,
- 2.6-3.3 mmol/l – close to optimal,
- 3.4-4.1 mmol/l – borderline high,
- 4.1-4.9 mmol/l – high,
- above 4.9 mmol/l – very high.
Possible reasons for increased LDL cholesterol levels:
- cholestasis - stagnation of bile, which can be caused by liver disease (hepatitis, cirrhosis) or gallstones,
- chronic inflammation of the kidneys leading to nephrotic syndrome,
- chronic renal failure,
- decreased thyroid function (hypothyroidism),
- poorly treated diabetes mellitus,
- alcoholism,
- obesity,
- prostate or pancreatic cancer.
Reduced LDL cholesterol levels are not used in diagnosis due to low specificity. However, its reasons may be:
- hereditary hypocholesterolemia,
- severe liver disease,
- oncological diseases of the bone marrow,
- increased thyroid function (hyperthyroidism),
- inflammatory joint diseases,
- B12—or folate deficiency anemia,
- common burns,
- acute diseases, acute infections,
- chronic obstructive pulmonary disease.
What can influence the result?
Cholesterol concentrations may change from time to time, this is normal. A single measurement does not always reflect normal levels, so sometimes it may be necessary to retake the test after 1-3 months.
Increases VLDL cholesterol levels:
- pregnancy (lipid profile should be done at least 6 weeks after birth),
- long fasting,
- donate blood while standing,
- anabolic steroids, androgens, corticosteroids,
- smoking,
- eating food containing animal fats.
Reduce VLDL cholesterol levels:
- being in a lying position,
- allopurinol, clofibrate, colchicine, antifungal drugs, statins, cholestyramine, erythromycin, estrogens,
- intense physical activity,
- a diet low in cholesterol and saturated fatty acids and, conversely, high in polyunsaturated fatty acids.
Important Notes
- A lipid profile should be taken when a person is relatively healthy. After an acute illness, heart attack, or surgery, you should wait at least 6 weeks before measuring cholesterol.
- LDL is usually calculated using the following formula: LDL cholesterol = total cholesterol - (HDL cholesterol - TG (triglycerides) / 2.2).
- In the USA, lipids are measured in milligrams per deciliter, in Russia and Europe - in millimoles per liter. Conversion is carried out using the formula: cholesterol (mg/dl) = cholesterol (mmol/l) × 38.5 or cholesterol (mmol/l) = cholesterol (mg/dl) x 0.0259.
- LDL cholesterol is usually calculated based on the results of other tests included in the lipid profile: total cholesterol, HDL cholesterol and triglycerides, another type of lipid that is part of lipoproteins. More often, a fairly accurate indicator is achieved, but if the triglyceride level is significantly elevated (> 10 mmol/l) or the person ate a lot of fatty foods before taking the test, the result may not be entirely correct. In this case, LDL is measured directly.
Also recommended
- Triglycerides
- Cholesterol – high density lipoprotein (HDL)
- Atherogenic coefficient
- Apolipoprotein A1
- Apolipoprotein B
Who orders the study?
General practitioner, therapist, cardiologist.