Among all cardiac patients, supraventricular tachycardia occurs in 6-10% of cases. This pathology in itself does not cause concern, but in combination with organic heart disease it can contribute to the development of serious hemodynamic disorders.
Supraventricular tachycardia (SVT) belongs to a general group of arrhythmias and is often associated with diseases of the cardiovascular system. In rare cases, primary SVT occurs, which is difficult to treat with medication. Depending on the location of the pathological focus, four types of supraventricular tachycardia are distinguished, among which in 6-10% of cases supraventricular tachycardia of the re-entry type occurs.
SVT is also known as atrial tachycardia, since ectopic foci in this type of arrhythmia are localized supraventricularly, that is, in the atria.
It is quite difficult to distinguish between the types of SVT, since they have many similarities. However, with the help of instrumental diagnostic methods and a thorough objective examination of the patient, it is possible to make a correct diagnosis and prescribe appropriate treatment.
Video Tachycardia
What is supraventricular tachycardia?
Supraventricular tachycardia (SVT) is a type of heart rhythm disorder (arrhythmia) or heart palpitations in which the heart beats too quickly.
A normal heartbeat is caused by an electrical impulse passing through the heart. The electrical impulse originates in the sinus node (also called the sinoatrial node), most often located in the upper part of the right atrium. Electrical signals travel through the heart tissue to the lower chambers of the heart, called the ventricles. An electrical impulse causes the upper chambers (atria) and lower chambers (ventricles) of the heart to beat regularly and consistently.
In supraventricular tachycardia, a series of early beats in the atrium accelerates the heart rate. A fast heartbeat (arrhythmia) prevents the ventricles from filling with enough blood because the electrical signal causes the heart to beat too quickly.
If a person has SVT, the heart may beat 140 to 250 beats per minute, when it normally beats 60 to 100 times per minute (at rest).
Causes of supraventricular tachycardia
Most people with supraventricular tachycardia do not have any serious heart problems or health conditions that lead to it.
SVT can be caused by factors such as:
- taking any types of medications;
- drinking large amounts of alcohol;
- caffeine;
- smoking;
- use of illegal substances such as cocaine.
However, some people experience supraventricular tachycardia (SVT) because there is an extra electrical connection in the heart that they are born with. This is called Wolff-Parkinson-White syndrome (WPW syndrome).
Other factors that may increase the risk of SVT include:
- cardiovascular diseases (cardiomyopathy);
- cardiac ischemia;
- heart surgery;
- hyperfunction of the thyroid gland (hyperthyroidism);
- lung disease such as chronic obstructive pulmonary disease (COPD);
- heart valve disease;
- heart problems that have been present since birth (congenital heart disease).
Clinical variants and incidence of supraventricular tachycardias in children
Supraventricular (supraventricular) tachycardias (SVT) account for 95% of all tachycardias in children and are often paroxysmal in nature. In most cases, SVTs are not life-threatening rhythm disturbances, but may be accompanied by complaints of a sharp deterioration in health and have a pronounced clinical picture.
The term “supraventricular tachycardia” refers to three or more consecutive heart contractions with a frequency exceeding the upper limit of the age norm in children and more than 100 beats per minute in adults, if the participation of the atria or atrioventricular (AV) junction is required for the occurrence and maintenance of tachycardia.
SVT includes tachycardias that occur above the bifurcation of the His bundle, namely in the sinus node, atrial myocardium, AV junction, trunk of the His bundle, emanating from the mouths of the vena cava, pulmonary veins, and also associated with additional conduction pathways.
Supraventricular tachycardia is a common form of cardiac arrhythmia in children and adults. The prevalence of paroxysmal SVT in the general population is 2.25 cases per 1000 people, with 35 new cases occurring per year per 100,000 population [1]. The incidence of SVT in children, according to various authors, varies significantly and ranges from 1 case in 25,000 children to 1 case in 250 children [2, 3].
In practice, it is convenient to use the clinical and electrophysiological classification of SVT, which systematizes individual nosological forms of tachycardias, indicating their localization, electrophysiological mechanism, various subtypes and variants of the clinical course [4].
Clinical and electrophysiological classification of supraventricular tachycardias in children:
I. Clinical options for SVT:
1. Paroxysmal tachycardia:
- stable (duration of attack 30 s or more);
- unstable (duration of attack less than 30 s).
2. Chronic tachycardia:
- constant;
- permanently returnable.
II. Clinical and electrophysiological types of SVT:
1. Sinus tachycardia:
- sinus tachycardia (functional);
- chronic sinus tachycardia;
- sinoatrial reciprocal tachycardia.
2. Atrial tachycardia:
- focal (focal) atrial tachycardia;
- multifocal or chaotic atrial tachycardia;
- incisional atrial tachycardia;
- atrial flutter;
- atrial fibrillation.
3. Tachycardia from the AV junction:
- atrioventricular nodal reciprocal tachycardia: - typical; - atypical;
- focal (focal) tachycardia from the AV junction: - postoperative; - congenital; - “adult” form.
4. Tachycardia with the participation of accessory pathways (Wolf–Parkinson–White syndrome (WPW), atriofascicular tract and other accessory pathways (ADP)):
- paroxysmal orthodromic AV reciprocal tachycardia with the participation of AP;
- chronic orthodromic AV reciprocal tachycardia with the participation of “slow” AP;
- paroxysmal antidromic AV reciprocal tachycardia with the participation of AP;
- paroxysmal AV reciprocal tachycardia with pre-excitation (involving several APs).
According to the nature of the course, tachycardias are divided into paroxysmal and chronic. Paroxysmal tachycardia has a sudden onset and end of an attack. Attacks of tachycardia are considered stable if they last more than 30 seconds, and unstable if their duration is less than 30 seconds. The clinical picture of paroxysmal tachycardia is quite diverse. In children of the first year of life, during an attack of tachycardia, anxiety, lethargy, refusal to feed, sweating during feeding, and pallor may be observed. In young children, attacks of tachycardia may be accompanied by pallor, weakness, sweating, drowsiness, and chest pain. In addition, children quite often emotionally and figuratively describe attacks, for example, as “heart in the tummy”, “jumping heart”, etc. School-age children can usually talk about all the clinical manifestations of an attack of tachycardia. Often attacks of tachycardia are provoked by physical and emotional stress, but they can also occur at rest. When asked about the heart rate during an attack of tachycardia, children and their parents usually answer that the pulse “cannot be counted”, “cannot be counted”. Sometimes attacks of tachycardia occur with a pronounced clinical picture, accompanied by weakness, dizziness, darkening of the eyes, syncope, and neurological symptoms. Loss of consciousness occurs in 10–15% of children with SVT, usually immediately after the onset of a paroxysm of tachycardia or during a long pause in the rhythm after its cessation.
Chronic tachycardia does not have an acute beginning and end of the attack; it drags on for a long time and can last for years. Chronic tachycardias are divided into constant (continuous) and constant-recurrent (continuously recurrent). Tachycardia is said to be permanent if it accounts for most of the time of day and represents a continuous tachycardic chain. With the constantly recurrent type of tachycardia, its circuits are interrupted by periods of sinus rhythm, but tachycardia can also occupy a significant portion of the day. This division of chronic tachycardia into two forms is somewhat arbitrary, but has a certain clinical significance, since the more time of day the tachycardia occupies and the higher the heart rate, the higher the risk of the child developing secondary arrhythmogenic cardiomyopathy and progressive heart failure. Quite often, chronic forms of SVT occur without distinct symptoms and are diagnosed after the first signs of heart failure appear.
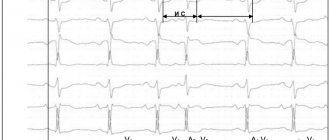
In most cases with SVT, the QRS complexes are narrow, but with aberrant impulse conduction they can widen. The heart rate (HR) during tachycardia depends on the age of the children. In newborns and children of the first years of life, heart rate during paroxysmal tachycardia is usually 220–300 beats/min, and in older children it is 180–250 beats/min. In chronic forms of tachycardia, heart rate is usually somewhat lower and amounts to 200–250 beats/min in children of the first years of life and 150–200 beats/min in older ages.
Most often, SVT must be differentiated from functional sinus tachycardia, which is usually a normal physiological response to physical and emotional stress due to an increase in sympathetic influences on the heart. At the same time, sinus tachycardia can signal serious illnesses. It is a symptom and/or compensatory mechanism of the following pathological conditions: fever, arterial hypotension, anemia, hypovolemia, which can be the result of infection, malignant processes, myocardial ischemia, congestive heart failure, pulmonary embolism, shock, thyrotoxicosis and other conditions. It is known that the heart rate has a direct relationship with body temperature; for example, when the body temperature of a child older than two months increases by 1 °C, the heart rate increases by 9.6 beats/min [5]. Sinus tachycardia is provoked by various stimulants (caffeine, alcohol, nicotine), the use of sympathomimetic, anticholinergic, some antihypertensive, hormonal and psychotropic drugs, as well as a number of toxic and narcotic substances (amphetamines, cocaine, ecstasy, etc.). Functional sinus tachycardia usually does not require special treatment. The disappearance or elimination of the cause of sinus tachycardia in most cases leads to the restoration of the normal frequency of sinus rhythm. Sometimes children experience chronic sinus tachycardia, in which the sinus rate does not correspond to the level of physical, emotional, pharmacological or pathological influence. Sinoatrial reciprocal tachycardia is extremely rarely recorded, usually having an unstable paroxysmal course.
Atrial tachycardia in children is often chronic and difficult to treat with medication, can lead to congestive heart failure, and is the most common cause of secondary arrhythmogenic cardiomyopathy. Therefore, despite the relatively low incidence, atrial tachycardia is a serious problem in pediatric arrhythmology. The most common type of atrial tachycardia is focal (ectopic) atrial tachycardia, which accounts for 15% of all SVT in children under one year of age and 10% in children aged one to five years [6].
Focal atrial tachycardia is a relatively regular atrial rhythm with a rate above the upper normal for age, usually between 120 and 300 bpm. In this case, frequent P waves of non-sinus origin, located in front of the QRS complexes, are recorded on the ECG. The morphology of P waves depends on the location of the tachycardia focus. With the simultaneous functioning of several atrial rhythm sources, multifocal (multifocal) atrial tachycardia occurs. This rather rare form of tachycardia is well known as “chaotic atrial tachycardia”. Chaotic atrial tachycardia is an irregular atrial rhythm with a continuously varying frequency from 100 to 400 beats per minute with variable AV conduction of atrial impulses with a frequency of an also irregular ventricular rhythm of 100–250 beats/min. Atrial flutter is a regular, regular atrial rhythm, usually between 250 and 450 beats per minute. With typical atrial flutter on the ECG, instead of P waves, “sawtooth” F waves are recorded with the absence of an isoline between them and with a maximum amplitude in leads II, III and aVF. Incisional (postoperative) atrial tachycardia occurs in 10–30% of children after correction of congenital heart disease (CHD), during which surgical manipulations were performed in the atria. Incisional tachycardias can appear both in the early postoperative period and several years after surgery. They are a serious problem and largely determine mortality after cardiac surgery. Quite rarely, children experience atrial fibrillation, which is chaotic electrical activity of the atria with a frequency of 300–700 per minute, while f waves of different amplitudes and configurations are recorded on the ECG without an isoline between them. Atrial fibrillation leads to a decrease in cardiac output due to loss of atrial systole and arrhythmia itself. Another serious danger of atrial fibrillation is the risk of thromboembolic complications.
The AV junction is associated with the occurrence of two tachycardias that are different in electrophysiological mechanism and clinical course: AV nodal reciprocal tachycardia and focal tachycardia from the AV junction. Paroxysmal AV nodal reentrant tachycardia accounts for 13–23% of all SVTs [2, 6]. Moreover, the incidence of this form of tachycardia increases with age - from isolated cases in children under two years of age to 31% of all SVT in adolescents [6, 7]. The occurrence of this tachycardia is based on the division of the AV connection into zones of fast and slow impulse conduction, which are called the “fast” and “slow” paths of the AV connection. These pathways form a re-entry circle, and depending on the direction of movement of the impulse, typical and atypical forms of AV nodal reciprocal tachycardia are distinguished. Focal tachycardia from the AV junction is associated with the occurrence of foci of pathological automatism or trigger activity in the area of the AV junction and is quite rare.
The most common type of SVT in children in all age groups is paroxysmal AV reentrant tachycardia involving an accessory AV junction (AVJ), which is a clinical manifestation of WPW syndrome. In half of the cases, this type of tachycardia occurs in childhood; it accounts for up to 80% of all SVT in children under one year of age and 65–70% in older age [6, 8].
In orthodromic AV reciprocal tachycardia, the impulse is conducted anterogradely (from the atria to the ventricles) through the AV node, and retrogradely (from the ventricles to the atria) returns through the AP. The ECG shows tachycardia with narrow QRS complexes. In children of the first year of life, the heart rate during tachycardia is usually 260–300 beats/min, in adolescents it is lower - 180–220 beats/min. Attacks of tachycardia can begin either at rest or be associated with physical and emotional stress. The beginning, like the end of the attack, is always sudden. The clinical picture is determined by the age of the child, heart rate, and duration of attacks. In a more rare variant, antidromic AV reciprocal tachycardia, the impulse is conducted anterogradely along the AP and returns through the AV node. In this case, the ECG shows tachycardia with wide, deformed QRS complexes.
We analyzed the incidence of various types of tachycardia in 525 children with SVT examined during the period 1993–2010. in the department of surgical treatment of complex cardiac arrhythmias and cardiac pacing in St. Petersburg State Healthcare Institution “City Clinical Hospital No. 31” (table).
Pathological forms of sinus tachycardia were diagnosed in 25 (4.7%) children, atrial tachycardia - in 75 (14.3%) children, tachycardia from the AV junction - in 163 (31.1%) children, tachycardia involving the APP - in 262 (49.9%) children. According to the nature of the course, 445 (84.8%) children had paroxysmal tachycardia, 80 (16.2%) had chronic tachycardia. It should be noted that functional sinus tachycardia is included in the classification of SVT, but is not taken into account when analyzing the structure of SVT due to the absolute prevalence over other forms of tachycardia, because it is observed in every child with normal sinus node function, for example, during physical activity or emotional stress .
257 (48.9%) children had WPW syndrome and its clinical manifestation was paroxysmal AV reciprocal tachycardia with the participation of an additional AV connection.
157 (29.9%) children were diagnosed with AV nodal reentrant tachycardia: 149 had the typical form, 8 had variants of the atypical form. 6 (1.1%) children had chronic focal tachycardia from the AV junction.
In 75 (14.3%) children, various types of atrial tachycardia were observed: chronic focal atrial tachycardia in 36 children, paroxysmal focal atrial tachycardia - in 15 children, incisional atrial tachycardia - in 2 children, atrial fibrillation - in 11 children, atrial flutter - in 9 children, chaotic atrial tachycardia - in 2 children. 2 (0.4%) children had sinoatrial reentrant tachycardia, 23 (4.4%) had chronic sinus tachycardia.
Considering that in St. Petersburg the overwhelming number of children with tachycardia were examined in our center, we can imagine an approximate epidemiological situation in the city according to SVT. 800 thousand children live in St. Petersburg. Approximately 32 children presented with new cases of SVT per year, which amounted to 1 case per 25,000 children.
From 2000 to 2010, during each year, from 14 to 28 children with WPW syndrome (average 19.4 ± 4.2 children) and from 8 to 16 children with paroxysmal AV nodal reentrant tachycardia (average 10.7 ± 2.8 children). Based on the child population of St. Petersburg, an average of 2 new cases of WPW syndrome and 1 case of paroxysmal AV nodal reentrant tachycardia per 80,000 children were detected per year.
Thus, supraventricular tachycardias in children have many clinical and electrophysiological variants. The first place in terms of frequency of occurrence is occupied by WPW syndrome, the second place is paroxysmal AV nodal reciprocal tachycardia, the third place is atrial tachycardia. According to our study, supraventricular tachycardias in children had the following structure: according to localization of occurrence: 4.7% - sinus tachycardias, 14.3% - atrial tachycardias, 31.1% - tachycardias from the AV junction, 49.9% - tachycardias with participation of the DPP; according to the clinical course: 84.8% - paroxysmal tachycardia, 15.2% - chronic tachycardia. Paroxysmal AV reciprocal tachycardia with the participation of an additional AV connection (WPW syndrome) accounted for 48.9% of all SVTs and 57.8% of paroxysmal forms of SVT. Systematization of various forms of tachycardia in children is of great clinical importance, as it allows one to navigate their diversity and helps to make a consistent differential diagnosis. Accurate verification of the type of tachycardia plays a decisive role in predicting the course of the disease, choosing antiarrhythmic therapy and assessing the effectiveness and safety of catheter ablation.
Literature
- Orejarena LA, Vidaillet HJ, DeStefano F. et al. Paroxysmal supraventricular tachycardia in general population // J. Am. Coll. Cardiol. 1998. Vol. 31, No. 1. P. 150–157.
- Ludomirsky A. Garson A. Supraventricular tachycardia // Pediatric Arrythmias: Electrophysiology and Pacing. Ed. by PC Gillette, A. Garson. Philadelphia, WB Saunders, 1990, pp. 380–426.
- Bauersfeld U., Pfammatter J.-P., Jaeggi E. Treatment of supraventricular tachycardias in the new millennium - drugs or radiofrequency catheter ablation? //Eur. J. Pediatr. 2001. V. 160. P. 1–9.
- Kruchina T.K., Vasichkina E.S., Egorov D.F. Supraventricular tachycardia in children: educational manual. Ed. prof. G. A. Novik. St. Petersburg: SPbGPMA, 2011. 60 p.
- Hanna C., Greenes D. How much tachycardia in infants can be attributed to fever? //Ann. Emerg. Med. 2004. V. 43. P. 699–705.
- Ko JK, Deal BJ, Strasburger JF, Benson DW Supraventricular tachycardia mechanisms and their age distribution in pediatric patients // Am. J. Cardiol. 1992. Vol. 69, No. 12. P. 1028–32.
- Kruchina T.K., Egorov D.F., Gordeev O.L. et al. Features of the clinical course of paroxysmal atrioventricular nodal reciprocal tachycardia in children // Bulletin of Arrhythmology. 2004. No. 35, appendix. B, p. 236–239.
- Rodriguez L.-M., de Chillou C., Schlapfer J. et al. Age at onset and gender of patients with different types of supraventricular tachycardias // Am. J. Cardiol. 1992. Vol. 70. P. 1213–1215.
T. K. Kruchina *, **, Candidate of Medical Sciences G. A. Novik ***, Doctor of Medical Sciences, Professor D. F. Egorov *, ****, Doctor of Medical Sciences, Professor
*Research Laboratory of Surgery, **St. Petersburg State Healthcare Institution “City Clinical Hospital No. 31”, ***St. Petersburg State Pediatric Medical Academy, ****National Research Center of St. Petersburg State Medical University named after. Academician I. P. Pavlov, St. Petersburg
Contact information for authors for correspondence
Signs and symptoms of supraventricular tachycardia
Supraventricular tachycardia does not always cause symptoms. If you have any symptoms, they may come and go and their duration will vary. The duration can be anything from several minutes to several months. Often supraventricular tachycardia begins and then ends abruptly.
During SVT, a person may experience:
- palpitations (an unpleasant sensation caused by a strong and fast beating of the heart);
- dizziness;
- chest pain;
- syncope, which rarely occurs with SVT.
Symptoms of heart failure may also occur if an episode of SVT lasts more than 24 hours before the patient receives medical attention. This is especially common in newborns and infants who cannot convey the sensation of a heartbeat.
Symptoms of SVT in children are subtle and often associated with poor feeding, vomiting, or a general decrease in the child's activity level and alertness.
Supraventricular tachycardia almost never causes sudden death. However, if you experience any of the symptoms, be sure to contact your GP.
Expert advice
In the prevention of VT attacks, eliminating the cause plays an important role. Therefore, I strongly recommend that my patients quit smoking, limit their consumption of coffee and alcohol, and avoid extreme stress and excessive physical activity. It is also necessary to conduct an examination to identify a disease that could provoke the development of arrhythmia, and its proper treatment (IHD, CHF, diffuse toxic goiter, etc.). It is important to remember that tachycardia is either a normal reaction of the body to stress or a symptom of heart damage. For this, the fact of observing yourself and your rhythm is important. If you notice an increase in the frequency of attacks, make an appointment with your doctor, first noting for yourself in what conditions tachycardia appears.
In cases where there is no obvious connection, the doctor will recommend that you undergo examinations. The first step in solving the problem of pathological tachycardia will be to get rid of any factors that can cause it in a healthy person, that is, stress. Stay calm and take care of yourself is important advice in treating arrhythmias.
Diagnosis of SVT
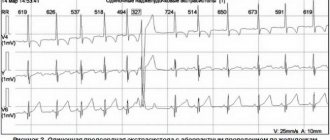
Supraventricular tachycardia is suspected when a doctor or nurse notes a rapid heart rate (>200) during an attack. To confirm the diagnosis, your doctor may perform an electrocardiogram (ECG). An electrocardiogram is a test that records the electrical activity of the heart. An echocardiogram or "echo" may also be performed in the cardiologist's office. This is a type of ultrasound that takes dynamic pictures of the heart.
An ECG, echocardiogram, and physical examination are usually normal if performed after the tachycardia (rapid heartbeat) has stopped, so it is important to obtain an ECG during symptoms. If this is not possible, the patient can be sent home with a Holter monitor or other heart monitor that can be used to continuously record the heart rhythm for at least 24 hours. An accurate ECG will allow you to make the correct diagnosis and select the appropriate treatment.
Your doctor may also refer you or your child to an electrophysiologist, a cardiologist who has additional education and training in diagnosing and treating abnormal heart rhythms.
Treatment of supraventricular tachycardia
Treatment of supraventricular tachycardia is aimed at controlling heart rhythm and heart rate. What treatment is prescribed will depend on the symptoms. No treatment may be required at all ; Sometimes the symptoms stop on their own.
If SVT is caused by medication, your doctor can check for it. If SVT is caused by an underlying health condition (disease), the doctor will focus treatment on that.
Vagal maneuvers
Older people may learn to perform vagal maneuvers in an attempt to slow or stop an episode of heart palpitations. Vagal maneuvers may include:
- holding and resuming breathing (Valsalva maneuver);
- immersion of the face in ice water (immersion reflex);
- cough.
Valsalva maneuver - involves you lying on your back and blowing into a syringe for 15 seconds. This increases pressure in the chest, which causes the heart rate to slow.
Drug treatment
If symptoms appear suddenly, your doctor may prescribe antiarrhythmic drugs , either in pill form or intravenously. They are aimed at returning the heart rate to normal. There are different types of medications that can do this, including a beta blocker , calcium channel blockers , and other antiarrhythmic drugs such as adenosine .
Ablation
While children with supraventricular tachycardia usually outgrow the arrhythmia, adults usually do not. Depending on a person's age and the severity and frequency of symptoms, a cardiologist may recommend a catheter ablation procedure to permanently eliminate SVT.
During ablation, several large IVs (small plastic tubes) are inserted into the major blood vessels in the legs. Catheters (thin tubes) are then passed through them and pushed through the veins to the heart. Electrical signals from the catheters help detect additional electrical connections, which can then be disrupted and removed. The procedure takes several hours and most patients return home the same day.
After successful ablation treatment, the person should not have any episodes of supraventricular tachycardia.
If a child has SVT, he or she may need to see a cardiologist frequently. Children with supraventricular tachycardia should see a cardiologist once or twice a year for medications and a follow-up electrocardiogram. However, older children and adults who have had a successful ablation procedure may not require ongoing follow-up.
First aid
An attack of tachycardia may go away on its own or you can get rid of it at home without contacting a specialist.
However, a significant deterioration in the patient’s health status necessitates urgent qualified medical care.
Self-relief of attacks must be carried out with caution to avoid aggravation of the patient’s condition
Relief from attacks is easily eliminated with the help of vagal tests - mechanical methods of influencing the vagus nerve, causing a reflex reaction of other organs and systems and reducing the intensity of heart contractions.
If tachycardia is detected, which does not threaten the patient’s health and the attacks of which can be stopped without the intervention of a specialist, the doctor explains the principle of performing vagal tests.
During the procedure you should:
- Massage the carotid sinus.
- Press on closed eyes.
- Hold your breath and lower your face into the water containing ice cubes.
- Strain with an accompanying deep exhalation.
- Perform squats while straining.
- Induce artificial vomiting and cough reflexes (by pressing on the root of the tongue).
The duration of the procedure depends on the time the patient reaches a normal state and can last from 30 seconds to several minutes. If necessary, the possibility of repeating them is not excluded.
To date, effects on the carotid node and eyes are rarely used.
The use of these methods is prohibited when:
- severe pain in the sternum;
- shortness of breath;
- a sharp feeling of weakness;
- low blood pressure;
- unconscious state;
- paleness or cyanosis of the skin;
- involuntary muscle contraction;
- impaired sensitivity and motor activity of the arms or legs.
The above manifestations may indicate serious illnesses (heart attacks, stroke, pulmonary edema) and require an immediate call to the ambulance.
Vagal tests are also contraindicated if you suspect:
- pulmonary embolism;
- acute cerebral circulatory disorder;
- acute coronary syndrome;
- damage to the aorta by atherosclerosis.
As a result, after the procedures, the symptoms of the pathology should disappear and the heart rhythm should be restored.
To eliminate attacks, you can also resort to sedatives (tincture of motherwort or valerian, valocordin, diazepam) in the dosage specified in the instructions for the drug.
Self-relief from attacks of supraventricular tachycardia with the help of medications should be carried out under the supervision of a physician.
The patient is subject to hospitalization if:
- loss of consciousness;
- hemodynamic abnormalities;
- manifestations of ischemia.
If an attack of tachycardia occurred for the first time and was stopped without medical assistance, in the future you should undergo the necessary examinations and exclude the possibility of the occurrence of any diseases.
Prognosis of supraventricular tachycardia
The prognosis is determined by the type of supraventricular tachycardia, the disease that caused it, the frequency and duration of attacks, the presence or absence of complications during episodes of attack, the state of the contractile myocardium (severe myocardial damage predisposes to the development of acute cardiac or cardiovascular failure, sudden arrhythmic death, myocardial ischemia, etc. .P.).
There is usually a small risk of sudden death only in a certain type of SVT, called Wolff-Parkinson-White syndrome.
The prognosis for patients with “primary” SVT is usually favorable: most patients retain full or partial ability to work for many years or decades, although complete spontaneous recovery is rare.
Symptoms
Supraventricular tachycardia is always felt subjectively by a person and is accompanied by anxiety. He becomes anxious, constantly listens to what is happening inside, and withdraws from the external environment.
Typical symptoms:
- increased excitability and fatigue;
- dizziness;
- causeless headaches, as well as in the legs and stomach.
External signs are also characteristic:
- asthenicity;
- underweight;
- pale skin.
Often the cause of disruption of the cardiovascular system is vegetative-vascular dystonia. In children with chronic tachycardia, in more than half of the cases, neurological problems were diagnosed: causeless headaches, phobias, stuttering, nervous tics, etc. They are more anxious, aggressive, and have an unstable emotional state. This creates obstacles for their adaptation in society. Even ordinary life situations, such as going to the doctor or meeting new people, cause them acute discomfort.
Advanced chronic tachycardia causes a decrease in the contractility of the heart muscle and subsequent heart failure. There are different versions about the causes of this disease. One of the authoritative ones is organic changes in the heart muscle. They may be preceded by the following events:
- intoxication;
- myocardial infarction;
- violation of coronary circulation;
- arterial hypertension;
- rheumatism; heart defects, coronary disease, myocarditis;
- undergone heart surgery.
Acute intoxications can become the beginning of the development of chronic SVT, although they initially cause its paroxysmal form. It manifests itself in one or more symptoms. These include:
- hand trembling;
- confused speech;
- temporary paralysis;
- fainting or conditions close to it.