Cardiac surgery for mitral valve defects
Return to section:
Cardiac surgery department
The mitral valve is located between the left atrium and the left ventricle.
Normally, it opens in diastole, allowing arterial blood to pass from the left atrium into the left ventricle, and closes in systole under the influence of blood pressure during contraction of the left ventricle, preventing the reverse flow of blood from the left ventricle into the left atrium.
There are 3 types of mitral valve defects:
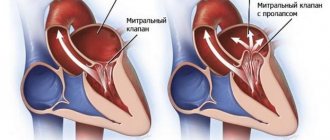
1) Mitral insufficiency. With pathology of connective tissue or changes in the heart muscle, a disturbance in the structure of the mitral valve occurs, which leads to “bending” of its valves into the cavity of the left atrium during contraction of the left ventricle, part of the blood flows back into the atrium.
2) Mitral stenosis. Due to infectious diseases such as rheumatism, the MV narrows, which leads to disruption of the flow of blood from the left atrium to the left ventricle.
3) Combined MV defect (insufficiency + stenosis).
Currently, in modern cardiac surgery for mitral valve defects, reconstructive (valve-preserving) operations are performed, as well as operations to replace (prosthetics) valves with a mechanical or biological prosthesis. Reconstructive operations are performed both for stenosis and mitral valve insufficiency.
Reconstructive surgeries
| Fig. 1 . Mitral annuloplasty on a support ring. |
An example is annuloplasty, which involves restoring the function of the affected valve using a rigid or elastic support ring.
It is fixed to the walls of the heart at the level of the opening connecting the atrium to the ventricle. As a result of sewing in such a support ring, the diameter of the atrioventricular orifice decreases, which ensures more complete closure of the valves and normalizes intracardiac blood flow.
Another option for reconstructive surgery on heart valves is surgery using various suture techniques.
During this procedure, the surgeon performs plastic surgery on the valve leaflet tissue, removes calcified deposits, or restores the structure of the altered chordae tendineae, which control the movement of the leaflets.
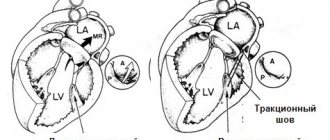
Rice. 2 .
Suture plasty of the mitral valve. A, B – resection of the altered portion of the posterior mitral valve leaflet; C, D, E – stages of eliminating the gap in the valve.
MK prosthetics.
A radical method of treating the mitral valve is its replacement. Modern mechanical (artificial heart valves) and biological valves are used.
| Mechanical prosthesis MK | Biological prosthesis MK |
Fig.3 . Mechanical (left) and biological (right) mitral valve.
In the case of pronounced morphological changes in the patient’s own valve, when it is no longer possible to preserve it, the valve is removed followed by prosthetics. Surgical replacement of the mitral valve is performed on a non-functioning heart using a heart-lung machine.
Mechanical (artificial heart valves) are very reliable, last a lifetime and do not need to be replaced, but require constant use of special medications to reduce blood clotting.
Biological valves (of animal or human origin) can deteriorate over time, and the lifespan of these valves is highly dependent on the age of the patient and his concomitant diseases. With age, the process of destruction of biological valves slows down greatly. The decision about which valve is the best option in a particular situation is made individually before surgery in a mandatory conversation between the surgeon and the patient.
Technical progress in cardiac surgery, namely the introduction into daily surgical practice of new instruments that make it possible to modify surgical approaches to the heart, inevitably puts forward the goal of performing them with minimal intraoperative trauma for the patient.
Choosing the most rational access to various parts of the heart is one of the necessary conditions for solving this problem.
Online access should ensure the solution of the main tasks:
- provide the surgeon with sufficient space for ease of manipulation in the surgical area;
- surgical access should preferably be less traumatic for the patient.
The traditional surgical approach to the heart is a longitudinal median sternotomy (Fig. 4).
| Diagram of median sternotomy | Type of postoperative scar |
On the one hand, it allows the surgeon to perform the necessary surgical procedures on the heart for various forms of its pathology and is as convenient as possible for connecting a heart-lung machine.
On the other hand, this access may not be optimal. This is due to a number of reasons:
- Greater trauma, the integrity of the chest is compromised, which requires a longer period of healing of the postoperative wound.
- High risk of postoperative complications (sternal instability). These complications are especially dangerous in elderly patients.
- Questionable cosmetic effect.
Fig.5 . View of the surgical field during reconstructive interventions on the mitral valve from a minimally invasive approach to the heart.
All cardiac surgeons will agree that mitral valve reconstruction through a minimally invasive approach (right minithoracotomy) should be performed on the patient with the same skill and quality as when performing operations through a median full sternotomy.
Correction of the mitral valve from a right-sided minithoracotomy is performed in the 4th intercostal space, 6 cm long, in the projection of the 4th intercostal space on the right.
| Scheme for performing a right minithoracotomy | Type of postoperative scar |
Benefits of Minimally Invasive Valve Surgery
- Less pain syndrome. Since access to the heart is through a right lateral minithoracotomy, where the length of the skin incision is about 7 cm, the frame function of the chest is also preserved, i.e. its integrity is not compromised than with the traditional approach - median sternotomy, where the length of the skin incision is about 20 cm, and to perform surgical manipulation of the heart it is necessary to saw the sternum along the midline.
- Reduced risk of complications. Since the chest wall maintains its integrity, the risk of developing complications such as postoperative sternal instability is eliminated.
- Faster recovery and return to normal activities. Less surgical trauma and preservation of the frame function of the chest after minithoracotomy allows for early activation and rehabilitation of patients, which helps reduce the length of hospital treatment.
- The scar is less noticeable. Most patients are very satisfied with the cosmetic results after surgery.
← Back
Mitral stenosis
This defect is characterized by a narrowing of the valve opening. The “critical” value of the area is 1–1.5 cm. The smaller the area, the more symptoms of the disease.
Mitral stenosis can lead to
- rheumatic fever;
— calcium deposits on the valve leaflets;
— connective tissue diseases (Marfan syndrome);
— myxoma (benign tumor) of the left atrium.
Rice.
1 - tricuspid valve;
2 - aortic valve;
3 - pulmonary valve;
4 - mitral valve;
5 - stenosis of the mitral valve opening.
Through the narrowed mitral orifice, blood from the left atrium to the left ventricle passes with difficulty: the atrium has to work harder and harder to push the blood. This increased work leads to an enlargement of the atrium. Blood stagnation in the lungs gradually develops, and over time the right parts of the heart also enlarge. An enlarged heart works worse, and heart failure develops.
Symptoms
At the initial stages, stenosis does not make itself felt. People feel completely healthy and can perform significant physical activity. As the defect progresses, shortness of breath (blood stagnation in the lungs) appears, at first only when moving, later at rest. Around the same time, a cough with a small amount of sputum may appear; Sometimes hemoptysis is observed. There is unmotivated weakness, rapid fatigue, a feeling of interruptions in the heart, diffuse chest pain. In advanced cases, an enlarged heart can put pressure on the esophagus and larynx - the voice changes and swallowing is impaired.
Diagnostics
People with mitral stenosis are characterized by a specific appearance: a pale face, sharply defined rosy cheeks with a bluish tint, cyanosis of the lips and tip of the nose. On the anterior chest there is a cardiac hump - this is how the enlarged heart sticks out. The pulse is not the same in the arms. With a thorough examination by a doctor, as a rule, there is no doubt about the diagnosis, because heart sounds and changes in clinical and laboratory data are specific changes that are difficult to confuse with other conditions.
Treatment
In the initial stages of development, some medications are used to help improve the functioning of the heart. In later stages and with the progression of the disease, treatment is carried out surgically: dissection of the fused valve leaflets or replacement with an artificial valve.
Prevention
The cause of mitral stenosis in almost half of the cases is rheumatic fever (the old name is rheumatism). You can get it if you do not properly treat a common sore throat (although not all people who have had a sore throat get rheumatism!), caused by streptococcus - it also causes rheumatic damage to the heart valves. The defect can be prevented by proper treatment of sore throat under the supervision of a physician, with the use of antibiotics and subsequent control ECG registrations.
3. Symptoms and diseases
The main symptoms of disturbances in the valve system include:
- insufficient, labored breathing that does not correspond to physical activity or body position (for example, lying down);
- dizziness, weakness, fatigue, lightheadedness, fainting with minor exertion;
- painful or other discomfort in the chest, synchronous with the processes of inhalation and exhalation;
- swelling in the lower legs and/or abdomen; Subjectively, this may be felt as flatulence (accumulated intestinal gases) or belching.
Valve defects, i.e. their incorrect structure or functioning may be congenital
, and
acquired
(for example, due to infections, unhealthy habits, etc.).
The most common ones are:
- stenosis – narrowing of the lumen;
- regurgitation - incomplete closure with reverse blood flow;
- prolapse (usually of the mitral valve) - sagging of the valve leaflets into the atrium.
About our clinic Chistye Prudy metro station Medintercom page!
1.How does the heart work?
If we consider the body as a complex dynamic biosystem, then the heart
is a muscle pump that ensures constant blood flow through the vessels and, accordingly, nutrition, oxygenation (oxygen saturation), cleansing of all organs and tissues. Contracting rhythmically, automatically and non-stop, the heart muscle performs a tremendous job, pumping about 10 thousand liters of blood per day.
It is well known that the heart, like a pump, consists of several chambers and valves
, ensuring blood circulation in the desired direction and hermetically blocking reverse flow. Heart valves open and close up to 100 thousand times a day. The characteristic sound of a heartbeat is formed by the harmonious and clear (normally) work of the two upper, leaflet valves (tricuspid, i.e. tricuspid, and bicuspid, or mitral) and two lower, “semilunar” (aortic and pulmonary, i.e. pulmonary ). Unfortunately, the heart and its constituent elements, like any other organ in the human body, are not immune from congenital malformations, diseases, or wear and tear.
A must read! Help with treatment and hospitalization!
2.Danger of valve pathology
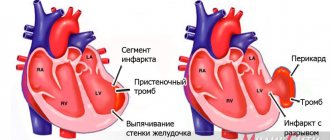
Any pathology in the mechanics of one or more heart valves inevitably affects the functioning of the myocardium as a whole, and therefore the entire life support system - no matter how stable it may be. The most common negative effect in this sense is that the heart muscle, automatically compensating for blood deficiency and working with constant overload, gradually hypertrophies
– increases in volume, stretches.
As a result, the so-called heart failure to varying (sometimes life-threatening) degrees. Arrhythmia, a tendency to thrombus formation due to blood stagnation, erosion,
etc.
may occur shortness of breath
, i.e. feeling of lack of air. Actually, this is a deficiency of oxygen in the blood, which is not oxygenated or purified properly.
Visit our Cardiology page
4.Diagnosis and treatment of the disease
Diagnosis
is established by a cardiologist based on complaints, anamnesis, results of auscultation, percussion and additional studies (ECG, ultrasound, etc.).
Treatment
can range from recommendations to follow certain rules and restrictions in daily life - and these recommendations should be taken seriously - to surgery. Over the past decades, cardiac surgery has accumulated a rich arsenal of methods for effective correction, implantation, and surgical reconstruction, which makes it possible to successfully cope with many serious and dangerous problems in the functioning of the heart muscle and its valves.