Potassium (K) is one of those minerals that is present in almost all foods. Vegetables, especially green leafy vegetables, and bananas are the best known sources of this macronutrient.
A lack of potassium affects the functioning of the heart and causes chronic fatigue. But the most interesting thing is that this mineral, acting on brain cells, causes a feeling of satisfaction and well-being.
Why is it needed?
Along with sodium and chlorine, potassium is the main element of all cells and tissues of the body. A certain ratio of these elements maintains a constant composition of cellular and intercellular fluid. The interaction between potassium and sodium ensures the normal functioning of cell membranes
.
Potassium is involved in conducting electrical impulses
in nerve and muscle cells. Therefore, it is very important for the normal functioning of the nervous and cardiovascular systems. In addition, potassium acts as a catalyst in carbohydrate and protein metabolism, maintains acid-base balance in the body, regulates blood pressure and helps normal kidney function.
Potassium and magnesium deficiency as a risk factor for the development of cardiovascular diseases
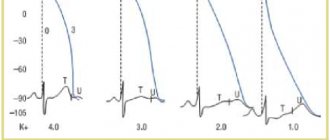
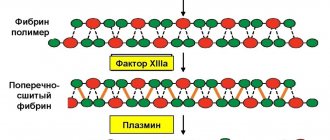
Having imagined the problem of human health in the form of an iceberg, we can say that the developed diseases are only its surface part. And sometimes the underlying causes of disturbances in the coordinated functioning of the body, caused by the development of any pathology, remain completely unclear. It is important to remember that for the friendly functioning of all organs and systems, the body needs daily intake of essential nutrients - including minerals, microelectrolytes and micronutrients. However, how often do we take proper care of our diet? Maintaining a normal balance of potassium and magnesium in the body is the basis of lasting health, which actualizes interest in the problems of studying the biological role of macro- and microelements. Potassium and magnesium are among the most common cations in the body; their deficiency plays a key role in the occurrence of functional disorders of the central nervous system (CNS) and the cardiovascular system (CVS). The importance of their optimal balance for the normal functioning of the body is currently difficult to overestimate [2,3,8]. In recent years, close attention of researchers in various fields of clinical medicine has been drawn to the problem of magnesium and potassium deficiency - a decrease in their concentration inside the cell - and its role in various pathological conditions of organs and systems. Magnesium was first isolated by the English chemist Geoffrey Davy in 1808; it is the main divalent metal (Mg++) of the second group of the Mendeleev periodic system, atomic mass unit 24.305; in ionized form it is a positive ion – a cation with a double positive charge (Mg++); is one of the most common elements on Earth. It is especially abundant in the water of the World Ocean (0.13%), which is close in electrolyte composition to the electrolyte composition of blood serum. Magnesium (Mg++) ranks 4th in concentration in the body among other cations (sodium, potassium, calcium) - 0.6–1.1 mmol/l in blood plasma, and in the cell - 2nd after potassium (K+ ) – 1.6–2.2 mmol/l (erythrocyte). Magnesium and potassium, together with the main inorganic chemical elements: calcium, sodium, chlorine, phosphorus, fluorine, sulfur, carbon, oxygen, hydrogen, nitrogen, determine 99% of the ionic composition of the human body. Currently, it has been established that there are at least 290 genes and protein fragments in the human genome sequence that are capable of recruiting Mg++ and K+ as cofactors of many enzymes involved in more than 300 intracellular biochemical reactions. Magnesium is a natural physiological calcium antagonist, a universal regulator of biochemical and physiological processes in the body: it controls ATP hydrolysis, reducing the separation of oxidation and phospholation, regulates glycolysis, reduces lactate accumulation, promotes potassium fixation in cells, ensuring polarization of cell membranes. Magnesium, by controlling the spontaneous electrical activity of the nervous tissue and conduction system of the heart, ensures the normal functioning of all subcellular structures of the cardiomyocyte, which determines its versatility in cardiocytoprotection (Fig. 1). Magnesium is involved in the energy process (ATP synthesis), plastic (synthesis of protein, lipids, nucleic acids necessary for DNA synthesis), reparative and electrolyte metabolism processes, in the synthesis of connective tissue; takes part in the relaxation of muscle fiber, reduces the aggregation ability of platelets, and maintains normal transmembrane potential in electrically excitable tissues. Magnesium deficiency in autonomic cardiopathy is manifested by a syndrome of prolongation of the QT interval with paroxysms of ventricular tachycardia of the torsades de pointes type, syncope and acute cardiac arrest, accompanied by the development of connective tissue dysplasia syndrome. On the ECG, magnesium deficiency is manifested by slowing of AV conduction, widening of the QRS complex, prolongation of the QT interval, nonspecific decrease in the ST segment and the formation of a pronounced U wave [5]. Neurological manifestations of magnesium deficiency - irritability, depression, sleep disorders, decreased performance, memory, hearing acuity, tinnitus, dizziness, muscle cramps, etc. According to the results of a large prospective clinical study involving more than 41 thousand women aged 38 to 63 years, there is an inverse relationship between magnesium intake and blood pressure levels [2,9]. In turn, potassium is also necessary for the normal functioning of various intracellular enzymes: it maintains osmotic and acid-base homeostasis, takes part in the synthesis of protein, glycogen, nervous system mediators (acetylcholine), etc. Neuromuscular excitability, myocardial contractility, and secretion of the glands of the digestive tract depend on the ratio of this macroelement and other ions. Today it is known that potassium ions are necessary for the regulation of insulin secretion, especially in conditions of impaired glucose tolerance or type 2 diabetes. Most often, hypokalemia affects the cardiovascular system - autonomic cardioneuropathy occurs with complex disturbances in the rhythm of cardiac activity, up to the development of atrial fibrillation or sudden cardiac death. In case of potassium deficiency, an ECG shows a smoothed T wave, a pathological U wave, and polytopic extrasystoles [5]. The results of numerous studies confirm the important role of potassium in the prevention and treatment of arterial hypertension (AH), as well as in reducing the incidence of cerebral stroke. Deficiency of this macroelement leads to increased blood pressure (BP) in patients with essential hypertension [3,14]. Clinical symptoms of the central nervous system with potassium deficiency are asthenia, depression, neuromuscular disorders (muscle weakness, cramps, paresis). Disturbances from the genitourinary system with low potassium levels manifest themselves in the form of atony of the bladder, polyuria, from the digestive system - in the form of decreased intestinal motility with constant constipation, up to paralytic intestinal obstruction (Fig. 2). Thus, the optimal ratio of potassium and magnesium is the basis for the normal functioning of the human body as a whole. Indirect signs of intracellular deficiency of potassium and magnesium are a decrease in their concentration in the blood serum below 3.5 and 0.65 mmol/l, respectively, and specific changes in a standard ECG with clinical manifestations of endothelial dysfunction underlying CVD [2,9]. The endothelium is a monolayer of cells, a semi-selective barrier between the blood and the vascular wall with a length of 7 km, with a total area of 400 m2 and a weight of about 2 kg, the normal function of which is directly dependent on the intracellular balance of electrolytes (potassium, magnesium), plays an extremely important role in the normalization functional state of the cardiovascular system. Endothelial dysfunction is a decrease in the ability of endothelial cells to secrete endothelium-dependent relaxation factor (EDFR) - NO, with a relative or absolute increase in the synthesis of vasoconstrictor, aggregation and proliferative factors. Endothelial dysfunction also occurs due to hyperactivation of the renin–angiotensin–aldosterone system (RAAS) [7,8,11] (Fig. 3). Potassium-magnesium deficiency in clinical practice is quite often the cause of the development of atrial fibrillation (AF). AF is the most common complication of all types of supraventricular tachyarrhythmia, accompanied by severe hemodynamic disorders. AF occurs in the general population in 0.3–0.4% of cases, tends to increase in frequency with age and in the vast majority of cases is a consequence of a violation of the intracellular potassium-magnesium balance of cardiomyocytes. Paroxysms of AF are the cause of more than a third of hospitalizations for cardiac arrhythmias. Currently, AF is most often associated with ischemic heart disease and heart failure. In 60% of patients with AF, hypertension is detected, which in most cases is a concomitant disease [1,4–6]. The clinical picture of AF is determined by the severity of central hemodynamic disorders and varies from asymptomatic to the development of pulmonary edema, syncope, angina attacks, ischemic strokes, etc. The absence of atrial systole reduces the diastolic filling of the ventricles preceding ventricular systole, and with healthy myocardium reduces cardiac output by up to 25%, and with diseases of the left ventricular myocardium - up to 50% (in particular, hypertrophic cardiomyopathy, ACS). Thus, restoration of sinus rhythm in AF is necessary to restore effective pumping activity of the heart in order to prevent the development of acute left ventricular failure, CHF and thromboembolic complications. In restoring sinus rhythm, the state of potassium/magnesium balance, which provides a membrane-stabilizing effect, is of no small importance. Another type of supraventricular and ventricular arrhythmias of the heart caused by a lack of potassium and magnesium is extrasystoles. Extrasystolic arrhythmia (extrasystole) is a disturbance of the heart rhythm due to premature contractions of the heart caused by excitations (of the mikro-re-entry type) occurring outside the sinoatrial node. The occurrence of extrasystoles depends on the state of the nervous system: they are often observed during neuroses and emotional stress (joy, anger, fear, fear, etc.), accompanied by intense loss of potassium and magnesium. A series of extrasystoles can cause transient disorders of cerebral hemodynamics, clinically manifested by general weakness, fatigue, irritability, decreased attention and memory, darkening in the eyes or flashing spots, dizziness, headache, and sleep disturbances [1–3.5]. Chronic deficiency of magnesium and potassium has an adverse effect on the course of coronary artery disease, which is caused by impaired endothelial function, activation of peroxidation, and progression of atherosclerosis [8,10,11]. In IHD, many different factors are involved in the mechanisms for the development of the protective effect of ischemic preconditioning. According to the latest data, in maintaining a normal intracellular energy-phosphate balance, the leading role is played by mitochondrial Mg++ ions, which activate K+ channels, which participate in the electron transport chain of oxidative phosphorylation in mitochondria. The pharmacological opening of ATP-dependent K+ channels using intravenous or oral administration of a potassium-magnesium composition completely reproduces the protective effect of ischemic preconditioning - the protection of cardiomycytes from ischemic damage [8]. In patients with hypertension, there is also a decrease in plasma concentrations of potassium and magnesium with an increase in sodium levels (more than 140 mmol/l). At the same time, activation of the RAAS and endothelial dysfunction in chronic magnesium deficiency create favorable conditions for systemic vasoconstriction and the development of vascular complications in hypertension and CHF. What causes a deficiency of potassium and magnesium in the body? The cause may be an unbalanced diet; in addition, hypomagnesemia and hypokalemia often accompany such types of pathology as cardiovascular diseases, type 2 diabetes, hereditary kidney diseases, severe diarrhea and vomiting. An imbalance of potassium and magnesium can develop with excessive consumption of foods containing potassium and magnesium displacers (NaCl): chips, dried squid and other over-salted foods, since salt promotes the active removal of potassium and magnesium from the body and inhibits their entry into the cell. Potassium and magnesium deficiency can be caused by the uncontrolled use of certain medications: diuretics that do not conserve potassium, cardiac glycosides, gentamicin, etc. The results of numerous studies, the first of which were conducted back in 1928, confirm the role of magnesium and potassium in prevention and treatment AG. The Rotterdam Study (1996) involved more than 3,200 people over the age of 55 years who were not taking antihypertensive drugs [9,13,14]. The results of this study confirm that increases in potassium and magnesium intake were associated with decreases in systolic and diastolic blood pressure. The 5-year randomized placebo-controlled SHEP (Systolic Hypertension in the Elderly Program) study analyzed data from more than 4 thousand elderly patients with isolated systolic hypertension. Its purpose was to determine the relationship between hypokalemia, which occurs with low-dose diuretics, and cardiovascular events. The results obtained indicate that a significant reduction in the risk of developing cardiovascular complications, such as heart attack and stroke, when treated with diuretics occurred in patients with normal levels of potassium and magnesium in the blood. No less interesting is another study, the purpose of which was to study the effect of potassium, magnesium, calcium and fiber intake on the risk of stroke. The trial included more than 43 thousand men aged 40 to 75 years without diagnosed cardiovascular disease or diabetes. Over the next 8 years, 328 hemorrhagic and ischemic strokes were recorded. Based on the analysis of the results obtained, an inverse relationship was identified between the level of potassium and magnesium intake and the risk of stroke [6,9,13,14]. Restoring potassium and magnesium reserves helps correct endothelial dysfunction, which is the initiator of the formation and progression of CVD. According to various researchers, the administration of oral magnesium and potassium supplements to patients with coronary artery disease was accompanied by a significant increase in endothelium-dependent dilatation of the brachial artery by 15.5% (p<0.01) compared with placebo - by 4.4% (p>0.05) , while a linear correlation was revealed between the intracellular concentration of magnesium and the degree of vasodilation [9,11]. Taking into account the antiatherogenic effects of magnesium drugs, correction of its deficiency can help slow the progression of coronary artery disease [2,7–9]. In the ARIC (The Atherosclerosis Risk In Communities) study, after 4–7 years of follow-up of 13,922 patients, an analysis of risk factors showed a connection between the development of coronary artery disease and hypomagnesemia [9]. The most pronounced magnesium deficiency occurs in patients with elevated levels of atherogenic lipids [8]. Often, patients with CVD are diagnosed with type 2 diabetes, in which magnesium deficiency increases, especially in old age. The use of magnesium supplements in such patients improves insulin-dependent glucose utilization [10]. Potassium and magnesium deficiency in patients with CHF is associated with poor quality of life and prognosis. The prescription of magnesium- and potassium-containing drugs is especially justified during long-term use of cardiac glycosides and diuretics, which provoke hypomagnesemia/hypokalemia and subsequent cardiac arrhythmias associated with a deficiency of these electrolytes [3,9,12]. The antiarrhythmic effect of magnesium is realized through its effect on the transport of sodium, potassium and calcium ions involved in the formation of the action potential [2]. As an antiarrhythmic, magnesium salts are most often used for torsades de pointes due to their ability to inhibit the development of trace depolarizations, shortening the duration of the QT interval. Magnesium can be used both for congenital long QT syndrome and for its iatrogenic variant caused by the use of class 1 antirhythmics and other drugs [3,5]. Magnesium preparations are used to prevent arrhythmias provoked by digitalis intoxication when the function of the potassium-sodium pump is impaired [8]. Timely replenishment of potassium and magnesium reserves in the body is necessary for patients with CVD. These intracellular cations improve myocardial metabolism, take part in the molecular mechanisms of muscle contraction and are necessary for the functioning of many intracellular enzymes. Considering the important role played by the microelements potassium and magnesium in the normal functioning of the body, it is advisable to use combination preparations containing potassium and magnesium. The combination of potassium and magnesium ions in one preparation is justified by the fact that potassium deficiency in the body is accompanied or caused by magnesium deficiency and requires simultaneous correction of the content of both cations in the body. When the levels of these electrolytes are simultaneously corrected, an additive effect is observed; At the same time, potassium and magnesium reduce the toxicity of glycoside drugs during the treatment of CHF, without negatively affecting their positive inotropic effect. Such combination drugs include the over-the-counter drug Panangin (), which over many years of presence on the pharmaceutical market of the Russian Federation has managed to win the trust of consumers. Panangin can be safely recommended not only to patients with the SVD, but also to healthy people in order to replenish the deficiency of these important cations and timely prevention of a wide range of pathological conditions. Endogenous asparaginate, characterized by a large affinity to cells, acts as a panangin, acts as a conductor of ions into the cell, i.e. Promotes faster and more effective entry of potassium and magnesium into myocytes. At the same time, potassium and magnesium asparaginate have a positive effect on myocardial metabolism. Indications for the use of Panangin for therapeutic and preventive purposes are: alimentary hypokalemia and hypomagnesia, as well as CCC diseases in the complex therapy of heart failure, with myocardial infarction and heart rhythm disorders. In addition, Panangin must be prescribed in the treatment of cardiac glycosides (to increase their effectiveness and improve the tolerance of drugs of this group). Given the high prevalence of the CVD in the Russian Federation, this drug rightfully occupies an important place in the therapeutic and preventive recommendations of primary healthcare doctors. In the treatment of rhythm of cardiac activity, Panangins are prescribed 2-3 tablets of 3 r./Day, the maximum daily dose - 3 tablets 3 r./Day. As a maintenance or preventive therapy (to prevent the development of arrhythmias during treatment with diuretics), the drug should be prescribed 1-2 tablets 3 times a day. After eating, because The acidic medium of the contents of the stomach reduces the effectiveness of its absorption. The use of infusion solutions of panangin is possible as the prevention of arrhythmias, as well as in some cases for their relief, for example, in patients with ACS, CHS when taking heart glycosides [8]. Panangin is a non -toxic drug, does not have a cumulative effect and has a limited list of relative contraindications for its use: acute or chronic renal failure (oliguria, anuria), an atrioventricular blockade of the III degree, acute metabolic acidosis, hypovolemia (dehydration), individual Hypersensitivity to the components of the drug. Thus, intracellular concentrations of K+ and Mg ++ ions provide normal metabolism of the central nervous system and CCC and, as already mentioned, are the basis of the normal functioning of the human body. The occurrence of potassium and magnesium deficiency - a decrease in intracellular concentration below reference values - is accompanied by clinical manifestations of violations of the functions of the CSC (IBS, OKS, AG, rhythm disorders) and central nervous system (chronic fatigue syndrome, circulatory encephalopathy), is a consequence of the violation of the balance Between their delivery and the pace of excretion. The deficiency of potassium and magnesium should be compensated with the help of combined drugs, simultaneously containing potassium and magnesium. The most effective in the prevention and treatment of CVD complications is a drug containing potassium and magnesium asparaginate, Panangin.
Literature 1. Cardiac arrhythmias. Mechanisms, diagnosis, treatment. T. 1. M.: Medicine, 1996. P. 346–379. 2. Gromova O.A. Magnesium and pyridoxine: basic knowledge. New technologies for diagnosing and correcting magnesium deficiency. UNESCO training programs. M.: RSC Institute of Microelements, 2006. pp. 3–176. 3. Metelitsa V.I. Handbook of clinical pharmacology of cardiovascular drugs. M., 2002. pp. 509–513. 4. Nechaeva G.M., Yakovlev V.M., Druk I.V., Tikhonova O.V. Heart rhythm disturbances in undifferentiated connective tissue dysplasia // Attending physician. 2008. No. 6. P. 2–7. 5. Tomov L., Tomov I. Heart rhythm disturbances. Clinical picture and treatment. Sofia, 1976. pp. 62–81. 6. Fonyakin A.V., Mashin V.V., Geraskina L.A., Mashin V.Vl. Cardiogenic encephalopathy. Risk factors and approaches to therapy // Consilium Medicum. 2012. T. 14. | No. 2. P. 4–7. 7. Shevchenko O.P., Praskurnichy E.A., Shevchenko A.O. Arterial hypertension and obesity. M.: Reopharm, 2006. 8. Shilov A.M. Myocardial infarction. M.: Miklos, 2009. pp. 7–163. 9. Shilov A.M., Melnik M.V., Osiya A.O. Treatment of cardiovascular diseases in the practice of a primary care physician: the place of potassium and magnesium preparations (Panangin) // RMZh. 2012. No. 3. pp. 102–107. 10. Barbato JE, Zuckerbraun BS, Overbaus M and al. Nitric oxide modulates vascular inflammation and intimal hyperplasia in insulin resistance and metabolic syndrome // J. Physiol. Heart. Circ. 2005. Vol. 289. R. 228–236. 11. Caballero AE Endothelial dysfunction in obesity and insulin resistance: a road to diabetes and heart disease // Obes. Res. 2003. Vol. 11. R. 1278–1289. 12. Kannel W. Fifty years of Framingham Study contributions to understanding hypertension // J Hum Hypertens. 2000. Vol. 14(2). R. 83–90. 13. Jellinek H., Takacs E. Morphological aspects of the effects of orotic acid and magnesium // Arzneimittelforschung. 1995. Aug. Vol. 45 (8). R. 836–842. 14. Seelig MS Metabolic Syndrom–X. A complex of common diseases – diabetes, hypertension, heart disease, dyslipidemia and obesity – marked by insulin resistance and low magnesium/high calcium // Mineral Res. Intern. Tech. Prod. Infor. 2003. R. 1–11.
What if it's not enough?
A lack of potassium causes problems in the functioning of the cardiovascular system: heart rhythm disturbances, changes in the heart muscle, heart attacks. The nervous and muscular systems
suffer - with a lack of potassium, a person constantly feels tired, muscle weakness, and shows signs of depression. Potassium deficiency leads to increased blood pressure, deterioration of intestinal function, food digestion, kidney function, lung function, and even miscarriage and infertility.
How to determine potassium deficiency
Potassium deficiency is characterized by the following symptoms
:
- fatigue, weakness, loss of strength;
- high blood pressure;
- muscle weakness, spasms and cramps;
- cardiac arrhythmia;
- constipation;
- tingling and numbness in the arms and legs;
- swelling;
- dizziness.
These symptoms indicate low levels of energy reserves in the muscles. The fact is that potassium is necessary to convert blood sugar into glycogen.
Because glycogen is used by muscles as an energy source, potassium deficiency causes noticeable fatigue and muscle weakness.
Leg cramps, especially ones that wake you up in the middle of the night, can also be associated with low magnesium and calcium levels.
Insufficient amounts of potassium and magnesium can contribute to the development of chronic fatigue syndrome. Often, just replenishing the body's mineral reserves with equal amounts (250-500 mg) of organic potassium and magnesium salts is enough to restore muscle tone, increase energy levels and increase endurance.
Results can often be noticeable in as little as a week. If this duo doesn't help on its own, it may still be a useful addition to treating other types of fatigue.
What can cause potassium deficiency?
In addition to insufficient potassium in the diet:
- consumption of foods not saturated with this element;
- increased excretion of potassium from the body along with urine;
- hyperfunction of the adrenal cortex and anterior pituitary gland;
- primary and secondary aldosteronism (increase in the hormone aldosterone);
- increased secretion of antidiuretic hormone;
- active treatment with corticosteroids;
- taking large amounts of potassium-free liquid for vomiting and diarrhea;
- diabetes;
- diabetes insipidus;
- magnesium deficiency;
- cystic fibrosis;
- acidosis.
The amount of potassium excreted through sweat can be very significant, especially during long exercise sessions in the heat. Athletes or people who exercise regularly may have a high need for this micronutrient.
What prevents it from being absorbed?
Maintaining a stable internal environment in the body mainly depends on the balance of potassium and sodium, so a deficiency of the former can be caused by excess consumption of the latter. As a rule, potassium deficiency due to an excess of sodium
develops in those who like to heavily salt their food and consume large amounts of canned food, smoked meats and pickles.
Potassium is excreted from the body during intense physical exertion, in hot climates and during profuse sweating during illness. Potassium is also actively excreted
with the constant use of laxatives and diuretics, including in weight loss medications. Potassium balance should be monitored by those who take hormonal medications or adhere to a strict diet. Alcohol consumption or a lack of magnesium in the body greatly harms potassium absorption.
Potassium in food
Around the world, perhaps the most famous source of potassium is the banana. Meanwhile, there are many other products in which the content of this mineral significantly exceeds its concentration in an exotic fruit.
To begin with, it is important to note that the most foods rich in potassium are fruits (especially dried fruits) and vegetables. But this does not mean that you should neglect legumes, fish and dairy foods - they also contain potassium reserves. It is important to include chard, beans, chicken eggs, spinach and mushrooms in the menu. Such a diet will supply the body with minerals in the amount of 150% of the daily requirement. Other foods rich in potassium include: potatoes, tomatoes, avocados, spinach, beans, peas, dried fruits (raisins, dried apricots, prunes), orange juice, fruits and berries (bananas, oranges, strawberries).
Considering the concentration of potassium in products, they are usually grouped into:
- low content (contain less than 100 mg of mineral per 100 g of product);
- with an average K content (150-250 mg);
- with high content (251-400 mg);
- very saturated with potassium (more than 400 mg).
Table of potassium content in food
| Product name (100 g) | Potassium (mg) |
| Dried apricots | 1717 |
| Soybeans | 1607 |
| Sea kale | 970 |
| Green pea | 873 |
| Prunes | 864 |
| Raisin | 860 |
| Spinach | 838 |
| Almond | 750 |
| Hazelnut | 717 |
| Lentils | 672 |
| Peanut | 660 |
| Potato | 570 |
| Potatoes baked in skins | 540 |
| Parsnip | 537 |
| Brussels sprouts | 494 |
| Salmon | 492 |
| Avocado | 480 |
| Broccoli | 450 |
| Chard | 379 |
| Banana | 348 |
| Parsley (greens) | 340 |
| Cod | 340 |
| Mussels | 310 |
| Beans | 307 |
| Apricot | 305 |
| Tuna | 298 |
| Turkey | 290 |
| Celery (root) | 262 |
| Parsley (root) | 262 |
| Beetroot (root) | 259 |
| Eggplant | 238 |
| Beet tops | 238 |
| Blackberry | 233 |
| Lean beef | 325 |
| Oysters | 220 |
| Tomatoes | 213 |
| Nectarine | 203 |
| Orange | 197 |
| Carrot | 195 |
| Figs | 190 |
| Grapefruit | 184 |
| Cauliflower | 176 |
| Zucchini | 172 |
| Strawberries | 161 |
| Raspberries | 158 |
| Cucumber | 153 |
| Strawberry | 153 |
| Melon | 118 |
| Watermelon | 117 |
A Brief History of Hypertension
It's hard to imagine that modern technology for measuring blood pressure has only been around for a little over 100 years (when Russian surgeon Dr. Kortokov described the method in an article). Previously, no one knew what “normal” blood pressure should be in a person. Population-based studies were later conducted to answer this question. With this knowledge came the realization that high blood pressure can increase the risk of cardiovascular disease.
Unfortunately, in the early 20th century there was no good treatment for hypertension. Whatever small treatment strategies there were, they look almost medieval and barbaric by today's standards.
These include bloodletting through phlebotomy or even kidney cutting. In fact, high blood pressure has even been referred to as malignant hypertension, the word malignant suggesting that the prognosis is as bad as cancer.
Modern methods of treating high blood pressure
Today, doctors no longer have to play vampire to treat their patients.
This is due in part to an improved understanding of human blood pressure physiology and the influence of external factors such as diet (which includes electrolytes such as sodium, potassium, etc.). However, like many problems, the more we learn, the more questions arise.
Thus, the average person may be mistaken in thinking that the modern physician has perfected the art and science of treating blood pressure. But even today, the treatment and approach to hypertension is still the subject of intense research and debate. One need only look at the several guidelines published by organizations around the world that tell the average physician when and how to treat high blood pressure. Each of them claims to be the final word on the subject; that is, until the next guide comes along.
How is blood pressure regulated?
Before we understand the role of potassium in regulating blood pressure, it is important to have an understanding of how our pressure thermostat works. This thermostat involves a complex coordination of mechanisms regulated by our nervous system, kidneys, endocrine system that creates hormones, the heart, our blood vessels, the amount of fluid flowing in the blood vessels, our electrolyte levels and much more.
Sometimes it seems trivial (like when you say “my blood pressure is 120/80”), but it is fascinating to realize how this ultra-complex mechanism must work in perfect coordination every second of our lives.