One of the common congenital heart pathologies is the bicuspid aortic valve. Epidemiology shows that this defect occurs in almost 2% of the population and is usually detected in adulthood. In most cases, the bicuspid aortic valve operates without disruption of hemodynamics and does not cause problems in the functioning of the organ, but often for this reason an aneurysm (protrusion of the wall of an artery or heart cavity) or aortic stenosis develops.
Fact! According to statistics, in 75-80% of cases of aortic valve stenosis in children, the valve is bicuspid.
Briefly about the essence of the problem
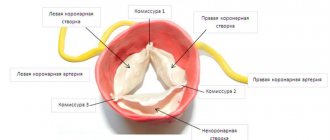
A normal valve must have three well-moving leaflets that open and close at regular intervals to ensure the outflow of blood into the aorta. The valves are shaped like crescents. There are cases when disturbances occur during the intrauterine development of the fetus, which lead to fusion of two of the three valves and the appearance of a congenital heart defect (CHD) called a bicuspid aortic valve.
The formation of the cardiovascular system occurs in the period from the sixth to the eighth week, this is the most dangerous period, because negative factors can lead to disruption of the formation of various organ elements and blood vessels. That is why doctors strongly recommend that pregnant women in the first trimester be especially attentive to their health, give up all bad habits and avoid stress.
Pathological changes in damage to the aortic valves
The result of congenital and acquired changes is the formation of insufficient closure of the valves, this is expressed in the return of part of the blood to the cavity of the left ventricle when it relaxes. The cavity expands and lengthens in size.
Forced intensification of contractions causes, over time, a breakdown of compensatory mechanisms and hypertrophy of the muscular layer of the left ventricle. This is followed by dilation of the left venous opening connecting the ventricle to the atrium. Overload from the left sections is transmitted through the pulmonary vessels to the right heart.
The impaired ability of the valve leaflets to close tightly leads to the formation of insufficiency and prolapse under the influence of reverse blood flow. Usually, aortic stenosis occurs simultaneously. In the clinical picture we can talk about the predominance of one type of defect. Both increase the load on the left ventricle of the heart. Features of the course must be taken into account when choosing a treatment method.
Signs of a cardiac abnormality
Very often, the defect - bicuspid aortic valve in children - occurs without symptoms, it is not suspected for decades, but the older a person gets, they more often show signs of an anomaly.
Typical symptoms include the following:
- the appearance of shortness of breath, which increases significantly after physical exertion. Over time, shortness of breath begins to appear even with light exertion;
- strong pulsation in the head;
- frequent tachycardia (many patients mistake it for palpitations);
- pain in the cardiac region (they are the result of ventricular hypertrophy).
A special symptom that characterizes a congenital heart defect called bicuspid aortic valve is a violation of blood flow in which reverse movement occurs, i.e. blood leaves the aorta back into the ventricle. This manifestation of a defect in a patient can only be identified by a specialist conducting an examination, but it is for this reason that other signs appear.
Medical Internet conferences
Introduction
Bicuspid aortic valve is the most common congenital heart defect. Remaining asymptomatic for a long time, it may eventually become complicated by the development of aortic stenosis or aortic insufficiency. Bicuspid aortic valve is also associated with aortic aneurysm and dissection. Given the high prevalence of this defect and the severity of complications, it is believed to cause more deaths than all other congenital heart defects combined [1].
Introduction
Bicuspid aortic valve is the most common congenital heart defect. Remaining asymptomatic for a long time, it may eventually become complicated by the development of aortic stenosis or aortic insufficiency. Bicuspid aortic valve is also associated with aortic aneurysm and dissection. Given the high prevalence of this defect and the severity of complications, it is believed to cause more deaths than all other congenital heart defects combined [1].
Introduction
Bicuspid aortic valve is the most common congenital heart defect. Remaining asymptomatic for a long time, it may eventually become complicated by the development of aortic stenosis or aortic insufficiency. Bicuspid aortic valve is also associated with aortic aneurysm and dissection. Given the high prevalence of this defect and the severity of complications, it is believed to cause more deaths than all other congenital heart defects combined [1].
Clinical case
Patient A., 51 years old, was admitted on March 4, 2021 with complaints of shortness of breath with difficulty inhaling and exhaling when going up to the 4th floor; dizziness when moving to a vertical body position; attacks of rapid heartbeat that occur in a lying position, lasting a few seconds, stopping on their own.
Considers himself sick for a year and a half (from the age of 49), when dizziness first began to bother him. Since March 2021, shortness of breath occurs during physical activity. Over the course of six months, an increase in blood pressure to 140 and 90 mm was repeatedly recorded. rt. Art. Since September 2021, attacks of rapid heartbeat occur occasionally at rest. An examination at a local clinic revealed a congenital heart defect: bicuspid aortic valve. Sent to the cardiology hospital.
From the life history it is known that the patient served in the army, coped well with physical activity, currently works as a mechanic at a factory, and previously smoked. As a child I had frequent sore throats. Among the operations undergone, he noted a tonsillectomy at the age of 12 years.
Upon examination, an asthenic physique attracted attention. On palpation, a high, intense, resistant, dome-shaped apical impulse was detected in the 5th intercostal space 1 cm outward from the left midclavicular line. During percussion, the left border of relative cardiac dullness was shifted to the left and coincided with the apical impulse. On auscultation, heart sounds were rhythmic, heart rate 72 per minute. At the top, the first tone was slightly weakened, but louder than the second tone. Above the aorta, the second sound was weakened, a rough systolic murmur was heard, carried through to the vessels of the neck and the entire precordial region. Blood pressure was 140 and 80 mm Hg. The radial artery pulse was the same in both arms, rhythmic with a frequency of 72 per minute.
There were no changes in general and biochemical blood tests as of 03/05/2019.
During electrocardiography on March 4, 2021 (Fig. 1), sinus rhythm was recorded with a frequency of 72 per minute. The electrical axis of the heart was located horizontally. Signs of left atrium enlargement were determined.
Holter ECG monitoring dated March 11, 2021, which lasted for 23 hours, showed the dominant rhythm was sinus. The average heart rate was 54 per minute. A paroxysm of ventricular tachycardia consisting of 5 contractions with a frequency of 129 per minute, 24 single ventricular extrasystoles was recorded. Supraventricular ectopic activity consisted of 288 contractions, of which 12 atrial groups lasting from 3 to 8 contractions with a frequency of 105 to 129 per minute, 12 episodes of paired atrial extrasystoles, including with aberration of intraventricular conduction, 201 single atrial extrasystoles. There were no diagnostically significant dynamics of the ST segment.
X-rays of the chest organs with a contrast-enhanced esophagus dated March 5, 2021 (Fig. 2) revealed signs of dilation of the ascending aorta, a slight enlargement of the left ventricle, and right-sided scoliosis of the thoracic spine.
Echocardiography on March 5, 2021 (Fig. 3) visualized a bicuspid aortic valve and multiple calcifications at the base and distal parts of the leaflets. Slight aortic regurgitation was detected; aortic stenosis, the degree of obstruction is severe, the maximum gradient is 79 mm Hg, the average gradient is 46-50 mm Hg, slight expansion of the aortic root (diameter 4.2 cm). There was a pronounced expansion of the ascending aorta (diameter 4.6-4.8 cm), slight pulmonary hypertension: systolic pulmonary artery pressure 36 mm Hg. Slight left ventricular hypertrophy was determined: myocardial mass index 107 g/m², slight enlargement of the left atrium (end-systolic volume 74 ml). The left ventricular ejection fraction was 66%. A pseudonormal type of transmitral blood flow was recorded.
Coronary angiography on March 6, 2021 revealed stenosis of the right coronary artery in the second segment up to 80%.
The patient was diagnosed:
Congenital heart defect: bicuspid aortic valve. Combined aortic disease: aortic stenosis of III-IV degree. Aortic insufficiency degree I. Arterial hypertension stage III risk 4.
Complications: Chronic heart failure stage IIa, functional class 2.
Treatment was prescribed: acecardol 100 mg once a day in the evening, cozaar 50 mg once a day in the morning, bisoprol 2.5 mg once a day in the evening.
A council of cardiac surgeons recommended aortic valve replacement for the patient.
Discussion
The incidence of bicuspid aortic valve ranges from 0.6% to 2% [1]. The disease occurs 3 times more often in men than in women.
The frequency of detection of pathology in first-degree relatives of a patient is 9% [2]. In recent years, views on this pathology have changed significantly, and today, when talking about this defect, they mean valvulo- and aortopathy of hereditary origin, caused by molecular and histological changes in the connective tissue [3]. The genetic mechanisms leading to the formation of a bicuspid aortic valve are not well understood. Currently, NOTCH1 remains the only confirmed candidate gene whose mutation is associated with both familial and sporadic cases of bicuspid aortic valve with concomitant thoracic aortic aneurysm [4].
The clinical picture in patients with a bicuspid aortic valve can vary from severe manifestations of valve dysfunction in infancy to their complete absence in older people [1]. In the presence of aortic stenosis or aortic insufficiency, patients are bothered by headaches, fainting, and dizziness, as in our patient. Clinical manifestations may also be caused by dilation of the ascending aorta (aortopathy), coarctation of the aorta, and the development of infective endocarditis [2].
Signs of a bicuspid aortic valve can be detected by auscultation. In patients with a normally functioning bicuspid aortic valve, a systolic ejection murmur is heard at the apex of the heart and in the projection of the aorta. In children predominantly 7-11 years old, aortic systolic clicks can be detected in the 2nd intercostal space to the right of the sternum [5]. With aortic regurgitation, a diastolic murmur is heard above the aorta and at Botkin's point, and in the presence of aortic stenosis (as in our patient), a rough systolic murmur is heard above the aorta, conducted to the vessels of the neck.
The electrocardiogram is usually normal, but there may be signs of left ventricular hypertrophy. The mainstay of diagnosis is echocardiography [6].
Currently, the following types of surgical interventions can be performed in children with a bicuspid aortic valve due to its stenosis: balloon valvuloplasty, valve replacement with mechanical and biological prostheses, Ross operation and reconstructive plastic surgery on the aortic valve [7].
According to Petrushenko D. Yu. and co-authors, satisfactory results of treatment of critical aortic stenosis in newborns and children in the first months of life were reported both when performing balloon valvuloplasty and open reconstructive plastic surgery on the valve. Both procedures are palliative: sooner or later the patient will again need surgical treatment, since after balloon valvuloplasty valve insufficiency develops, and after open repair there is a risk of developing restenosis [7]. Aortic valve replacement is performed in children and adolescents in whom previous balloon valvuloplasty has resulted in aortic insufficiency. The operation is performed during the period when the growth of the aorta is completed [5]. Surgical treatment of bicuspid aortic heart disease in adults in tactical terms does not cause much discussion: unlike children, the issue of tactics and surgical techniques is much simpler to solve - the vast majority of patients require aortic valve replacement [3]. Patients with large aortas have a significant risk of mortality within 5 years due to aortic dissection or rupture, especially when the aortic diameter reaches 6 cm [8]. In case of bicuspid aortic valve, surgery on the ascending aorta is indicated in the case of: enlargement of the root or ascending aorta >55 mm; enlargement of the root or ascending aorta >50 mm and the presence of other risk factors; enlargement of the root or ascending aorta >45 mm during planned aortic valve replacement surgery. With planned replacement of the ascending aorta (including the aortic root), surgical mortality ranges from 1.6-4.8% [9].
It is known that in patients with Marfan syndrome, β-blockers and/or losartan can slow down the dilatation of the aortic root and reduce the risk of aortic complications. By analogy, it is common clinical practice to recommend these drugs to patients with a bicuspid aortic valve and enlargement of the root or ascending aorta [10]. Therefore, our patient was prescribed bisoprolol and cozaar.
In the presence of a bicuspid aortic valve, as with other heart defects, when performing invasive medical interventions accompanied by bacteremia, it is necessary to prescribe antibiotics to prevent infective endocarditis.
The prognosis for bicuspid aortic valve is generally favorable. However, more than half of all patients in the world who require aortic valve replacement are patients with this heart defect [5]. According to Pelekh D.M., who analyzed the outcomes of surgical treatment of patients with aortic stenosis, including patients with bicuspid valvulopathy, aortic valve replacement leads to good immediate and long-term results: a decrease in the size of the left chambers of the heart, a decrease in the severity of myocardial hypertrophy, and an improvement in myocardial contractility left ventricle and, consequently, the well-being of patients. Most patients progress to NYHA functional class 1–2. After surgery, acute cerebrovascular accidents, prosthesis thrombosis, and infective endocarditis may develop. Mortality in the early postoperative period ranges from 9.3 to 12.3% [11].
Conclusion
Bicuspid aortic valve is a common heart defect, the presence of which predisposes to severe complications. The disease may not appear clinically for a long time. To prevent the development of complications, it is necessary to timely identify this heart defect and carefully monitor the patient to timely determine indications for surgical treatment.
Causes of the phenomenon
As the main reason for the development of this defect, doctors call the impact of harmful and dangerous factors on the body of a pregnant woman during the formation of elements of the cardiovascular system. This may be radiation exposure, x-ray exposure, infection, poor ecology and other mutagens.
The next factor is a woman’s smoking during pregnancy. Nicotine has a negative effect on the formation of any organs during fetal development.
It affects the development of the bicuspid aortic valve and heredity, it is transmitted from one of the parents. Therefore, doctors strongly recommend that those parents who have this anomaly conduct a full examination of the child immediately after birth in order to take the necessary measures and carry out therapy in a timely manner.
Treatment Options
The severity of the symptoms of the disease entirely determines the treatment tactics. If before the examination the patient did not have any health problems, the body was subjected to intense physical activity, no specific therapy is required. However, after confirming the diagnosis, the doctor must register him with a dispensary, which obliges him to take a series of tests several times a year.
A different approach is required by a severe form of pathology. The patient is indicated for surgery with installation of an aortic valve prosthesis. Surgical intervention does not involve open manipulation of the chest. Modern techniques allow the installation of a prosthesis through the skin. The implant is inserted through the subclavian or femoral artery. After the operation, the patient is prescribed constant medication to reduce blood clotting.
Diagnostic examination methods
If any signs indicating problems with the heart appear, an examination by a cardiologist is immediately required. In addition to collecting anamnesis, the doctor prescribes the necessary types of hardware diagnostics.
The very first method that will reveal the presence of congenital heart disease in the form of a bicuspid aortic valve is echocardiography (a type of ultrasound (you can watch it on video), which allows you to identify not only the presence of an anomaly, but also the degree of regurgitation).
In addition, diagnostics may include:
- radiography;
- electrocardiogram;
- Doppler study;
- cardiac catheterization.
How does valvular insufficiency manifest?
Symptoms of incomplete closure of the aortic valve begin to appear if the reverse flow of ejected blood reaches 15–30% of the volume of the ventricular cavity. Before this, people feel good, even play sports. Patients complain about:
- heartbeat;
- headaches with dizziness;
- moderate shortness of breath;
- feeling of pulsation of blood vessels in the body;
- angina pain in the heart area;
- tendency to faint.
With decompensation of the cardiac adaptation mechanisms, the following appears:
- dyspnea;
- swelling in the limbs;
- heaviness in the hypochondrium on the right (due to stagnation of blood in the liver).
During the examination, the doctor notes:
- pale skin (reflex spasm of peripheral small capillaries);
- pronounced pulsation of the cervical arteries and tongue;
- change in pupil diameter in accordance with the pulse;
- In children and adolescents, the chest protrudes due to strong heartbeats into the non-ossified sternum and ribs.
Intensified beats are felt by the doctor when palpating the heart area. Auscultation reveals a typical systolic murmur.
Blood pressure measurement shows an increase in the upper number and a decrease in the lower one, for example, 160/50 mmHg. Art.
Treatment of diseases
If a bicuspid aortic valve is detected with grade 1 insufficiency, and it does not show any signs and does not affect the patient’s quality of life, does not interfere with physical activity, then the defect can be left for some time without surgical intervention. However, the patient must undergo periodic examinations, ultrasound scans and avoid overloading the heart. However, with age, surgery will still be indicated.
A bicuspid aortic valve requires surgical intervention, which involves:
- prosthetics (replacement with a biological or mechanical prosthesis);
- transcatheter implantation of valve prosthesis (modern method of percutaneous implantation).
Diagnosis of disorders
If you have any complaints, you should definitely consult a doctor. He may suspect the presence of pathology by conducting a physical examination, if there are any murmurs, additional sounds, or changes in the size of the heart.
Diagnosis of the bicuspid aortic valve is usually not difficult, since one of the popular and accessible research methods is ultrasound scanning. Echocardioscopy allows not only to determine the anatomical structure of the organ, but also the degree of dysfunction.
In modern clinics it is possible to conduct transesophageal cardiography. This is a study where a special sensor is inserted through the mouth into the esophagus using a special probe. This makes it possible to more accurately visualize the valve apparatus and measure the volume of blood ejected by the heart.
It is also possible to indirectly confirm the presence of pathology and its complications using a chest x-ray with contrast. If there are contraindications to radiation, magnetic resonance imaging may be performed.
The degree of functional impairment can be assessed using an exercise tolerance test, during which an electrocardiogram is recorded.
Patient prognosis and recommendations
Now, about how long the patient will live after he is diagnosed with “Bivalve aortic valve”, the prognosis will depend on the rate of changes in the functioning of the organ caused by the presence of the defect, and on whether there is a manifestation of heart or coronary insufficiency.
If no serious destructive problems are found, then ten years may pass from the moment of diagnosis, but if destruction occurs and the presence of a defect affects the functioning of the organ, then the forecasts do not exceed two years.
Attention! This defect requires constant monitoring and observation by specialists, and clinical manifestations indicate the need for immediate treatment in a specialized clinic.
Even if the functional bicuspid valve does not affect the rhythm of life, doctors recommend avoiding nervous strain, trying to avoid stress, maintaining a work-rest schedule, eating more vitamins (in the form of vegetables and fruits) and be sure to take daily walks in the fresh air. Prevention should be aimed at protecting against infections such as endocarditis, and it also helps against sclerosis.
As for the question: bicuspid aortic valve and sports, it should be resolved individually in consultation with a doctor.
How is the disease treated?
The only effective method of combating pathology is surgery. It is aimed at installing an artificial valve. But first, the feasibility of its implementation will be considered. For example, if a person is diagnosed with BAV without hemodynamic disturbances, he is not bothered by any symptoms, and he can easily tolerate normal physical activity, then there is no need to perform surgery. In this case, the doctor will recommend observation by a cardiologist and systematic ultrasound examination.
If the doctor identifies an anomaly, then it is necessary to decide whether valve replacement surgery is required.
In situations where there really is a threat to the patient’s health, the question of surgical intervention and valve replacement will be very relevant. It should be noted that thanks to the wide capabilities of modern medicine, operations are highly successful. They can be carried out in several ways. Everything will depend on the patient’s health condition. The survival rate after prosthetics is quite high, so there is no doubt about the effectiveness of surgical treatment.
Bicuspid aortic valve and sports
Some patients are concerned about the compatibility of this disease and sports. Doctors cannot give a definite answer, because everything depends on the degree of damage and the severity of the pathological process. Of course, there is no place for patients with such a diagnosis in professional sports. Excessive physical activity can worsen the course of the disease and lead to irreversible consequences. Given the hereditary nature of the disease, it can be diagnosed at the age of 10-15 years. Therefore, parents, knowing about such a diagnosis, should periodically take their child for examination. Deviations in the functioning of the cardiac system are a contraindication to sports. In this case, it is better to opt for the least traumatic options (yoga, Pilates). In any case, you should consult your doctor and do not ignore his recommendations.