People in various situations sometimes feel chest pain that subsides over time. If this recurs regularly, you need to visit a therapist so that he can find out the cause and prescribe the correct treatment. Chest pain can have different etiologies, and without the help of a doctor it is impossible to determine whether the heart is stabbing or another organ is hurting.
Character of chest pain
The nature of chest pain differs into several types:
- pressing;
- piercing;
- aching.
The pain may be localized to a specific area or may be felt throughout the entire chest and radiate to the shoulder or arm. Aching, pressing or stabbing pain in the heart area occurs under various circumstances - when changing posture, during inhalation, with increased stress, or even at rest. In terms of duration, it can be short-term or long-term.
Symptoms
The pathology has quite varied symptoms, which largely depend on the type of damage, causes, concomitant diseases and duration of the disease. The main symptoms include:
- bad breath, burning, heartburn, cough, shortness of breath, difficulty breathing;
- sharp pain (most often behind the sternum);
- low pressure;
- decreased appetite, weakened immune system, gastrointestinal problems;
- pale skin color, blue mucous membranes, etc.
The first and most obvious symptom is problems with swallowing.
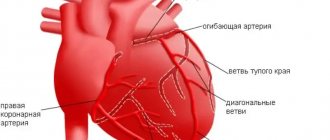
Pain due to heart disease
There are a number of heart diseases that are symptomatic of chest pain.
Compressive pain occurs as a result of manifestations of ischemic diseases. With angina pectoris, an attack of pain can last up to 20 minutes. If after this the pain does not subside, then it is probably not just angina, but a myocardial infarction. During a heart attack, pain radiates to the arm, jaw, shoulder or shoulder blade.
Aching and stabbing pain in the heart area is caused by heart diseases such as myocardial dystrophy, cardiomyopathy, pericarditis, myocarditis, and cardiosclerosis.
conclusions
Do not neglect the importance of the symptom when your heart hurts after eating. This can be a signal of serious illness or interfere with normal life activities. If discomfort occurs in the chest while eating, consult a doctor who will prescribe the necessary examinations and offer the correct solution to the problem with the help of medication or surgical treatment. Diet and psychotherapy have a significant effect. If you are worried about tachycardia after eating, we recommend that you read our expert’s article on this topic.
Chest pain due to gastrointestinal and respiratory diseases
When an esophageal ulcer worsens, severe pain occurs in the chest, as a result of which in some cases the person may lose consciousness. The pain occurs when eating, and is similar in nature to the symptoms of angina pectoris; it seems as if the heart is stabbing. The same pain occurs with cancerous tumors, Mallory-Weiss syndrome (rupture of the esophagus) and also as a result of chemical burns of the esophagus.
Lung diseases, such as pneumonia, bronchitis, pleurisy, tuberculosis and silicosis, are manifested by aching pain and heaviness in the chest. Symptoms that differ from heart disease are cough, which may include shortness of breath and respiratory failure. As a result of shortness of breath, many people experience heart palpitations.
Lapina T.L. Esophageal pain // Medical Bulletin. – 2006. – No. 32 (375). - October 11. - With. 16.
Esophageal pain
T.L.
Lapina A detailed and complete description of such an important symptom as pain allows the doctor to “find” the correct diagnosis, assess the stage of the disease and possible complications.
Pain in diseases of the esophagus
is often very “eloquent”, clearly indicating the nosological form, but there are also frequent situations when chest pain requires a broad differential diagnosis, and it is not easy to identify its connection with esophageal pathology.
T.L. Lapina, associate professor of the course “Functional diagnostics and pharmacotherapy in gastroenterology” at the Department of Family Medicine of the MMA named after. THEM. Sechenov
It is necessary to determine whether the pain is caused by swallowing or not. Pain when swallowing
is called
odynophagy
.
If there is no connection between pain and swallowing, it is called spontaneous. As a feature of odynophagia, its possible combination with dysphagia should be noted. Dysphagia
, which is defined as difficulty, obstruction or discomfort during swallowing (that is, when food passes through the oral cavity, pharynx and esophagus) when pathological changes in the esophagus become more severe, can indeed develop into odynophagia or become an additional symptom when painful swallowing occurs.
Odynophagia
, unlike spontaneous pain, as a rule, very clearly indicates that
the pain belongs to the esophagus
. Diseases of the esophagus with odynophagia are often accompanied by destructive changes in the mucous membrane: chemical burn of the esophagus, infectious esophagitis (especially viral - herpetic, cytomegalovirus, but also bacterial and fungal), drug esophagitis, erosive and erosive-ulcerative esophagitis with gastroesophageal reflux disease, esophageal tumors. The severity of odynophagia can vary, be minor and occur only when swallowing solid food or hot drinks, or it can accompany every meal and be extremely painful. Odynophagia can make the patient refuse to eat. We observed a young woman who came to the clinic with complaints of intense pain behind the sternum when passing solid and liquid food (the most severe pain was localized in the middle third of the sternum); a feeling of difficulty in passing food in the middle third of the sternum and constant pain along the esophagus, especially in the middle third of the sternum, which was so pronounced that in order to alleviate it, the patient took a forced position (lying on her stomach or tilting her body forward in a vertical position) . Thus, in one case there was a combination of odynophagia, dysphagia and esophageal pain; not related to swallowing. The complaints were due to a large ulcer localized on the posterior wall in the middle third of the esophagus, the formation of which was caused by taking a nutritional supplement. If the pain is not caused by swallowing (or is not associated with other typical esophageal symptoms, such as heartburn), then it can be difficult to determine its cause, since pain localized to the chest is very common. Even in the most general terms, it is necessary to differentiate a number of possible sources/causes of pain (see table).
Table. Causes of chest pain
Cardiac
| Non-cardiac | |
| - ischemic - non-ischemic |
|
Determine the true cause of chest pain
It's not always easy.
Thus, according to SR Achem (2005), in the USA in the late 80s. last century, when conducting coronary angiography, up to 30% of those examined did not have damage to the coronary arteries of the heart: with a general count throughout the country, up to 300 thousand cases of non-cardiac pain in the chest could be detected annually. When analyzing domestic data from coronary angiography of 425 patients, changes in the coronary vessels were not detected in 9.4% of cases, and the diagnosis of gastroesophageal reflux disease was established in 6.4%. The following should be listed as causes of esophageal pain: acid-peptic factor during reflux; smooth muscle spasm; stretching of the esophagus; damage to the sensory nerve endings of the esophagus during tumor growth. Accordingly, gastroesophageal reflux disease is most often accompanied by esophageal pain. It is recognized that in 50% of patients with noncardiac chest pain, the cause of pain is precisely gastroesophageal reflux. More rare causes of pain are diseases caused by movement disorders (esophagospasm, achalasia cardia) and tumors. With esophagospasm, the pain is intense, localized in the sternum or high in the epigastric region, radiating along the front surface of the chest up to the neck, into the lower jaw, shoulders, occurring either spontaneously or when swallowing food or saliva, or during neuropsychic stress. With achalasia cardia, the pain is localized at the level of the lower third of the sternum and usually occurs after eating due to overstretching of the esophagus with stagnant contents. With gastroesophageal reflux disease, pain is also localized behind the sternum, can be pressing, burning, radiates to the back, often occurs in the supine position and after eating, decreases or disappears after taking antacid or antisecretory drugs. To establish the esophageal cause of chest pain, it is necessary to carefully question the patient. The combination of pain with other esophageal symptoms (heartburn, dysphagia) significantly helps in the interpretation of the pain syndrome. With a typical clinical picture of gastroesophageal reflux disease, proton pump inhibitors can be immediately prescribed, treatment of which is likely to lead to the disappearance of pain. In the absence of a clue in the form of typical esophageal symptoms, a detailed instrumental examination may be required. An X-ray examination of the chest (to exclude lung diseases) and an ultrasound examination of the abdominal organs (to exclude pancreatobiliary pathology) are advisable. X-ray examination of the esophagus and stomach will make it possible to establish a diagnosis of esophagospasm, achalasia cardia, tumor, but for most cases of reflux disease it will be uninformative. The importance of endoscopy also cannot be overestimated, since pain can be a manifestation of non-erosive (endoscopically negative) reflux disease. 24-hour pH monitoring
has been repeatedly studied as a method for objectively identifying the cause of non-cardiac chest pain.
Its diagnostic value is debated. About 40% of patients with noncardiac pain demonstrate pathological acid reflux, a positive symptom index. However, recorded acid reflux may in some cases not indicate the presence of reflux disease, including as a cause of non-cardiac pain. Esophageal manometry
, unfortunately, cannot be considered as an optimal diagnostic test. According to WG Paterson (1998), pathological manometry data are found in 60% of patients with non-cardiac chest pain, but the identified changes are insignificant, atypical (that is, not characteristic of esophagospasm), regarded as nonspecific motor disorders and are unlikely to have significant clinical significance . In addition, episodes of non-cardiac pain may be irregular, which also makes their diagnosis difficult. Carrying out manometry with provocative tests (acid perfusion, betanicol stimulation or balloon distension of the esophagus) in most cases allows to initiate pain syndrome and increases the accuracy of diagnosis, however, it becomes difficult and uncomfortable for the patient. It becomes obvious that a simple and informative test with a proton pump inhibitor (for example, omeprazole) serves as a very attractive diagnostic method for gastroesophageal reflux disease with extraesophageal manifestation - non-cardiac chest pain. If after a trial course of a proton pump inhibitor the pain goes away, then it was caused by reflux. Thus, F. Cremonini et al. (2005), in a meta-analysis of studies undertaken to compare the proton pump inhibitor test with endoscopy and pH monitoring, found that the sensitivity of the test was 80% and the specificity 74% for diagnosing this condition. The same authors conducted a meta-analysis of eight randomized controlled trials to evaluate the effectiveness of a proton pump inhibitor treatment for noncardiac chest pain compared with placebo. The risk of continued episodes of non-cardiac chest pain after treatment with a proton pump inhibitor was 0.54 (95% CI (confidence intervals) 0.41-0.71), NNT (number needed to treat) - 3 (95% CI 2-4 ). It was concluded that proton pump inhibitors may be used to treat non-cardiac chest pain. A recent review of the literature on this topic (JR Malagelada, 2004) recommends the possibility of prescribing a proton pump blocker for non-coronary chest pain at a standard dose for a short course of treatment, for example one week, which may be sufficient to relieve pain. Other drug approaches to the treatment of esophageal pain include nitrates and calcium channel blockers (for hypermotor dyskinesias of the esophagus), as well as antidepressants.
Chest pain due to sprains, intercostal neuralgia and injuries
With intercostal neuralgia, which manifests itself as a result of muscle spasm, the nerve roots are compressed, and a sharp pain occurs in the chest, radiating to the back.
Chest pain can also be caused by damage to the pectoral or back muscles - sprains, tumors (rhabdomyoma), inflammation (myositis).
Pain from bruises, fractures or cracked ribs can also be mistaken for heart pain. However, by the location of the source of pain, it can be determined that it is not the heart that is hurting.
If you have chest pain or heart pain, contact our clinic. Experienced doctors will make the correct diagnosis and prescribe a course of treatment.
Esophageal injuries
If a patient comes to the doctor asking why there is pain in the middle of the chest when swallowing, then the doctor must determine the cause. This is often associated with trauma to the esophagus, which may be:
- received due to various types of damage: gunshots, stab wounds, incised wounds, etc.;
- associated with internal pathological processes: neoplasms, narrowing, expansion in different areas (neck, thoracic region, etc.);
- associated with various pathologies of body systems, for example, damage to large vessels;
- received due to damage during surgical treatment, for example, during intubation, neck injuries, etc.
The type and duration of treatment depends on the type of injury and the severity of the damage.
Diagnostics
The doctor will determine which examinations will be needed during the initial consultation. To do this you need to see a therapist
who will give recommendations and directions, or you can immediately go to
a gastroenterologist
who will prescribe an endoscopy of the stomach and esophagus.
X-rays (with and without contrast agent), ultrasound
of certain internal organs, checking the functioning of the cardiovascular system and additional studies and tests (for each specific case) may also be prescribed.