Congenital heart defects
They are formed in utero. About 2% of children are born with various PS: from mild to severe, incompatible with life. The main reasons for their development:
- chromosomal abnormalities (Down syndrome, Patau);
- the effect of alcohol, nicotine, and drugs on the fetus;
- infection of the mother during pregnancy with rubella viruses, herpes simplex, chickenpox, cytomegalovirus, toxoplasma;
- maternal diabetes;
- exposure to radiation on a pregnant woman;
- taking certain medications during pregnancy (tetracycline, sulfonamide, antitumor antibiotics).
Acquired heart defects
They develop throughout life for the following reasons:
- rheumatism ー damage to the connective tissue by one’s own antibodies that are produced against streptococci (develops in some children after scarlet fever or streptococcal tonsillitis);
- bacterial endocarditis - inflammation of the inner lining of the heart, leading to changes in the valves;
- atherosclerosis - deposition of cholesterol plaques in the walls of blood vessels;
- degenerative changes in valves - typical for older people, caused by tissue wear;
- damage to the aorta, valve apparatus due to syphilis and autoimmune diseases.
Mitral stenosis.
II Acquired heart defects.
Heart disease is an anatomical change in the valve apparatus of the heart or the interatrial, interventricular septum and other defects.
Based on their origin, defects are divided into:
- Congenital - arise as a result of a violation of the formation of the heart and blood vessels in the embryonic period.
- Acquired - acquired changes in the heart valves, leading to dysfunction and hemodynamics; acquired defects are a complication of various diseases.
Combined defect is a combination of two defects of one valve. For example, mitral stenosis and mitral insufficiency.
Combined defect - a combination of defects of several valves, for example, mitral stenosis and aortic insufficiency.
An isolated defect is one defect of one valve, for example, mitral regurgitation.
Compensated defect - no complaints, no signs of circulatory failure.
Decompensated defect - complaints of circulatory failure of the left ventricular or right ventricular type appear.
MITRAL HEART DEFECTS.
Mitral stenosis is a narrowing of the left atrioventricular orifice, which prevents the physiological flow of blood from it into the left ventricle during systole of the left atrium.
Mitral insufficiency is the inability of the left atrioventricular valve to prevent the reverse movement of blood from the left ventricle into the left atrium during ventricular systole, that is, incomplete closure of the mitral valves.
Mitral valve prolapse (MVP) is a pathological sagging (bending) of one or both mitral valve leaflets into the left atrium during left ventricular systole.
I05.0 Mitral stenosis, rheumatic.
I05.1 Rheumatic mitral valve insufficiency
I05.2 Mitral stenosis with insufficiency
I05.8 Other diseases of the mitral valve (mitral insufficiency).
I05.9 Mitral valve disease, unspecified
EPIDEMIOLOGY and ETIOLOGY.
■ Mitral stenosis almost always occurs as a result of an acute rheumatic attack, more often in women.
On average, the latent period from the moment of rheumatic heart disease (carditis) to the development of clinical manifestations of the defect is about 20 years, so the disease manifests itself between 30 and 40 years of life.
■ Mitral insufficiency. Causes: MVP, rheumatism (30%), atherosclerosis, infective endocarditis, trauma, connective tissue diseases. In men, mitral insufficiency is more common.
■ PMK. Causes: rheumatism, infections, ischemic heart disease.
CLASSIFICATION.
- The classification of mitral stenosis by severity is based on the severity of the narrowing of the left atrioventricular orifice (mild, moderate and severe stenosis).
- The classification of mitral regurgitation by severity is determined by the volume of regurgitant blood (4 degrees of mitral regurgitation).
PATHOGENESIS
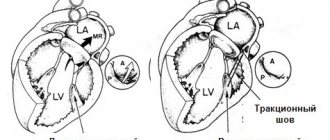
Through the narrowed left atrioventricular orifice, not all the blood during left atrium (LA) systole enters the left ventricle (LV), as a result, an excess volume of blood is formed in the left atrium (remaining after systole and re-entered from the pulmonary veins during subsequent diastole) , this leads to hypertrophy of the left atrium (compensation stage), over time, the atrial myocardium is depleted, the cavity of the left atrium expands, decompensation develops, as a result, the pressure in the ICC increases and hypertrophy of the right ventricle (RV), and then the right atrium (RA) develops.
Your opinion is important to us! Was the published material useful? Yes | No
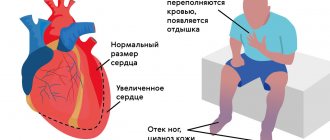
Symptoms of heart defects
Impaired hemodynamics (blood circulation) leads to a lack of blood supply to some organs and venous stagnation in others. The heart has to work harder to pump blood, it increases in size, this temporarily compensates for the pathology, symptoms do not appear. But over time, compensatory reserves are depleted, the heart muscle stretches, weakens and can no longer effectively perform its job.
This gives rise to a number of typical signs:
- shortness of breath (at the initial stages after physical activity, then at rest);
- dizziness, fainting;
- cyanosis of the nasolabial triangle, mucous membranes, fingertips;
- swelling in the legs (appears in the evening, disappears in the morning);
- symptom of “drumsticks” - club-shaped expansion of the fingertips (appears with a long course of the disease);
- rosy cheeks against a background of general pallor ー mitral face (with mitral stenosis).
If such symptoms appear, you should contact a cardiologist for further diagnosis.
I51.9 Heart disease, unspecified: description, symptoms and treatment
from 2000-2015. REGISTER OF MEDICINES OF RUSSIA ® RLS ®
Classification of acquired heart defects
(Adopted at the VI Congress of Cardiologists of Ukraine, Kyiv, 2000) Mitral stenosis:
Rheumatic 1.05.0 Non-rheumatic 1.34.2 (with clarification of etiology) Stage I - compensation Stage II - pulmonary congestion
stage - right ventricular failure
stage—dystrophic
Stage V - terminal
Mitral regurgitation
Rheumatic 1.05.1 Non-rheumatic 1.34.0 (with clarification of etiology) Stage I - compensation Stage II - subcompensation Stage III - right ventricular decompensation Stage IV - dystrophic Stage V - terminal Combined rheumatic mitral disease (Rheumatic mitral stenosis with insufficiency: 1.05.2) C predominance of stenosis: stages and indications for surgical treatment, as in mitral stenosis With predominance of insufficiency: stages and indications for surgical treatment, as in mitral regurgitation Without obvious predominance: stages and indications for surgical treatment, as in mitral regurgitation Mitral valve prolapse 1.34.1 Aortic stenosis: Rheumatic 1.06.0 Non-rheumatic 1.35.0 (with specification of etiology) Stage I - full compensation Stage II - latent heart failure Stage III - relative coronary insufficiency GU stage - severe left ventricular failure Stage V - terminal Aortic failure:
Rheumatic 1.06.1 Non-rheumatic 1.35.1 (with specification of etiology) Stage I - full compensation Stage II - latent heart failure
stage—subcompensation
stage - decompensation
Stage V—terminal Combined aortic disease:
Rheumatic aortic stenosis with insufficiency 1.06.2 Non-rheumatic aortic (valvular) stenosis with insufficiency 1.35.2 (with clarification of etiology) With predominant stenosis: stages and indications for surgical treatment correspond to those for aortic stenosis With predominant insufficiency: stages and indications for surgical treatment correspond to those for aortic insufficiency 216
Without obvious predominance: stages and indications for surgical treatment correspond to those for aortic stenosis. Tricuspid stenosis:
Rheumatic 1.07.0 Non-rheumatic 1.36.0 (with specification of etiology) Tricuspid insufficiency:
Rheumatic 1.07.1 Non-rheumatic 1.36.1 (with specification of etiology) Combined tricuspid defect:
Rheumatic tricuspid stenosis with insufficiency 1.07.2 Non-rheumatic stenosis of the tricuspid valve with insufficiency 1.36.2 (with specification of etiology) Pulmonary artery stenosis 1.37.0 Pulmonary valve insufficiency 1.37.1 Combined pulmonary valve disease (Pulmonary stenosis with valve insufficiency 1.37.2 ) Combined heart defects:
Combined damage to the mitral and aortic valves 1.08.0 Combined damage to the mitral and tricuspid valves 1.08.1 Combined damage to the aortic and tricuspid valves 1.08.2 Combined damage to the mitral, aortic and tricuspid valves 1.08.3 The severity of “simple” defects is determined by three degrees:
I degree - insignificant II degree - moderate III degree - pronounced.
The severity of the defects in accordance with their clinical and instrumental characteristics are given below for individual nosological forms of heart defects.
It should be noted that heart disease is considered “combined” when there is stenosis and insufficiency of one valve and “combined” when several valves are affected. If there are several defects, they are listed, and the defect whose severity is greater is indicated first - for example, aortic valve insufficiency, mitral valve disease with a predominance of stenosis.
Considering that valve kalydinosis determines the tactics of surgical intervention, it has been proposed to distinguish 3 degrees of kalydinosis (Knyshov G.V. BendetYa.A. 1996).
Degrees of valve calcification
+ Individual lumps of calcium in the thickness of commissures or valves
++ Significant calcification of the valves and commissures without water
attraction of the valve ring III +++ Massive calcification of the valve with transition to the fibrous ring, and sometimes to the aortic wall and ventricular myocardium. The diagnosis also needs to take into account the etiological cause of the defect (rheumatism, infective endocarditis, atherosclerosis), the degree of heart failure.
For patients who have undergone heart valve surgery, the pre-existing defect should be identified, the date of surgical treatment, and the nature of complications should be indicated. For example, operated mitral heart disease with predominant stenosis, closed commissurotomy (date) or operated aortic valve disease with predominant insufficiency. Aortic valve replacement (specify type of prosthesis and date).
Along with heart defects caused by organic changes in the valve, there are dysfunctions of the valve in the form of relative insufficiency or relative stenosis. The cause of relative valve insufficiency may be a decrease in the tone of the papillary muscles or impaired function of the circular muscles, which normally reduce the lumen of the orifice during systole. With a decrease in the tone of these muscles, the opening remains large during systole, and even unchanged valve leaflets cannot completely cover it. The most typical is relative mitral valve insufficiency in aortic disease, which gives rise to talk about “mitralization of aortic disease.” Relative insufficiency of the valves of the great vessels is observed with an increase in the perimeter of the fibrous ring, in which the area of the valve leaflets is insufficient to completely cover the mouths of the vessels (more often relative insufficiency of the pulmonary valve). Relative stenosis occurs in cases of a sharp increase in blood flow through a normally sized hole, for example, with severe regurgitation of the mitral or aortic valves. The addition of relative valve insufficiency or relative stenosis, despite changes in auscultatory signs and the course of the disease, does not provide grounds for designating the defect as combined.
Classification of heart defects
| Type | Name |
| Congenital | |
| Without the development of cyanosis (pale type) | Defects of the interventricular and interatrial septa |
| Patent ductus arteriosus | |
| Pulmonary stenosis | |
| Coarctation of the aorta | |
| With the development of cyanosis (blue) | Transposition of the great vessels |
| Common ventricle | |
| Tetralogy of Fallot | |
| Purchased | |
| Mitral valve (between the left atrium and ventricle) | Mitral stenosis |
| Mitral regurgitation | |
| Tricuspid valve (between the right atrium and ventricle) | Tricuspid valve stenosis |
| Tricuspid valve insufficiency | |
| Aortic valve (between the left ventricle and the aorta) | Aortic stenosis |
| Aortic insufficiency | |
| Pulmonary valve | Pulmonary valve stenosis |
| Pulmonary valve insufficiency | |
Stenosis
called narrowing of the valve opening, which causes difficulty in blood flow.
Insufficiency
ー inability of the valves to close tightly. In people with valve stenosis, valve insufficiency develops over time - this is called combined PS.
Coarctation of the aorta
- narrowing of the lumen of the aorta, in the area of the isthmus - the transition of the arch to the descending part.
Transposition of the great vessels
- the aorta originates from the right parts of the heart, and the pulmonary artery - from the left (it should be the other way around).
Tetralogy of Fallot
— combines four critically dangerous disorders: stenosis of the outflow tract of the right ventricle, ventricular septal defect; dextroposition of the aorta and hypertrophy (enlargement) of the right ventricular myocardium
Publications in the media
Classification of congenital heart disease by severity classes (J. Kirklin et al., 1981) • Class I. It is possible to perform a planned operation later than 6 months: VSD, ASD, radical correction for tetralogy of Fallot • Class II. Elective surgery can be performed within 3–6 months: radical correction for VSD, open atrioventricular canal (PAVC), palliative correction for TF • Class III. A planned operation can be performed within a period of up to several weeks: radical correction for transposition of the great vessels (TMS) • Class IV. Emergency surgery with a maximum preparation time of several days: radical correction for total anomalous pulmonary vein drainage (TAPD), palliative correction for TMS, VSD, OAVC • Class V. The operation is performed urgently due to cardiogenic shock: various types of defects in the decompensation stage.
Classification of congenital heart disease by prognostic groups (Fyler D., 1980) • 1 group. Relatively favorable prognosis (mortality during the first year of life does not exceed 8–11%): patent ductus arteriosus, VSD, ASD, pulmonary stenosis, etc. • Group 2. Relatively unfavorable prognosis (mortality during the first year of life is 24–36%): tetralogy of Fallot, myocardial diseases, etc. • Group 3. Poor prognosis (mortality during the first year of life is 36–52%): TMS, coarctation and stenosis of the aorta, tricuspid valve atresia, TADLV, single ventricle of the heart, OAVC, origin of the aorta and pulmonary artery from the right ventricle, etc. • Group 4. Extremely unfavorable prognosis (mortality during the first year of life is 73–97%): hypoplasia of the left ventricle, pulmonary atresia with an intact interventricular septum, common truncus arteriosus, etc.
Classification of congenital heart disease according to the possibility of radical correction (Turley K. et al., 1980) • 1 group. Defects for which only radical correction is possible: aortic stenosis, pulmonary artery stenosis, TADLV, triatrial heart, coarctation of the aorta, patent ductus arteriosus, aortopulmonary septal defect, ASD, mitral valve stenosis or insufficiency • Group 2. Defects in which the advisability of radical or palliative surgery depends on the anatomy of the defect, the age of the child and the experience of the cardiology center: various variants of TMS, pulmonary atresia, common truncus arteriosus, tetralogy of Fallot, OAVC, VSD • group 3. Defects for which only palliative operations are possible in infancy: a single ventricle of the heart, some variants of the origin of the great vessels from the right or left ventricle with pulmonary stenosis, atresia of the tricuspid valve, atresia of the mitral valve, hypoplasia of the ventricles of the heart. Abbreviations • PAVK - patent atrioventricular canal • TMS - transposition of the great vessels • TADPV - total anomalous drainage of the pulmonary veins.
ICD-10 • Q20 Congenital anomalies [malformations] of the heart chambers and connections • Q21 Congenital anomalies [malformations] of the cardiac septum • Q22 Congenital anomalies [malformations] of the pulmonary and tricuspid valves • Q23 Congenital anomalies [malformations] of the aortic and mitral valves • Q24 Other congenital anomalies [malformations] of the heart.
Heart defects in children
Congenital PS, depending on the severity, can manifest themselves in the first 3 years of a child’s life. Sometimes they are detected already in adulthood. The following signs indicate their possible presence:
- blue lips and nasolabial triangle when crying;
- the appearance of a “heart hump” - a bulge of the chest in the projection of the heart;
- shortness of breath, cough without signs of inflammatory diseases of the respiratory tract;
- delayed physical and mental development;
- the appearance of the “drumsticks” symptom.
Children with such manifestations should be shown to a pediatrician or pediatric cardiologist.
In the children's department, medical appointments are conducted by doctors who have undergone special training to identify health problems in children and infants, taking into account all age-related characteristics.