Pulse rate is an important indicator that can tell a lot about a person’s health and condition. If even at rest the heart beats very quickly, it means that it is trying to “tell” about some problems in the body.
In general, the lower your heart rate, the better your health. This means that the heart contracts normally and pumps out enough blood to supply all organs. And if the pulse is too fast, it means that the heart is not doing its job very well and is trying to compensate for this. The normal heart rate for an adult is between 60 and 100 per minute. It is more common in children - there are different norms for each age group.
General information
Hypoxia is a pathological condition characterized by insufficient oxygen content in tissues and blood ( hypoxemia ) or disruption of its utilization processes during biological oxidation with the development of secondary nonspecific functional/metabolic disorders and subsequent adaptation reactions.
The term “hypoxia” usually refers to various variants of oxygen deficiency, but sometimes in the literature the term “hypoxemia” is distinguished, meaning a decrease in O2 tension in the blood, “anoxemia” - the absence of O2 in the blood and “anoxia” - the absence of O2 in the tissues, but true anoxemia / anoxia is extremely rare. In practice, anoxia occurs only in laboratory conditions. Quite often in everyday life you can hear the expressions “brain hypoxia”, “heart hypoxia”.
What does this mean? This means that the brain structures or heart muscles lack oxygen. However, it is necessary to distinguish hypoxia from ischemia , in which a decrease in volumetric blood flow in tissues is primarily observed, which is accompanied by a natural decrease in O2 tension. During ischemia, insufficiency of ATP synthesis acutely develops, and it is mainly the result of a decrease in the supply of energy substrates (glucose) to the tissues, in contrast to hypoxia, in which ATP synthesis gradually decreases as a result of a decrease in oxygen tension in the tissues. Therefore, tissue damage during the development of ischemia develops faster than in cases of hypoxia.
It is important to note that not all organs and tissues of the body have the same sensitivity to O2 deficiency. The central nervous system and, above all, the cerebral cortex react most acutely, which reacts even to a slight lack of oxygen in the brain, and in cases of a significant decrease in oxygen tension in the brain tissue, severe/irreversible changes develop. The myocardium is also quite sensitive to lack of oxygen.
Normally, there is an equilibrium between capillary blood and alveolar air and the O2 pressure at the end of the pulmonary capillaries is practically no different from the O2 pressure in the alveolar air. Oxygen is transported through the blood to the tissues, where it leaves the capillaries and enters the cells along a partial pressure gradient. After which PO2 in venous blood decreases and becomes (on average 55 mm Hg) less than in arterial blood. Oxygen in the blood is mainly bound to hemoglobin, and only a small part of it is dissolved in the plasma. At the same time, 1 g of hemoglobin at full saturation binds 1.3 ml of oxygen. When breathing air, normal O2 saturation is about 98%. The binding of hemoglobin to oxygen depends on O2 pressure and this dependence is described by the S-shaped curve (Fig. below) of oxyhemoglobin dissociation.
It must be taken into account that hypoxia should not always be considered only as a pathological process. A person in his daily activities often experiences the effects of so-called “physiological hypoxia”, which can form during intense muscular work in the skeletal muscles, with pronounced mental stress in the brain tissue, as well as in the gastrointestinal tract, liver, kidneys with excessive physiological activity of these organs (stress hypoxia). It is important to take into account that periodically occurring physiological hypoxia in various tissues often acts as a natural irritant that activates various reactions of the body, including reflex ones, changing the overall activity of the body and target organs.
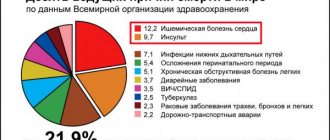
The body of a healthy person in most cases is exposed to exogenous acute hypoxia, which is usually caused by a decrease in the partial pressure of O2 in the inhaled air/gas mixture during extreme conditions in certain professions/sports (pilots, divers, high-altitude tourists, climbers, submariners). Extreme medicine is also associated with the concept of acute hypoxia (acute blood loss, trauma, heart attack , stroke , poisoning, airborne infections, endogenous/exogenous intoxication, etc.).
Characteristics of adaptive reactions during hypoxia (acute and chronic)
Hypoxia of any type, caused by various factors, is accompanied by immediate/delayed activation of characteristic adaptive reactions at all levels - behavioral, systemic/organ, molecular-cellular, aimed at maintaining homeostasis . The structure of the adaptation system for hypoxia includes the heart/vascular system, lungs, blood, regulatory systems and biological oxidation systems. Under conditions of the development of acute hypoxia, adaptation mechanisms are of an urgent/functional nature, while in chronic hypoxia long-term structural adaptation is involved.
Adaptation reactions during acute hypoxia
External respiration system
Adaptation is ensured by deepening/increasing respiratory excursions and involving reserve alveoli in the respiratory process with an adequate simultaneous increase in pulmonary blood flow. At the same time, the minute volume of ventilation/perfusion can increase 10-15 times relative to the resting state. The appearance of hyper/tachypnea is ensured by activation of peripheral/central chemoreceptors against the background of hypoxia, changes in blood gas composition, hypercapnia and acidotic changes in the blood.
Heart/vascular system
In response to a lack of oxygen, adaptive hormones are released, the sympathoadrenal system is sharply activated, which causes tachycardia , an increase in IOC, volumetric/linear blood flow velocity, and an increased release of deposited blood. At the same time, against the background of the release of catecholamines and activation of the sympathoadrenal system, the so-called “blood flow redistribution phenomenon” develops, which contributes to the narrowing of arterioles and a decrease in blood flow to the vast majority of peripheral organs/tissues (abdominal organs, subcutaneous tissue, muscles). As a result, the centralization of blood flow in the vessels of the heart, brain, and respiratory muscles increases.
Blood system
Quantitative/qualitative changes are noted in the blood system. Quantitative adaptive changes occur under the influence of high concentrations of corticosteroid / thyroid hormones / catecholamines and are expressed in an increase in the mass of circulating blood due to the increased release of red blood cells from the bone marrow / blood cells from the depot. Qualitative changes are caused by an increase in the affinity of Hb for oxygen in the capillaries of the lungs.
Biological oxidation systems
Adaptation occurs due to the activation of metabolism and is characterized by an improvement in the efficiency of the absorption of oxygen and various oxidation substrates by body tissues, the delivery of oxidation substrates to mitochondria, an increase in the coupling of phosphorylation/oxidation processes and a sharp activation of glycolysis.
The figure below shows adaptation reactions during acute hypoxia.
Adaptation reactions during chronic hypoxia
External respiration system
The basis for ensuring a sufficient level of gas exchange is an increase in the power of the respiratory muscles and the capacity of the chest, an increase in the area of the alveoli, the number of capillaries in the partitions between the alveoli, and activation of the diffusion function of the alveolar-capillary membranes.
Heart/vascular system
Based on myocardial hypertrophy (the speed and strength of myocardial contraction/relaxation processes increases, the volume of cardiac output increases, the speed of transmembrane processes and the rate of interaction between myosin and actin in the myofibrils of cardiomyocytes increase). Providing the required level of tissue perfusion with blood is achieved by increasing the number of capillaries and developing arterial hyperemia .
Blood system
Adaptive reactions occur in the bone marrow due to increased erythropoiesis (increased production of erythropoietin by the kidneys). In the peripheral blood, the content of erythrocytes increases to a level of 6-7 million and hemoglobin (to a level of 170-180 g/l).
Endocrine system
Adaptation is carried out by increasing the sensitivity of cellular receptors to hormones, which helps to reduce their synthesis in the endocrine glands. Against this background, the level of sensitivity of the hypothalamic-pituitary-adrenal system increases, which significantly limits the pathogenic effects of stress reaction mechanisms.
Adaptation reactions during chronic hypoxia
Hypoxia detection methods
The fulminant and acute form of the pathology is determined by symptoms and requires immediate resuscitation and restoration of the oxygen balance in the blood. In chronic cases, identification of the root cause and concomitant diseases is required. After attacks of hypoxia, it is also necessary to carry out a series of diagnostic manipulations in order to fix the damage caused to internal structures.
The following instrumental methods are designed to cope with the diagnostic task:
- Pulse oximetry. It is carried out using a measuring device – a pulse oximeter, placed on the patient’s finger. It only takes a few seconds to calculate your blood oxygen saturation. The normal rate is 95% and above.
- Study of pH balance, gas content in venous and arterial blood.
- Capnography/CO-metry. Measures the ratio of gases in the air exhaled by the patient.
- MRI. Allows you to detect the cause of chronic hypoxia, the degree of damage to brain tissue, internal organs and systems, possible obstacles in the pulmonary area, intoxication disorders, blockage of blood vessels, tumors that prevent blood flow to the brain.
In diagnosing the root causes of the disease, magnetic resonance scanning remains the most effective method. If the results of other studies provide an incomplete picture, the neurologist writes a referral for a full MRI examination. Only MRI screening can detect tumor formations hidden inside the skull, the severity of damage to the meninges after a heart attack, and other anomalies leading to hypoxia.
Pathogenesis
Since the pathogenesis of each type of hypoxia is different and it is not possible to consider them within the scope of the article, we will consider only exogenous hypoxia. Regardless of the cause of this type of hypoxia, the main links in its pathogenesis include:
- Arterial hypoxemia . A decrease in O2 tension in arterial blood is the initiating and main element of exogenous hypoxia. Developing hypoxemia leads to a decrease in hemoglobin oxygen saturation and total oxygen content in the blood, which causes metabolic/gas exchange disorders in tissues.
- Hypocapnia (decreased carbon dioxide tension in the blood). Occurs as a result of compensatory hyperventilation of the lungs caused by hypoxemia.
- Gas alkalosis as a result of hypocapnia , followed by acidosis .
- Arterial hypotension . A decrease in systemic blood pressure, combined with tissue hypoperfusion. CO2 is one of the main regulators of cerebral vascular tone, and a pronounced decrease in CO2 causes a narrowing of the lumen of brain arterioles and heart vessels and a significant decrease in their blood supply. Such changes cause disorders of the body's functioning (fainting/coronary insufficiency).
- Simultaneously with such deviations, an imbalance in the ion balance occurs ( hypernatremia / hypocalcemia / hypokalemia ) in biological fluids and tissue cells (in the intercellular fluid, cerebrospinal fluid, lymph, blood plasma).
Classification
The classification of types of hypoxia is based on several criteria - the causes of development, the speed of their development, the severity of disorders in the body, duration.
Due to development they distinguish:
- exogenous types of hypoxia (normal/hypobaric);
- endogenous types of hypoxia (respiratory, circulatory, hemic, tissue, overload type of hypoxia, substrate type of hypoxia, mixed hypoxia).
According to the severity of disorders of the body's vital functions, they are distinguished:
- mild degree;
- moderate (average) degree;
- severe;
- critical (lethal).
Based on the speed of occurrence/duration of the hypoxic state, the following are distinguished:
- Lightning—occurs within seconds after exposure to the causative factor.
- Acute - develops within a few minutes after exposure to the causative factor (acute respiratory failure, acute blood loss).
- Subacute - develops over several hours within the first day (in case of poisoning with benzene, nitrates, nitrogen oxides).
- Chronic - development period from several days to several years (with respiratory/heart failure, chronic anemia).
Causes
The causes of each type of hypoxia are different and are briefly presented below.
Exogenous types of hypoxia (normo/hypobaric varieties)
The cause of exogenous hypoxia is a decrease in the partial pressure of oxygen in the air entering the body. Hypoxia of this type can develop at normal barometric pressure (normobaric hypoxia) or with a decrease in barometric pressure (hypobaric hypoxia). The causes of normobaric hypoxia are conditions that contribute to limiting the supply of oxygen with air into the body against the background of normal barometric pressure:
- Disturbance in the supply/regeneration of breathing air in deep/airborne vehicles, autonomous suits of rescuers, pilots, firefighters, divers.
- Finding people in a poorly ventilated/small confined space (elevator shaft, well).
- In cases of violation of the technique of artificial ventilation.
The causes of hypobaric hypoxia are reduced barometric pressure. Hypoxic hypoxia develops mainly when a person rises to an altitude of more than 3000–3500 m (hypoxic hypoxia is observed when the air O2 pressure decreases to 100 mm Hg) or in a pressure chamber. In such conditions the following may develop:
- Mountain sickness, which is observed when a person climbs the mountains on foot, where his body is exposed to low oxygen content in the air and barometric pressure, as well as severe physical activity, increased insolation, and cooling.
- Altitude sickness - develops when a person is lifted in open aircraft to a high altitude or in cases of decreased pressure in the pressure chamber.
- Decompression sickness (caisson sickness) occurs when there is a sharp decrease in barometric pressure when a person quickly rises from great depths to the surface.
Endogenous types of hypoxia
The causes of endogenous hypoxia are, in most cases, pathological processes in the human body and diseases that contribute to insufficient transport of oxygen, metabolic substrates to various organs or their use by tissues. Also, hypoxia of this type can develop as a result of a significant increase in the body’s need for energy due to excessive physical/mental stress.
Respiratory hypoxia
The main cause of respiratory hypoxia is respiratory failure (insufficient gas exchange in the lungs), which is most often caused by hypoventilation of the alveoli ; decreased diffusion through the airborne oxygen barrier ; hypoperfusion of lung tissue with blood.
Circulatory hypoxia (local and systemic)
The main cause of circulatory hypoxia is insufficient blood supply to organs/tissues. The causes of local hypoxia are most often local circulatory disorders in the form of ischemia , venous hyperemia , stasis, and regional disorders of the process of oxygen diffusion to cells. The causes of systemic hypoxia are mainly heart failure , hypovolemia , generalized decrease in the tone of the walls of arterioles / venules .
Hemic hypoxia
The cause of blood (hemic) hypoxia is a decrease in the oxygen-transporting function of the blood, i.e., a decrease in the effective oxygen capacity, which causes a lack of oxygen in the patient’s blood.
Tissue hypoxia
The main causes of tissue hypoxia are factors that disrupt the process/reduce efficiency:
- utilization of oxygen by tissue cells;
- of phosphorylation and oxidation processes in mitochondria
Substrate type of hypoxia
The main reason for its development is a deficiency of biological oxidation substrates (glucose) in cells in the absence of significant disturbances in the delivery of oxygen to cells.
Overload type of hypoxia
The reason is a long-term (significant) increase in the function of organs, systems and tissues. Most often develops in situations caused by prolonged/increased functioning of skeletal muscles and myocardium.
Signs of an abnormal condition
The disease is characterized by typical symptoms:
- increased excitability at the initial stage of the disease;
- a feeling of euphoria accompanied by loss of coordination;
- change in skin tone towards discoloration, blueness or severe redness, increased sweating at cold temperatures;
- central nervous system inhibition, nausea, weakness, characteristic of the second stage of the disorder;
- loss of clarity of visual perception, darkening of the eyes, “interference” (the condition often ends in fainting);
- loss of reflexes as a result of the development of swelling of the brain.
With continued oxygen deficiency, the patient falls into a deep coma. Rapid death may occur.
Symptoms
Lack of oxygen in the body can manifest itself with various symptoms depending on the severity of hypoxia and the specific disease causing it. Thus, with acute hypoxia, symptoms of oxygen starvation of the brain first appear in the form of decreased critical/logical thinking, a feeling of discomfort, incoordination of movements, and disturbances of consciousness. Symptoms of cerebral hypoxia can manifest themselves in the appearance of various “bulbar disorders.”
In subacute forms of hypoxia, there is increased drowsiness , fatigue, memory impairment, decreased concentration, headache , and periodic dizziness . Myocardial hypoxia can be manifested by decreased blood pressure , tachycardia , increased cardiac output; pallor/blueness of the skin, increased depth/frequency of breathing or, conversely, rare and shallow breathing, swelling of the lower extremities. In this case, symptoms can be of varying degrees of severity and vary significantly. As an example, the symptoms of altitude sickness will be discussed in more detail.
Altitude sickness
Exogenous acute hypoxia with hypobaria , as already indicated, can develop due to a decrease in general atmospheric pressure, which occurs when climbing mountains, especially in the absence of acclimatization (mountain sickness) or in cases of flying in unpressurized aircraft (altitude sickness). When assessing the effect of hypoxia on physiological processes, it is important to understand that the speed/severity of the body’s response to a decrease in pressure is determined by several factors: the degree of hypobaria; rate of pressure reduction; duration of hypobaria; individual sensitivity of individuals to oxygen deficiency; physical condition of the body. It is also important to take into account that in high altitude conditions, in addition to hypobaria/hypoxia, a person is additionally influenced by a complex of natural factors - the “mountain complex”, including low air humidity, exposure to low temperature, high solar radiation/air ionization, wind and high physical activity.
For the vast majority of untrained people, the altitude at which the normal level of partial pressure of oxygen in the atmosphere is maintained and normal mental activity is 3000 m, but the first changes in a person’s well-being when climbing are observed already at an altitude of 2200-2500 m. Mild malaise and headache , dizziness , drowsiness , nausea . Objectively - increased breathing, slight tachycardia , less often - the appearance of euphoria .
shortness of breath occur , and behavior resembles a state of alcohol intoxication. Attacks of suffocation may occur, breathing becomes arrhythmic. Some individuals develop noncardiogenic pulmonary edema . When climbing to a height of 5000 meters or more, acute physical weakness, pale skin, dizziness , tachycardia , severe shortness of breath , intense headaches, and bleeding from the ears/nose appear. Possible mental disorders. Affected individuals experience a feeling of doom/helplessness, facial features become sharpened, and clonic convulsions .
Against the background of low temperatures, pulmonary/brain edema can occur quickly (8-12 hours). These complications develop mainly at night due to:
- a decrease in the activity of the central nervous system, which, against the background of respiratory acidosis, contributes to a weakening of respiratory function;
- increased venous return (due to a change in body position) to the upper half of the body;
- increased tone of the vagus nerve, which increases bronchospasm .
How does it manifest itself?
Acute cerebrovascular accident or stroke manifests itself with severe symptoms. May be observed:
- speech disorders,
- decreased sensitivity, numbness of the limbs;
- nausea, vomiting;
- numbness of half the face, asymmetry of the tongue;
- visual impairment (“spots”, spots, loss of vision);
- coordination problems.
Chronic cerebrovascular accident develops gradually. Many people ignore the body’s signals, considering poor health to be the consequences of overwork. But a mild disorder gradually becomes a chronic disease. In this case, there will be no quick recovery: you will have to undergo a course of treatment, possibly in a hospital. Here are the signs of chronic circulatory disorders in the brain:
- weakness, drowsiness;
- difficulty concentrating;
- minor motor disturbances (unsteadiness of gait, as the disease progresses - tremors of the hands, stiffness of movements);
- dizziness.
Prevention
Prevention of AMS should first involve assessing the degree of risk individually for each participant going to high altitude (see table below).
For a low-risk individual, there is no need for prophylactic medications and participants should focus on following a gradual climb schedule. Thus, at altitudes of 3000 meters or more, participants should not increase the altitude of their overnight stop by more than 500 meters/day with a mandatory rest day. If it is impossible to comply with this requirement (relief and other factors do not allow it), it is recommended to arrange a rest day immediately before a large climb or immediately after it at the nearest point with the expectation that the total rate of climb over the period covered will be below 500 meters/day.
A stepped climb/pre-acclimatization significantly reduces the risk of developing mountain sickness, improves oxygenation/ventilation, and reduces the increase in pressure in the pulmonary artery during subsequent climbs.
Individuals at moderate/high risk of developing AMS are recommended to take the mountain sickness tablet Dexamethasone . Doses for adults are 2 mg every 6 hours or 4 mg every 12 hours. Higher doses (4 mg every 6 hours) should only be prescribed in high-risk situations. In this case, the duration of taking dexamethasone in order to avoid suppression of adrenal function/development of glucocorticoid intoxication should not exceed 10 days.
Acetazolamide ( Diacarb ) is also quite effective in preventing AMS (125 mg tablets 2 times a day). However, it is necessary to carefully monitor doses, since increasing them is accompanied by a high risk of side effects. Nifedipine , Tadalafil , Sildenafil are indicated for the prevention of high-altitude pulmonary edema .
The use of other drugs (coca tea, chewing coca leaves, leukotriene receptor blockers, antioxidants, phosphodiesterase inhibitors, Spironolactone / Sumatriptan , salicylic acid ) does not have a positive effect in the prevention of AMS.
Overhydration (increased drinking regimen) also did not demonstrate a positive effect in the prevention of AMS, but at the same time, the risk of hyponatremia .
Some authors believe that resistance to hypoxia is expressed during exercise in special masks, which, in their opinion, imitate hypoxic conditions.
The oxygen deprivation mask restricts the air flow entering the nose/mouth, thereby attempting to simulate the effect of training at high altitudes. At the same time, the mask has a mechanism for regulating the flow of air, which allows for altitudes from 900 to 5500 meters. According to the manufacturer, the use of masks allows you to achieve a significant increase in the key marker of growth in aerobic endurance - VO2max.
However, to date, the effectiveness of using training masks has been studied extremely poorly and many believe that a training mask has nothing to do with hiking in high altitudes. Despite the fact that it is difficult to breathe both at high altitudes and in a mask, the reasons for this are completely different: at high altitudes there is less oxygen in the air, but when using a mask, the oxygen does not become less. It is simply harder for a person to breathe. Therefore, masks cannot be considered a sports accessory that simulates hiking in the highlands. Rather, they can be considered as a simulator used to strengthen the inspiratory muscles involved in the act of inhalation.
Consequences and complications
Regardless of the cause of hypoxia, its development leads to a decrease in aerobic metabolism (up to its complete stop), depletion of high-energy intracellular compounds, disruption of cell function and subsequent death. Under hypoxic conditions, the lifespan of a cell depends on energy/oxygen reserves, metabolic needs, and the body's ability to maintain metabolic processes under anaerobic conditions. The period of preservation of function is about one minute for the cerebral cortex, about 5 minutes for the myocardium, about 10 minutes for the liver/kidneys. The critical time after which it is impossible to restore functions is 4-5 times longer than the period of preservation of the function.
Respiratory system. The development of hypoxia stimulates the chemoreceptors of the aortic/carotid bodies, which leads to an increase in the frequency/depth of breathing. Mild hypoxia is often not accompanied by shortness of breath. Loss of consciousness usually occurs without obvious warning signs.
The cardiovascular system. Lack of oxygen increases sympathetic tone, which increases heart rate and cardiac output. In cases of mild, short-term hypoxia, blood pressure usually remains normal. While in the lungs, hypoxia contributes to vasoconstriction and increased pressure in the pulmonary artery.
CNS. It is the most sensitive to hypoxia. Initially, as hypoxia develops, psychomotor retardation and deterioration of cognitive functions are noted. Further, the disorders quickly increase and worsen: anxiety, stupor appear, and when PaO2 levels are below 30-40 mm Hg. Art. stupor develops, coma with a high probability of death.
Complications
In the absence of timely diagnosis and subsequent restorative measures, the patient falls into a vegetative state or prolonged coma. All vital functions are relatively normal, but there is no reaction to external stimuli. The patient loses interest in what is happening, is unable to speak, and is completely detached from others. There is no ability for self-care or conscious movements. Due to associated diseases (infections in places of bedsores, pulmonary pathologies, anorexia, vein thrombosis), death occurs within 1-3 years.
When the root cause of hypoxia is discovered and eliminated, the prognosis looks more favorable. With short-term oxygen starvation, complete recovery and rapid recovery from a coma are possible.
Forecast
The prognosis is determined by the dynamics/character and degree of changes/disturbances in the body’s vital functions, which depends on the type of hypoxia, its severity, rate of development, and state of the body. Thus, in severe fulminant form, hypoxia quickly leads to loss of consciousness, severe disruption of body functions and death of the patient (in case of acute arterial massive blood loss, ventricular fibrillation , cyanide , etc.). Chronic moderate hypoxia (constant/intermittent) is accompanied in most cases by the body's adaptation to hypoxia.
Where is the diagnosis carried out?
A targeted MRI scan can be performed at any diagnostic center that uses high-precision equipment. The Msk-mrt website contains a complete list of clinics distributed across the capital’s districts. When urgently searching for a medical organization, there is a hotline number located at the top of the page. Operators will provide information about the nearest centers, prices for the procedure, sign up for a session, or provide contact information for an institution that accepts emergency patients. When registering for a procedure through the portal, discounts are provided.
List of sources
- Hypoxia. Adaptation, pathogenesis, clinic / Responsible. ed. Yu.L. Shevchenko. - St. Petersburg: Elbi-SPb LLC, 2000. -384 p.
- Kislitsyn A.N. The influence of hypoxia on the human body during high mountain ascents // General. resuscitation. - 2006. - T.II, No. 1. — P. 39-41.
- Lukyanova L.D., Kirova Yu.I., Sukoyan G.V. New information about signaling mechanisms of adaptation to hypoxia and their role in systemic regulation // Pathogenesis. - 2011. - T.9, No. 3. — P. 4-14.
- Chesnokova N.P., Brill G.E., Polutova N.V., Bizenkova M.N. LECTURE 10 HYPOXIA: TYPES, ETIOLOGY, PATHOGENESIS // Scientific Review. Medical Sciences. – 2021. – No. 2. – P. 53-55.
- Molov A.A., Shkhagumov K.Yu., Borukaeva I.Kh., Abazova Z.Kh. Adaptation of the brain and heart to lack of oxygen // Modern problems of science and education. – 2021. – No. 2.