Pulmonary sclerosis is a disease in which lung tissue is replaced by connective tissue. Pulmonologists at the Yusupov Hospital, based on a comprehensive examination, identify the cause of sclerosis of the lung tissue and carry out effective therapy for the disease that caused it.
Pulmonary sclerosis can be local or diffuse. Pathological changes often form in the following diseases or accompany them:
- chronic obstructive pulmonary diseases;
- infectious, viral and fungal diseases of the lungs;
- pneumoconiosis;
- genetically determined lung diseases;
- injuries and consequences of penetrating chest wounds.
If their treatment is ineffective, prerequisites for the development of sclerosis arise in the lung tissue. Among the provoking factors of the disease, heart failure, pulmonary thrombosis, the influence of ionizing radiation, and dysfunction of the immune system should be noted.
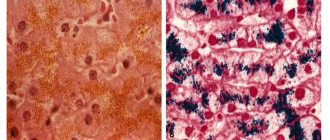
With incomplete resolution of the inflammatory process in the lungs, connective tissue grows, which leads to pneumosclerosis. Similar changes in lung tissue are observed after pulmonary tuberculosis. Diffuse sclerosis develops in patients suffering from Hamman-Rich syndrome. In this case, the lung resembles a honeycomb. With mitral valve stenosis and cardiac left ventricular failure, fluid leaks from the blood vessels, which leads to cardiogenic pulmonary sclerosis.
Pulmonary sclerosis. Symptoms, diagnosis and treatment
As a result of pathomorphological changes in areas of the lungs affected by sclerosis, elasticity and gas exchange are impaired. Local or limited pneumosclerosis develops, which is asymptomatic. On auscultation, harsh breathing and fine wheezing may be heard. It is detected by x-ray methods. The image shows an area of densified lung tissue.
With diffuse changes, the following symptoms occur:
- chest pain;
- progressive shortness of breath;
- cough;
- cyanosis.
During percussion, patients experience a shortening of the percussion sound and limited mobility of the pulmonary edge. Auscultation can be heard fine-bubbly or dry scattered wheezing, weakened vesicular breathing with a hard tint.
With diffuse sclerosis of the lungs, the vascular bed is reduced, pulmonary ventilation is impaired, arterial hypoxemia and chronic respiratory failure develop. Subsequently, emphysema and inflammatory diseases of the lungs develop, and cor pulmonale develops.
To identify and evaluate lesions at the Yusupov Hospital, pulmonologists use research methods:
- radiography and computed tomography or multislice computed tomography of the lungs;
- spirography;
- lung biopsy with morphological verification of the diagnosis.
They are performed using high-tech diagnostic equipment from leading companies in the world.
Pulmonary vascular sclerosis
In the clinical picture of pulmonary artery atherosclerosis, a distinction is made between primary atherosclerosis, which develops in patients with normal blood pressure in the pulmonary circulation, and secondary atherosclerosis, which develops in diseases accompanied by increased blood pressure in the pulmonary circulation. Primary sclerosis of the large branches of the pulmonary artery occurs in people over 40 years of age, and over 70 years of age - very often, but clinically it is usually asymptomatic. Secondary atherosclerosis of the pulmonary artery occurs mainly with increased pressure in the pulmonary circulation, narrowing of the left atrioventricular orifice, patent ductus arteriosus, emphysema, pneumosclerosis, widespread pleural cords, kyphoscoliosis and primary pulmonary hypertension.
The most pronounced clinical picture of atherosclerosis of the pulmonary artery, spreading to its small branches. There is a sharp cyanosis, sometimes black coloring of the skin. A number of authors call sclerosis of the small arteries of the small circle Ayers disease, since Young was the first to emphasize the importance of cyanosis in pulmonary artery sclerosis, calling such patients “black heart patients.”
Cyanosis increases with physical exertion. However, with significant anemia, cyanosis may be absent even with severe atherosclerosis of the pulmonary artery.
Patients complain of shortness of breath, cough, and sometimes hemoptysis. It is characteristic that shortness of breath is weakly expressed in comparison with severe cyanosis. A picture of cor pulmonale develops.
The diagnosis is based primarily on the presence of significant cyanosis, more severe than dyspnea. It is important to recognize the corresponding heart and lung diseases leading to hypertension in the pulmonary circulation. Significant difficulties are presented by differential diagnosis from repeated low-symptomatic embolisms of the pulmonary circulation (attention to varicose veins, thrombophlebitis).
The prognosis is unfavorable. Circulatory disorders of the right ventricular type progress relatively quickly. The addition of various complications (pneumonia, profuse pulmonary hemorrhage, pulmonary artery thrombosis) further aggravates the prognosis.
Prevention requires eliminating (at least partially) the causes that increase pressure in the pulmonary artery. Timely surgical treatment of heart defects is used, and ventilation problems in lung diseases are combated (see Cor pulmonale).
Treatment: gentle regimen, oxygen therapy, drugs that lower pressure in the pulmonary circulation, cardiovascular drugs, anticoagulants to prevent thromboembolic complications.
Pulmonary sclerosis. Treatment and prevention
Doctors at the Yusupov Hospital prescribe small doses of glucocorticoids to patients suffering from pulmonary sclerosis for six months to a year. In the acute period of the disease, their daily dose is 20-30 mg; for maintenance therapy, 5-10 mg of prednisolone is recommended. For bronchitis, bronchiectasis and pneumonia, antibacterial and anti-inflammatory drugs are used. Among the antibiotics, macrolides (azithromycin) are the drugs of choice. To treat pneumosclerosis, doctors also prescribe cephalosporins of the second and third generation. Metronidazole is administered intravenously.
Complex therapy for pulmonary sclerosis includes the following medications:
- expectorants and sputum thinners;
- bronchodilators;
- cardiac glycosides (for circulatory failure);
- vitamins (retinol, α-tocopherol acetate and others).
Non-drug treatment methods are widely used: physiotherapy, oxygen therapy and exercise therapy. For pulmonary sclerosis at the Yusupov Hospital, patients are taught therapeutic and breathing exercises. Outside of exacerbation, sanatorium treatment is recommended. Rarely is there a need for surgery, in which surgeons remove the affected part of the lung. If necessary, this operation is performed in partner clinics.
Prevention of pneumosclerosis consists of timely treatment of colds, hardening, and an active lifestyle. Effective treatment of pneumosclerosis is possible after a comprehensive examination, which is carried out by doctors at the Yusupov Hospital, using modern diagnostic methods. If you have signs of pulmonary sclerosis, call and a consultant doctor will answer all your questions.
Lung lesions in systemic connective tissue diseases
Systemic connective tissue diseases are a group of inflammatory autoimmune diseases of unknown etiology, characterized by multiple lesions of the connective tissue of various organs and systems. The process may involve all parts of the respiratory system. In some cases, lung pathology is associated directly with systemic damage to the connective tissue; in others, it is secondary. Often lesions of different types are combined in one patient, and this multiplicity of lung damage is a common feature of systemic diseases. At the same time, each disease has a unique pulmonary pathology. Systemic connective tissue diseases are progressive in nature and have a long, often severe course. Pulmonary manifestations can occur at any stage or precede the disease by several years. The leading symptoms are shortness of breath, cough and chest pain. The most common syndromes are pleural lesions and interstitial lung diseases. The dysfunction of the immune system characteristic of these diseases, as well as the use of glucocorticosteroids and cytostatic drugs in treatment, increase the body’s susceptibility to infection and contribute to the development of severe complications (pneumonia, sepsis and tuberculosis). Along with the usual pathogens of pneumonia, complications are often caused by opportunistic flora, Mycobacterium tuberculosis, viruses and fungi.
Systemic lupus erythematosus (SLE) is an autoimmune disease characterized by systemic damage to blood vessels of various sizes. SLE is characterized by the presence in the blood serum of high titers of antinuclear factors (ANF), antibodies to native DNA and Smith antigen (Sm-Ag), and low levels of complement.
Compared to other systemic diseases, lung damage in SLE is represented by the widest range of syndromes:
- pleurisy is often bilateral, often combined with pericarditis,
- acute lupus pneumonitis is observed in 1-4% of cases, combined with exudative pleurisy, accompanied by fever, shortness of breath, cough with sputum, hemoptysis (35-60% of cases),
- chronic interstitial pneumonitis,
- damage to interstitial lung tissue occurs in 3-8% of cases,
- alveolar hemorrhages,
- damage to the respiratory muscles (lung shrinkage syndrome),
- bronchiolitis obliterans,
- pulmonary vasculitis with pulmonary hypertension,
- thromboembolism of the branches of the pulmonary artery,
- infectious complications.
The clinical picture of lung damage is observed in 1-6% of cases of SLE; according to multislice computed tomography (MSCT), lung damage is already observed in 30%, and at autopsy - in 70% of cases, SLE is accompanied by lung damage.
The basis of treatment for systemic lupus erythematosus is glucocorticosteroid drugs and immunosuppressive agents. Without treatment, the prognosis is unfavorable; with adequate therapy, remission can be achieved.
Rheumatoid arthritis (RA) is a symmetrical chronic inflammation primarily of the joints of the hands and feet, accompanied by gradual destruction (destruction) of their structure. An immunological feature of RA is the production of autoantibodies of the IgM class to one’s own immunoglobulins (rheumatoid factors), which are found in the blood serum in moderate or high titers. Along with joint damage, 20-30% of patients develop extra-articular manifestations, which include rheumatoid nodules and rheumatoid vasculitis. The most typical manifestations of vasculitis are digital (digital) arteritis, skin ulcers, peripheral neuropathy and vasculitis of internal organs (lungs, heart, kidneys). The risk of death with the development of extra-articular manifestations increases 5 times. Rheumatoid arthritis is characterized by bronchiectasis and bronchiolitis, as well as damage to the pleura, pulmonary vessels (vasculitis, pulmonary hypertension), alveolar hemorrhages, and the development of interstitial lung diseases (ILD). Pleurisy is the most common lung lesion in RA; it is asymptomatic, with a small amount of effusion, and is observed in approximately 25% of patients. In a third of patients, pleurisy is associated with ILD, the course of which in rheumatoid arthritis can be very slow (10 years or more) or fulminant (fulminant, instantaneous). Rheumatoid nodules (RU) are rarely found in the lungs (in 1-2%). In 10-15% of patients, a dangerous complication develops - secondary amyloidosis, including involvement of the lungs. A more frequent development of lymphomas, myeloma and leukemia has been proven against the background of rheumatoid arthritis.
Systemic scleroderma (progressive systemic sclerosis) is a group of diseases in the early stages of which microcirculatory disorders and inflammation prevail, gradually leading to generalized fibrosis (sclerosis). Typical autoimmune disorders in systemic scleroderma are the formation of anticentromere antibodies and antibodies to the topoisomerase 1 antigen (Scl-70). The disease is characterized by a variety of appearances, the most striking of which is thickening of the skin. The diffuse form of scleroderma is characterized by acute development and rapid progression of generalized fibrosis of the skin and internal organs (heart, lungs, kidneys). A relatively benign limited form debuts with Raynaud's phenomenon (syndrome), skin changes are limited in nature, progress slowly and are accompanied by vascular ischemic disorders. Lung damage with scleroderma occurs more often than with other systemic diseases, in men more often than in women. Lung pathology with multislice computed tomography (MSCT) in patients with systemic scleroderma is observed in 80-90%. The most common diseases are interstitial lung disease (ILD) and pulmonary hypertension (PH). The cause of PH in 12-15% may also be fibrous lesions of the left parts of the heart (valve, myocardium). Pulmonary hypertension is more often associated with a limited form of the disease and is detected in patients with a long history of ILD with a diffuse form. Infectious complications (pneumonia, abscess formation) occur less frequently than with other systemic diseases. The risk of developing lung cancer against the background of systemic scleroderma increases 3-5 times.
Idiopathic inflammatory myopathies are a group of diseases whose clinical manifestations are based on inflammation of striated muscles (polymyositis, dermatomyositis, juvenile dermatomyositis, etc.). Immunological markers are myositis-specific antibodies directed to cytoplasmic proteins and ribonucleic acids. The most common antibodies are antibodies to tRNA aminoacyl synthetases (Jo-1, etc.).
Muscle damage is manifested by symmetrical weakness of the proximal (located closer to the body) muscle groups of the upper and lower extremities and muscles involved in neck flexion, which is manifested by difficulty in rising from a low chair; when boarding a vehicle; when washing and combing your hair. Characteristic damage to the muscles of the pharynx, larynx and upper third of the esophagus (dysphonia, dysphagia). Intraorgan manifestations are varied, the most common being damage to the respiratory system. Typical for myopathies is damage to the intercostal muscles and diaphragm, which leads to difficulty breathing and shortness of breath. Pneumonia complicates the course of polymyositis and dermatomyositis in 30-50% of patients. The leading role in its development is played by aspiration of food associated with damage to the muscles of the pharynx and the upper third of the esophagus (aspiration syndrome). The most severe lung disease is interstitial disease (ILD), the symptoms of which precede symptoms of muscle damage in 10% of cases.