Hospitalization and treatment under the compulsory medical insurance quota. More details after viewing the pictures.
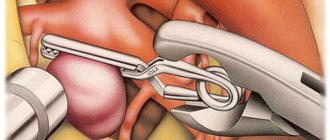
- Aneurysm clipping
A cerebral aneurysm is a local protrusion of the arterial walls. The disease often occurs without symptoms. As the brain aneurysm grows, a significant thinning of the walls of the formation occurs, which can lead to its rupture and the development of hemorrhagic stroke.
Depending on the shape, a cerebral aneurysm can be spindle-shaped or saccular. The exact type of disease can only be determined during a comprehensive diagnosis. Saccular aneurysm is much more common.
Causes of the disease
An aneurysm is a dangerous condition that primarily requires surgical treatment. Otherwise, complications will not be avoided. Experts believe that the disease is a consequence of developmental abnormalities that disrupt the structure of the vascular wall. Often, a cerebral aneurysm is combined with connective tissue dysplasia, polycystic kidney disease, and vascular disorders. The acquired form of the disease can be a consequence of traumatic brain injury. Also, a cerebral aneurysm occurs against the background of atherosclerosis and hypertension.
The vascular wall defect itself occurs gradually. Against the background of degenerative processes, tissue damage or underdevelopment, the area loses its former elasticity. Under the pressure of blood flow, the vascular wall begins to bulge. This is how a brain aneurysm forms. Most often, the formation occurs in the place where the arteries branch and there is the strongest pressure on the vessel wall.
Types of cerebral aneurysms
By development:
- True aneurysms (the area of the vessel evenly expands).
- False aneurysms (a hematoma is formed that communicates with the lumen of the vessel).
To size:
- Most aneurysms are small - less than 11 mm.
- Rarely, aneurysms reach 11–25 mm in diameter - average size .
- Aneurysms with a diameter exceeding 25 mm are called giant .
There are three types of aneurysms based on their shape:
- A saccular aneurysm is a round sac of blood attached by its neck to an artery, or perhaps to the site of a branch of a vessel. This is the most common form of cerebral artery aneurysm. More often they form in adults.
- A lateral aneurysm looks like a tumor on the wall of a blood vessel.
- Fusiform aneurysm is a diffuse expansion of the vessel wall over a significant extent.
According to the clinical course:
- Asymptomatic aneurysm (does not cause symptoms and is detected incidentally).
- Unruptured aneurysms (symptoms of compression of the brain and cranial nerves).
- Ruptured aneurysm (signs of intracranial bleeding).
Symptoms of an aneurysm
Two variants of the course of the disease can be distinguished: apoplexy and tumor-like. The characteristics of the clinical picture depend on the types of aneurysm. The tumor-like form of the disease is accompanied by an active course. In a short period of time, the aneurysm increases in size and compresses important anatomical structures of the brain.
A tumor-like aneurysm is most often localized in the area of the cavernous sinus or chiasm. When the chiasmal region is damaged, visual acuity decreases. Over a long period of time, optic nerve atrophy occurs. If a cerebral aneurysm is located in the cavernous sinus, paresis occurs and damage to the branches of the trigeminal nerve occurs. As the pathology develops, oculomotor disturbances occur and strabismus may appear.
Signs of a ruptured aneurysm
A sharp headache is the first symptom of a ruptured aneurysm. The pain syndrome is initially local in nature. But very quickly the headache spreads and becomes diffuse. In this case, patients note the appearance of nausea and repeated vomiting.
In the future, characteristic meningeal symptoms arise:
- stiffness of the neck muscles;
- Kernig's and Brudzinski's symptoms;
- loss of consciousness.
When a cerebral aneurysm ruptures, subarachnoid hemorrhage occurs. It may be accompanied by focal symptoms, which depend on the location of the formation. The most severe is hemorrhage into the ventricles, which often leads to the death of the patient.
With an aneurysm of the anterior cerebral artery, leg paresis develops, which is often combined with mental disorders. Damage to the middle cerebral artery leads to speech impairment and the development of hemiparesis.
If the pathology is localized in the area of the vertebrobasilar system, during the rupture of the aneurysm, swallowing disorders occur, nystagmus develops in combination with central paresis of the face and trigeminal nerve.
At the first sign of a possible aneurysm, you should immediately seek emergency medical help. It is important to maintain physical rest and avoid overexertion. Specialists will conduct an examination, diagnose, make an accurate diagnosis, and prescribe the necessary medications to reduce the risk of life-threatening complications.
Management of a patient with a ruptured cerebral artery aneurysm
After subarachnoid hemorrhage in a patient in stupor or coma, intracranial pressure may be increased. Therefore, it is necessary to maintain sufficient cerebral perfusion pressure (CPP) while ensuring that mean arterial pressure does not increase excessively. To assess alveolar ventilation in the lungs, the content of gases in arterial blood should be monitored. In case of hypercapnia, the patient requires artificial pulmonary ventilation (ALV). If a subdural or intracerebral hematoma causes an increase in neurological disorders, surgical removal is advisable. During the operation, the neurosurgeon can also remove the found aneurysm from the bloodstream using a vascular clip at its base.
To avoid recurrent hemorrhage, all patients are advised to rest in bed and placed in a quiet, preferably darkened room. To prevent constipation as a result of a sedentary state, which then forces the patient with an aneurysm to push, laxatives are prescribed. At the same time, excessive restrictions on activity can lead to anxiety, so the patient is allowed to read, listen to the radio, and meet with relatives. For severe headaches and pain in the neck, mild sedatives and analgesics are prescribed. Acetylsalicylic acid (aspirin), which has an antiplatelet effect, is not recommended, but paracetamol (acetaminophen) or meperidine and phenobarbital or other sedatives can be used. Excessive prescription of sedatives to a patient with a cerebral artery aneurysm is undesirable, since it complicates the assessment of his initial and possible neurological symptoms.
Epileptic seizures at the time of aneurysm rupture are rare. Minor trembling, twitching, and an extended posture in the patient often accompany loss of consciousness, probably due to a sharp increase in intracranial pressure. Because generalized seizures increase the risk of aneurysm re-rupture, phenytoin (300 mg daily) or phenobarbital (30 mg three times daily) is sometimes given as preventive therapy.
Steroid medications help reduce pain in the head and neck caused by the irritating effect of blood in the subarachnoid space. There are no data on their effectiveness in cerebral edema, sometimes observed in patients immediately after subarachnoid hemorrhage.
How is it diagnosed?
Since an arterial aneurysm can occur without significant symptoms, it is necessary to pay special attention to the first signs in women and men. A neurologist must diagnose the disease based on the examination, the diagnostic results obtained and the study of cerebrospinal fluid.
During a neurological examination, focal and meningeal symptoms are detected. Based on the location of complaints, it is possible to determine presumably where the pathological focus is located.
The neurologist obtains accurate information about the patient’s condition using the following studies:
- X-ray of the skull. A cerebral aneurysm is characterized by signs of bone tissue destruction.
- Computed tomography, magnetic resonance imaging of the brain.
- Angiography. Basic information about the location, shape and size of the brain aneurysm can be obtained.
- Lumbar puncture. The study reveals blood in the cerebrospinal fluid, which indicates the presence of hemorrhage.
Specialists carry out differential diagnosis of cerebral aneurysm. It is important to make an accurate diagnosis in a short time. This will avoid the adverse effects of a brain aneurysm. It is necessary to differentiate an aneurysm from tumor-like processes, cysts and abscesses.
Treatment of large and giant aneurysms
| Exclusion of a giant ICA aneurysm using the IAC technique |
Surgical treatment of large and giant aneurysms is one of the most difficult issues in vascular neurosurgery. In the 70s, surgical treatment for such patients was limited to ligation of the internal carotid artery in the neck, while postoperative mortality was 15.2%. With the advent of endovasal technology, it became possible to conduct a balloon occlusion test under EEG control followed by stationary occlusion of the ICA. In some cases, this treatment method was combined with the application of EICMA; however, postoperative mortality in the group of giant aneurysms remained high. Since 1995, the institute has developed and used a technique for intravascular aspiration of blood from an aneurysm. The ICA technique has proven to be very effective in the surgery of large and giant aneurysms of the ICA; it has made it possible to reduce postoperative mortality by 4 times and significantly reduce the group of patients who are denied surgical treatment. Currently, the department has the most experience in the world in applying the HAC technique.
| Shutdown of a large aneurysm using a flow-directing stent |
Along with direct interventions, endovascular methods have been used at the Institute for many years to treat large and giant aneurysms. Before the advent of stent-assistance and flow-directing stents, it was rarely possible to completely shut off such aneurysms with coils. The advent of stents has significantly changed the possibilities for endovascular treatment of large and giant aneurysms. Since the use of flow-directing stents, there has been a significant decrease in the proportion of deconstructive operations. There is no doubt that this technology has great prospects and in the near future will significantly change the structure of endovascular interventions in the treatment of aneurysms in general.
Principles of treatment
Aneurysm treatment is carried out by a neurologist. The operation is performed only by a neurosurgeon. Surgical methods are aimed primarily at preventing aneurysm rupture, which can result in the death of the patient. Conservative therapy for this pathology is used to slow the progression of the disease.
Surgical treatment of a cerebral aneurysm involves two types of main operations: clipping and endovascular occlusion. Surgery prevents the aneurysm from rupturing. A radical method of treatment is the removal of arteriovenous malformation during a microsurgical operation.
Aneurysm clipping
Aneurysm clipping is an open operation during which the neurosurgeon blocks blood flow in a certain area of the vessel and applies a clip. At the stage of preparation for surgery, specialists prescribe a procedure that allows them to stabilize the patient’s condition and minimize the risk of possible complications. Preventive examination makes it possible to identify possible disorders and diseases that can lead to adverse consequences of surgical intervention.
The operation is performed using modern microsurgical techniques through a small trepanation hole. During surgery, the neurosurgeon prevents rupture of the wall of the malformation.
After isolating the neck of the aneurysm, the specialist places a clip on it. Additional control with Doppler ultrasound allows you to assess the state of blood flow and ensure the effectiveness of the operation.
Treatment of an aneurysm using the clipping method is considered quite complex and should only be performed by an experienced neurosurgeon. A qualified specialist will do everything possible to ensure accurate and technically correct application of the clip. Otherwise, dangerous complications and a long rehabilitation period cannot be avoided.
The clip is applied to the neck of the aneurysm vessel. The accuracy of the neurosurgeon’s actions is confirmed by conducting high-quality diagnostics (Dopplerography) during the procedure.
Endovascular occlusion
During endovascular occlusion of an aneurysm, the neurosurgeon blocks the lumen of the dilated vessel with a special implant. The operation is used when clipping is not possible, for example, when the aneurysm is spindle-shaped. During surgery, a specialist inserts a catheter balloon through the femoral artery using angiographic control. It closes the lumen of the aneurysm. You can also use a microspiral to perform thrombosis. The choice remains with the attending physician. The microspiral in the cavity of the affected vascular area forms blood clots, which clog the lumen of the vessel and shut off the aneurysms from the blood circulation.
results
The results of patient treatment are presented in the table.
Results of treatment of patients with large and giant aneurysms of the SBB Note. OA - basilar artery, VA - vertebral artery, PICA - posterior inferior cerebellar artery, SMA - superior cerebellar artery, FD - flow diverter, flow-directing stent, AS - assisting stent, stent used for assistance.
In 7 patients, it was possible to achieve immediate exclusion of the aneurysm from the blood flow or a marked slowdown of blood flow in the aneurysm. In 6 cases, no increase in neurological symptoms was noted. In 1 patient with a combination of PICA aneurysm and AVM, increased diplopia was noted in the early postoperative period. A patient with a fusiform aneurysm of the middle and lower third of the trunk of the basilar artery, with a volumetric effect on the pons, was planned to implant a flow-directing stent into an assisting stent (with the aim of maximizing positioning of the flow-directing stent only in the area of the artery defect, assisting (in a relatively unchanged area) - the upper third main artery). In the early postoperative period (day 1), the patient developed symptoms of ischemic damage to the brain stem caused by thrombosis of the perforating branches of the basilar artery, which led to the patient’s death on the 3rd day after surgery.
In 2 cases, due to persistent symptoms, the second stage of surgery was performed, which consisted of decompressive trepanation of the posterior cranial fossa and removal of the aneurysm sac, which exerts a compressive effect on the brain stem (Fig. 2).
Rice. 2. Giant aneurysm of the right superior cerebellar artery. a, b, c — MRI in coronal, sagittal and axial projections, T1 mode V.I. A giant aneurysm sac is visualized, roughly compressing the brain stem; d — SCT angiography, the white arrow indicates the filling part of the aneurysm; d — stage of the operation to remove thrombotic masses from the aneurysm cavity. Intraoperative photo. AA—aneurysm sac, Cer—cerebellum; e — SCT of the brain after surgery, there is a significant decrease in the size of the aneurysmal sac with a decrease in trunk compression.
Long-term results were monitored in 5 patients from 3 to 48 months after surgery. In 4 patients there was almost complete regression of existing symptoms. According to control cerebral angiography, the aneurysm does not fill in 4 patients, and slight filling remains in 1 patient. All patients also underwent a control MRI of the brain, according to which a decrease in aneurysm size was noted in 3, and no change in size in 2.
Rehabilitation after surgical treatment of an aneurysm
The rehabilitation period takes place under the supervision of specialists. Professionals do everything necessary to prevent the occurrence of postoperative complications. The patient remains in the intensive care unit for several days under the constant supervision of specialists. Afterwards, the patient is transferred to a general ward, where strict bed rest must be observed for some time. The return to a normal lifestyle occurs gradually.
If the patient's well-being worsens after surgery, transcranial Doppler ultrasound may be prescribed. Rehabilitation is aimed primarily at preventing vasospasm and increased blood pressure. Specialists also monitor the general condition of the cardiovascular system and, if necessary, prescribe osmodiuretics to eliminate swelling of the brain tissue. Additionally, anti-inflammatory therapy is carried out.
Rehabilitation after surgical treatment of an aneurysm necessarily includes a program to restore impaired body functions and further socialize the patient. The recovery period lasts at least 6 months. With the help of high-quality rehabilitation, it is possible, among other things, to eliminate the adverse consequences of surgical treatment.
Rehabilitation measures include physiotherapy, massage, and the implementation of an individually selected rehabilitation program. After endoscopic clipping, the patient can return to normal life within a few weeks.
Treatment of patients in the acute period of the disease
| Comparison of brain appearance in the acute and cold periods after SAH |
Treatment of patients in the acute period after SAH is a complex task that requires the involvement of various specialists. The rationale for operations in the acute period is, first of all, the possibility of repeated hemorrhages, which are accompanied by extremely high mortality. After switching off the aneurysm, it is also possible to begin intensive vascular therapy aimed at eliminating the consequences of hemorrhage. Based on an analysis of the results of surgical treatment of more than 600 patients in the acute period of SAH at the institute, it was shown that prognostically significant criteria for assessing the outcome of the operation are the massiveness of the hemorrhage, the patient’s condition on the Hunt-Hess or WFNS scale, and the duration of surgery after SAH. Taking these factors into account, the basic principles of treating patients have been developed. Indications for surgery in the acute stage of SAH must be strictly individualized. To resolve the issue of patient management tactics, the necessary minimum is to assess the patient’s condition using the Hunt-Hess or WFNS scale, CT, angiography, TC ultrasound and determining the severity of vasospasm. Particular attention should be paid to the period after hemorrhage. The operation is indicated for patients in stages I–II according to Hunt–Hess, regardless of the period after SAH; in stages III–IV according to Hunt–Hess within a period of 14 days after SAH. In stage III–IV patients undergoing surgery on days 0–3 after SAH, it is necessary to install sensors for postoperative ICP monitoring, since these patients are characterized by the development of vasospasm and cerebral edema in the early postoperative period. In stage III–IV patients on days 4–7 after SAH, in the presence of moderate or severe vasospasm, surgery should be abstained. The duration of delay of surgery for vasospasm depends on the TC parameters of the ultrasound scan: the operation can be performed when the blood flow velocity decreases to the level corresponding to a mild spasm, or when it stabilizes at the level of a moderate spasm for several days, but not earlier than 7 days after SAH. In stage V, surgery is indicated only in the presence of large intracerebral hematomas. In these cases, surgery is most effective with the earliest interventions possible. In the acute period of SAH, endovascular exclusion of the aneurysm should be considered the method of choice, especially in severely ill patients. In some cases, if it is impossible to completely occlude the aneurysm, you can limit yourself to partial shutdown, followed by a repeat operation after the condition improves. In addition to anatomical features, a limitation for endovascular surgery in the acute period is severe vasospasm, which prevents the insertion of a catheter. When performing direct intervention, it is necessary to take into account that the brain of a patient in the acute period of SAH is much more sensitive to surgical trauma; therefore, it is necessary to use the most gentle methods of access to the aneurysm with limited traction of the brain, the use of relaxation methods (osmodiuresis, removal of cerebrospinal fluid) and brain protection from ischemia. Throughout the entire period of treatment of patients in the acute stage of SAH, the leading task is the prevention and treatment of complications typical for hemorrhage from an aneurysm, primarily vasospasm, cerebral edema and acute or delayed hydrocephalus. Currently, to combat these complications, the technique of intravascular administration of antispasmodics under the control of TC ultrasound, 3H-therapy under multimodal monitoring, and decompressive craniotomy are used. Over the past 10 years, postoperative mortality during direct operations in the acute period averaged 7.3%, and overall mortality - 12.4%. Among surviving patients, 80% are completely independent in daily life, and about 40% have returned to work and school. The data obtained were used to create a recommendation protocol for the management of patients in the acute period of SAH together with leading neurosurgeons in Russia. The experience of the institute allowed us to take part in several international studies on the treatment of patients in the acute stage of SAH.
Forecast for life
The prognosis of the disease depends on the location of the vascular protrusion and its size. The initial condition of the patient also has a huge impact. The mortality rate in case of rupture of a cerebral aneurysm exceeds 30-50%. Surviving patients sometimes retain the consequences of the condition in the form of movement restrictions, cognitive impairment and a significant decrease in quality of life. Mortality after recurrent hemorrhage exceeds 70%.
Therefore, it is so important to carry out surgical treatment in time, turning to a qualified neurosurgeon. The operation is postponed only if there are certain medical indications.
Successful neurosurgical operations are carried out at the Burdenko Research Institute. Patients with signs of an aneurysm or suspected aneurysm are admitted here. At the Institute of Neurosurgery, it is possible to carry out comprehensive diagnostics using the latest technology and further treatment of identified diseases.
Choosing a method to turn off an aneurysm
| Aneurysm occlusion with stent assistance |
The advantages of endovasal treatment are primarily important in patients in the acute period of hemorrhage, with aneurysms of the paraclinoid part of the ICA and the vertebrobasilar region. Until recently, the main factor determining the possibility of aneurysm occlusion using the endovascular method was considered to be the ratio of the size of the aneurysm body and its neck. It has been established that the larger the size of the aneurysm and the wider its neck, the greater the likelihood of distant recanalization after the initial total occlusion. To solve this problem, stent-assisted techniques have been developed. The essence of the stent-assisted technique in the treatment of aneurysms is to prevent displacement of the coils of the coils into the lumen of the supporting vessel. This is achieved as follows: in the first stage, a stent is installed in the vessel at the level of the aneurysm neck, and then a microcatheter is passed through the stent cell, through which microspirals are delivered. In recent years, a new category of intracranial stents has emerged, the so-called flow divert stents, which reduce blood flow in the aneurysm by directing the main blood flow through the supporting vessel. Thrombosis of the aneurysm after installation of such a stent occurs on average within 4 to 6 months after surgery. This technique is most effective for treating large and giant aneurysms. Currently, the Research Institute of Neurosurgery annually performs about 250 microsurgical and 150 endovascular operations on aneurysms in the “cold” period after SAH (21 days or more). The choice of surgical method depends, first of all, on the anatomical features of the aneurysm. The endovascular method is preferable for ICA aneurysms of the paraclinoid and infraclinoid location. For MCA bifurcation aneurysms and ACA-ASA aneurysms, direct interventions are more often performed, since the structural features of these aneurysms (predominantly wide neck, proximity of the ostia of second-order arteries, variations in the structure of the ACA, etc.) and the impossibility of using stents limit the use of the endovascular method. The decision on the method of operation is influenced by the age of the patient - in young patients direct operations, which are more radical, are preferable. Limitations for the endovascular method are pathological bends and severe atherosclerosis of the brachiocephalic arteries. If a stent-assisted operation is necessary, a history of bleeding of various etiologies should be taken into account, since stent installation requires long-term use of anticoagulants in the postoperative period. In some cases, microsurgical operations are performed as a second stage in cases where only partial occlusion of the aneurysm was achieved during endovascular intervention. The opposite situations are also possible - endovascular intervention after palliative direct surgery (strengthening the aneurysm with gauze, incomplete clipping). The results of microsurgical treatment of aneurysms in the cold period after SAH have remained quite good for many years. The risk of a new neurological deficit is slightly higher with microsurgical exclusion of the aneurysm, and the risk of death is higher with endovasal treatment.