Atrial fibrillation - causes, symptoms and treatment
Atrial fibrillation is manifested by scattered, chaotic contraction of the muscle tissue (myocardium) of the atria, at a speed of 350-600 pulse waves per minute. As a result, the atria do not contract fully, and the presence of blood in the ventricles weakens. Some blood is retained in the atria, which increases the risk of blood clots.
The presence of an outbreak of atrial fibrillation for more than 48 hours leads to a high risk of developing ischemic stroke, myocardial infarction, thromboembolism of various organs and peripheral vessels, and severe cardiovascular failure.
What it is?
Atrial fibrillation is translated from Latin as “madness of the heart.” The term “atrial fibrillation” is a synonym, and the definition of the disease is as follows: atrial fibrillation is a type of supraventricular tachycardia, characterized by chaotic activity of the atria with their contraction at a frequency of 350-700 per minute.
This heart rhythm disorder is quite common and can occur at any age - in children, the elderly, middle-aged and young men and women. Up to 30% of cases of need for emergency care and hospitalization for rhythm disturbances are associated precisely with the consequences of atrial fibrillation. With age, the frequency of the disease increases: if up to 60 years of age it is observed in 1% of patients, then later the disease is registered in 6-10% of people.
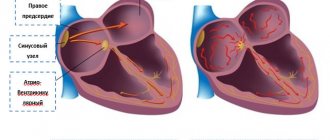
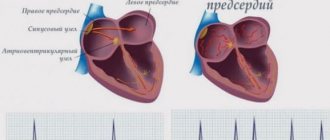
With atrial fibrillation, contraction of the atria occurs in the form of their twitching, the atria seem to flutter, flickering ripples run through them, while individual groups of fibers work uncoordinated in relation to each other. The disease leads to a natural disruption of the activity of the right and left ventricles, which cannot throw a sufficient amount of blood into the aorta. Therefore, with atrial fibrillation, the patient often exhibits a pulse deficiency in large vessels and irregular heart rate. The final diagnosis can be made by ECG, which reflects the pathological electrical activity of the atria, and also reveals the random, inadequate nature of cardiac cycles.
The best beta blockers for arrhythmia
Thanks to such means, it is possible to reduce the need of the heart muscle for oxygen supply, as well as stop the functions of catecholamines. Cardiologists prescribe this group of medications to patients with sinus-type disease or caused by insufficient blood microcirculation. The list of beta blocker drugs for cardiac arrhythmia included 2 leaders according to reviews and assessments by cardiologists.
Metoprolol
The first in this category is a drug for normalizing cardiac activity. In terms of composition, it is a beta1-blocker with a wide spectrum of effects, but of a selective type. Another difference from analogues is the prolonged effect. The active substance is metoprolol succinate, which has antiarrhythmic, antihypertensive, and antianginal effects.
That is, proper use of tablets reduces blood pressure, prevents it from jumping, and prevents heart rhythm disturbances and angina attacks. The therapy also helps slow the pulse, muscle contractility, reduce the volume of ejected blood and myocardial excitability. The effect develops gradually, reaching a maximum after 2 weeks of the course.
Advantages:
- Large list of indications;
- Selective action;
- Possibility of use for prophylactic purposes;
- Bioavailability;
- Prolonged effect;
- Decreased heart rate and blood pressure.
Flaws:
- Withdrawal syndrome;
- Risks of side effects.
The standard treatment regimen is 100 mg in one or two doses per day, gradually increasing the dose to 200-400 mg. The product is not recommended for low blood pressure, heart failure, impaired peripheral blood supply, or lactation.
Anaprilin
Tablets for arrhythmia of non-selective action, designed to normalize heart rhythm by influencing blood pressure, the sympathetic nervous system, and pulse. The active substance is propranolol hydrochloride, which reduces the frequency of muscle contractions and blood pressure. The list of indications also includes tachycardia, angina pectoris, extrasystole, and hypertension.
The tablet form can be of 3 types depending on the concentration of the active substance - 10, 50, 100 mg. Medical practice shows that the correct use of Anaprilin has a beneficial effect on the myocardium, eliminates dizziness, shortness of breath, and discomfort in the chest area. Improvement occurs within 30 minutes, even faster if administered by injection.
Advantages:
- Calm, lower blood pressure;
- Quick relief;
- Help with VSD, panic attacks;
- “First aid” for rhythm disturbances;
- Availability;
- Inexpensive.
Flaws:
- Lots of side effects;
- Specific taste.
Treatment in this way is unacceptable for acidosis, acute infarction, peripheral circulatory disorders, bronchospasms, and sinus bradycardia. Otherwise, start with 20 mg three times a day with a gradual increase in dose. For better digestibility, this should be done half an hour before meals.
Causes
Various acute and chronic conditions can provoke heart rhythm disturbances such as atrial fibrillation.
Acute causes are:
- exposure to temperature factors – hyper- or hypothermia;
- operations;
- myocardial infarction;
- excessive consumption of caffeine, alcohol, nicotine;
- inflammatory heart diseases – pericarditis, myocarditis;
- taking drugs with arrhythmogenic effects;
- mechanical effects on the body - injuries, vibration;
- some other types of arrhythmias (WPW syndrome).
The impact of the factors mentioned above on a healthy heart will most likely not provoke atrial fibrillation - its occurrence is facilitated by structural and metabolic changes in the myocardium, as well as some types of non-cardiac pathology:
- cardiomyopathy;
- heart tumors;
- constrictive pericarditis;
- endocrine pathology, in particular;
- cardiac ischemia;
- acquired and some congenital heart defects;
- arterial hypertension;
- thyrotoxicosis;
- diseases of the gastrointestinal tract (calculous cholecystitis, diaphragmatic hernia);
- pathology of the central nervous system;
- intoxication.
Symptoms of atrial fibrillation
It should be remembered that in 20-30% of cases, atrial fibrillation occurs without symptoms, without causing any sensations. The discovery of this form usually occurs by accident.
The main complaints of patients with atrial fibrillation include:
- the main complaint is sudden attacks of rapid irregular heartbeat or a feeling of constant irregular heartbeat, pulsation of the veins in the neck;
- squeezing pain in the heart area like angina pectoris;
- general weakness, increased fatigue;
- difficulty breathing (shortness of breath), especially during physical activity;
- dizziness, unsteadiness of gait;
- fainting states, fainting;
- increased sweating;
- rarely, an increase in urine (polyuria) with the release of natriuretic hormone.
With the development of a permanent form of the disease, patients cease to feel discomfort or interruptions in the functioning of the heart and adapt to living with this disease.
Why do you need to control your lifestyle?
Because it affects the size of the left atrium. The more severe the obesity, the larger the size of the left atrium. If a person is overweight, the pressure in the heart increases, the volume of circulating blood increases, and the left atrium stretches. The larger the left atrium is from normal (400 mm), the higher the risk of developing atrial fibrillation.
Situations
With normal left atrium size, the effectiveness of radiofrequency ablation can reach 70%. The larger the size of the left atrium, the lower the effectiveness of RFA.
● If a patient is undergoing radiofrequency ablation, it is important to remember: the more abnormal the atrial function is, the higher the risk of recurrent atrial fibrillation. ● When a person’s heart rhythm is lost, during an ultrasound they pay attention to the size of the left atrium: if it is slightly dilated, it makes sense to try to restore this rhythm using medications or electrical pulse therapy. But if the left atrium is significantly dilated, there is no particular point in restoring the rhythm - sooner or later it will break down again.
What to do?
● Control your weight. ● Avoid alcohol - alcohol increases the risk of bleeding and aggravates the course of the arrhythmia or increases the frequency of breakdowns of this arrhythmia. ● Stop smoking. ● Stop taking dietary supplements - most of them can enhance the effect of anticoagulants. ● Increase physical activity. ● Monitor the condition of the thyroid gland by an endocrinologist.
Complications
The most dangerous complications of MA:
- The development of thromboembolism due to thrombus formation in the chambers of the heart.
- Heart failure.
- The onset of sudden death due to cardiac arrest caused by blockage of its internal orifices.
- The development of cardioembolic stroke, which occurs due to stagnation of blood in the atria.
- Cardiogenic shock, which provokes a significant decrease in blood pressure, as a result of which the organs and tissues of the human body cease to receive the necessary nutrition, and irreversible processes begin in them.
- The formation of blood clots, which can travel through the bloodstream to any organ, including the brain, causing the death of brain tissue (stroke).
Atrial fibrillation seems to be a simple disease only at first glance. Patients with this diagnosis should remember that atrial fibrillation is a pathology, the danger of which is associated with complications that arise as a result of the lack of timely adequate treatment or the transition of the disease to a chronic form.
These include:
1. Rhythm control/pulse rate control
If rhythm disturbances occur more than once or twice a year, constant use of antiarrhythmic drugs is necessary.
Tactics to actively restore and maintain normal (sinus) rhythm using AAP are called rhythm control tactics. It is preferable in those patients with paroxysmal, permanent and persistent forms of the disease who lead an active lifestyle and do not have solid concomitant pathology. With fairly frequent, prolonged episodes of AF, ongoing planned antiarrhythmic therapy is also mandatory. Often, an increase in paroxysms is a natural course of the disease. But in some cases, this form of MA is caused by improper treatment, when the patient takes medications in insufficient doses or is not treated at all. It is the arrhythmologist who is called upon to select the treatment regimen that will help the patient cope with the disease. If it is unsuccessful, the patient may be recommended to consult a cardiac surgeon - arrhythmologist for surgical treatment of AF.
If this arrhythmia becomes permanent, active rhythm restoration is not indicated due to ineffectiveness. Under the influence of a long-term arrhythmia, the structure and function of the heart change and it “gets used” to living with it; it is no longer possible. In such patients, pulse control tactics are used, that is, with the help of medications, a heart rate that is comfortable for the patient is achieved. But no active attempts are made to restore the rhythm.
The following are currently used as antiarrhythmic drugs:
- beta blockers (metoprolol, bisoprolol, carvedilol)
- propafenone
- amiodarone
- sotahexal
- allapinin
- digoxin
- drug combination
2.Prevention of complications:
prevention of stroke and thromboembolism
With AF, there is no single, coordinated ejection of blood from the heart; some of the blood stagnates in its chambers and, in the form of blood clots, can enter the vessels. Most often, the blood vessels of the brain are affected and a stroke develops.
In order to prevent it, drugs that affect blood clotting are prescribed - warfarin, rivaroxaban, dabigatran, apixaban, which reliably (more than 90%) protect against stroke.
While taking these drugs, the patient should monitor for bleeding and monitor the complete blood count and creatinine quarterly. (when taking rivaroxaban, dabigatran and apixaban)., or test the INR (international normalized ratio) at least once a month when taking warfarin. This is necessary in order to correctly calculate the dose of the drug and monitor its safety.
Acetylsalicylic acid (aspirin, cardiomagnyl, thromboass) is not routinely used for the prevention of thromboembolism, since the degree of protection against venous thrombosis when used is only 25%.
prevention of heart failure
Heart failure (HF)
– a complication of many heart diseases, including AF. This condition is caused by the lack of full pumping function of the heart, as a result of which the liquid part of the blood stagnates in the tissues and organs, which is manifested by shortness of breath and edema.
For the prevention and treatment of heart failure, ACE inhibitors (enalapril, lisinopril, perindopril, etc.), veroshpiron (eplerenone), and diuretics (torasemide, furosemide, hypothiazide) are used.
3. Surgical treatment is used if there is no effect from medications and is carried out in specialized cardiac surgery clinics.
Types of surgical treatment of MA:
- implantation of a pacemaker for bradyform MA
- radiofrequency ablation of the pulmonary veins and other arrhythmogenic areas
- with paroxysmal tachyform of atrial fibrillation and flutter
Surgery for arrhythmias in general and AF in particular is the “last cartridge” used when drug therapy is unsuccessful.
After surgical treatment, in order to prevent recurrence of arrhythmia, patients are prescribed planned antiarrhythmic therapy.
Thus, treatment of atrial fibrillation is a way of life that involves the patient “working on himself.” And an arrhythmologist helps him with this.
A patient with MA should avoid colds, lead a healthy lifestyle, get rid of bad habits and avoid factors leading to its development, and strictly follow all the recommendations of his doctor. The doctor will help you choose an individual treatment regimen and recommend what to do if a recurrence of arrhythmia develops, and will also promptly refer you to a cardiac surgeon - arrhythmologist, if indicated.
It is important to understand that the selection of antiarrhythmic therapy takes some time, requires repeated examinations by a doctor and a number of dynamic studies (general clinical tests, study of thyroid hormone levels, cardiac ultrasound and Holter ECG monitoring, electrocardiogram registration) and this should be treated with understanding. In some cases, it is necessary to replace one drug with another.
Living with atrial fibrillation is not an easy process and it is very important that the patient feels supported and helped by the doctor. We are happy to help you with this and are ready to offer follow-up programs for a cardiologist, arrhythmologist and cardiac surgeon in our clinic.
Diagnostics
Atrial fibrillation is diagnosed based on:
- collection and analysis of anamnesis;
- detection of characteristic complaints of the patient himself;
- detection of certain specific changes in standard electrocardiogram recordings.
Electrocardiographic signs of the pathology in question are as follows:
- Multiple f waves are detected, confirming atrial fibrillation (flickering). This type of wave may differ in amplitude, shape and other characteristics;
- the recordings completely lack P waves, which are necessarily detected in normal sinus heart rhythm;
- while the QRS complexes are preserved, a chaotic violation of the RR intervals is observed.
In addition, when performing standard electrocardiography, doctors have the opportunity to determine the patient’s associated cardiac pathology that provokes rhythm disorders. Also, to establish an accurate diagnosis and detect all concomitant pathologies, doctors can use diagnostic techniques such as Holter monitoring, echocardiography, cardiac ultrasound, etc.
An example of paroxysmal atrial fibrillation on an ECG
How to choose a drug for arrhythmia
It is impossible to choose medications for the treatment of abnormal heart rhythms on your own. To avoid harm to your health, consult your doctor. What to buy at the pharmacy largely depends on the form of arrhythmia determined by the cardiologist and concomitant pathologies. There are also a number of other factors in individual development of a treatment regimen.
The doctor's consultation
The list of medications and the regimen for taking them is prescribed only by a specialist, a cardiologist. We are talking about a whole group of antiarrhythmic drugs, which are selected only after diagnosis. If you do not solve the problem comprehensively, there is a high probability of relapses and complications. Self-medication, incorrect choice of dosages, all this threatens with serious side effects.
Form of arrhythmia
The choice of medications depends on what form of heart rhythm disturbance the doctor has diagnosed. The generally accepted classification considers nootropic, heterotropic form, atrioventricular block, changes/disturbances in excitability, conductivity or excitatory function. The type of pathology depends on the reasons that provoke it. Each case is individual, as is the treatment plan.
Presence of other diseases
Since we are talking about a disease of the cardiovascular system, there is a high probability of developing associated disorders. Medical practice considers sinus bradycardia or tachycardia, atrial fibrillation or flutter, reciprocal AV nodal or ventricular tachycardia, atrial/ventricular extrasystole. Depending on this, auxiliary means are selected.
Other selection factors
There are a number of minor factors that determine which agents are appropriate in treatment. The first is the severity of the pathology. The specialist also takes into account the patient’s age, for example, drugs for arrhythmia for older people should not affect blood pressure. Take into account the contraindications in the instructions so as not to encounter side effects.
Treatment of atrial fibrillation
Today, several treatment methods are used for atrial fibrillation, aimed at restoring an adequate heart rhythm and preventing new attacks. Medicines and electrical cardioversion are used. If the effectiveness of these methods is weak, surgical treatment methods are used - catheter ablation or implantation of a pacemaker. An integrated approach to therapy helps prevent new attacks.
The following drugs are used for atrial fibrillation:
- Blood thinners - antiplatelet agents - prevent the formation of blood clots.
- Beta blockers (betaxolol, carvedilol, nebivalol, metoprolol, pindolol, propraolol, celiprolol, esmolol) and calcium blockers (verapamil, diltiazem) - they slow down the heart rate. These medications for atrial fibrillation prevent the ventricles from contracting too quickly, but do not regulate the heart rhythm.
- For antiplatelet therapy, anticoagulants are prescribed that do not prevent the formation of blood clots, but reduce the risk of this, and, consequently, the occurrence of strokes (heparin, fondaparinux, enoxaparin).
- Also, when atrial fibrillation is diagnosed, medications are used that prevent the formation of blood clots and strokes (warfarin, Pradaxa).
- Antiarrhythmic drugs (amiodarone, dronedarone, ibutilide, procainamide, propafenone, sotalol, flecainide).
Regular blood tests are required to monitor the effects of medications. Only a doctor can choose the right pills for atrial fibrillation, since many of them have serious contraindications, as well as proarrhythmic activity, when taking the drug itself can unexpectedly provoke atrial fibrillation.
Before treating atrial fibrillation, the patient’s concomitant diseases should be taken into account. Sometimes medication is started in a hospital, where doctors can more easily monitor the body's response and heart rate. With this therapy, in 30-60% of cases the patient's condition improves, but over time the effectiveness of the drugs may decrease. In this regard, doctors often prescribe several antiarrhythmic drugs at once.
Rating of drugs for arrhythmia
When selecting appropriate medications, VyborExpert relied on the recommendations of leading cardiologists, after which effective and time-tested drugs were assessed for the following characteristics:
- Form of the disease;
- Presence of concomitant disorders;
- Patient's age;
- Composition of the drug;
- Mechanism of action;
- Presence of additional risk factors;
- Release form, ease of use;
- Contraindications, risks of side effects;
- Safety, bioavailability;
- Course duration, price.
The result of the comparative analysis was a list of drugs for arrhythmia consisting of 9 nominees. For convenience, they were divided into 5 groups according to the principle of action. These are both preventive and therapeutic agents. Thanks to customer reviews, it was possible to determine the strengths and weaknesses of each.
Treatment of permanent atrial fibrillation
In this form, the patient is prescribed tablets that slow down the heart rate. The main ones here are the group of beta blockers and cardiac glycosides, for example, Concor 5 mg x 1 time per day, Coronal 5 mg x 1 time per day, Egilok 25 mg x 2 times per day, Betaloc ZOK 25-50 mg x 1 time per day etc. Of the cardiac glycosides, digoxin 0.025 mg is used, 1/2 tablet x 2 times a day - 5 days, break - 2 days (Sat, Sun).
It is necessary to prescribe anticoagulants and antiplatelet agents, for example, cardiomagnyl 100 mg at lunch, or clopidogrel 75 mg at lunch, or warfarin 2.5-5 mg x 1 time per day (necessarily under the control of INR - a parameter of the blood coagulation system, 2.0-2.5 is usually recommended). These drugs prevent increased thrombosis and reduce the risk of heart attacks and strokes.
Chronic heart failure should be treated with diuretics (indapamide 1.5 mg in the morning, veroshpiron 25 mg in the morning) and ACE inhibitors (Prestarium 5 mg in the morning, enalapril 5 mg x 2 times a day, lisinopril 5 mg in the morning), which have an organoprotective effect on the blood vessels and heart.
Lifestyle with atrial fibrillation
All heart diseases require leading a lifestyle that is traditionally characterized as healthy. Atrial fibrillation is no exception.
Standard recommendations include light physical activity for atrial fibrillation: morning exercises, daily walks in the fresh air. A person should maintain natural mobility and should not lie down all the time (except during periods of an arrhythmic attack).
A separate issue is the combination of the diagnosis of atrial fibrillation and alcohol. People with heart disease should not abuse alcohol.
At the same time, it is known that in small quantities alcohol can have a positive effect, in particular: on the nervous system (calming effect), on the digestive system (stimulates digestion), on blood vessels (dilates blood vessels). In exceptional cases, a person suffering from atrial fibrillation can drink no more than 50 g of a drink with 40% alcohol and no more than 150 g of a drink with 12% alcohol per day.
Diet
The diet of such patients should be based on plant-based, low-fat foods, as well as whole grain porridges and water soups. Vegetable stews and casseroles, fresh salads seasoned with a small amount of any refined oil, boiled or steamed sea fish are shown.
You need to eat in small portions: overeating causes irritation of the vagus nerve, which has a depressing effect on the function of the sinus angle, where pathological impulses then arise.
Separately, I would like to say about any alcohol: it should be completely excluded from the nutrition system. Even in relatively healthy people, drinking alcohol can provoke an attack of arrhythmia, which can be very difficult to stop due to rapidly occurring degenerative changes in the heart.
What's the forecast?
The prognosis for life with atrial fibrillation is determined primarily by the causes of the disease. For example, for survivors of acute myocardial infarction and significant cardiosclerosis, the short-term prognosis for life can be favorable, but for health in the medium term unfavorable, since in a short period of time the patient develops chronic heart failure, which worsens the quality of life and shortens it duration.
However, with regular use of medications prescribed by a doctor, the prognosis for life and health undoubtedly improves. And patients with a permanent form of MA registered at a young age, with proper compensation, live with it for up to 20-40 years.