Why is it necessary to do a lipid profile?
The content of the article
A lipidogram allows you to assess the risk of developing plasma atherosclerosis even with normal levels of total cholesterol.
A lipidogram or lipid profile includes the study of the following indicators:
- triglycerides;
- total cholesterol;
- low density lipoproteins - LDL;
- high density lipoproteins - HDL.
Their values provide information about the state of lipid metabolism and metabolic disorders and, therefore, about the risk of developing atherosclerosis and cardiovascular complications, such as:
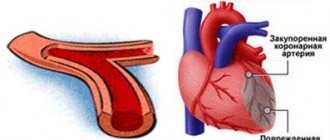
- Coronary artery stenosis and myocardial infarction;
- Stroke.
Factors in the development of atherosclerosis:
- elevated lipid levels - triglycerides, total cholesterol and LDL fraction;
- lower HDL cholesterol levels;
- hypertension;
- smoking;
- diabetes;
- increased levels of fibrinogen, homocysteine;
- obesity;
- poor diet rich in saturated fats;
- low physical activity;
- old age.
Why is cholesterol needed?
Cholesterol is necessary for our body for the functioning of organs and systems. It is part of cell membranes, ensures their strength, participates in the synthesis of sex hormones (androgens and estrogens), as well as those hormones produced by the adrenal glands (cortisol) and in the ovaries (estradiol). Cholesterol plays an important role in the metabolism of fat-soluble vitamins (A, D, E and K). Approximately three-quarters of cholesterol is synthesized in the body and only a quarter comes from food.
Lipoproteins, which are divided into:
- Very low-density lipoproteins (VLDL), which are produced in the liver, contain lipids (triglycerides and cholesterol). They are transported through the blood to the tissues;
- low-density lipoproteins (LDL) are formed from VLDL due to the release of triglycerides from them, contain mainly cholesterol, which is delivered from the liver to the body tissues;
- High-density lipoproteins (HDL) transport unused cholesterol from tissues to the liver, where it is synthesized into bile acids.
Andrey Pristrom: “Lipid metabolism disorders occur due to a breakdown in the mechanism for regulating cholesterol levels. What does it mean? When cholesterol rises, mechanisms must be activated that reduce its formation, and vice versa. There are many reasons that can lead to such an “imbalance.” It’s almost impossible to say unequivocally what exactly triggered the failure.”
What is checked during the analysis?
The package includes measurements of the level of indicators such as:
- Total cholesterol
– determines cholesterol levels. Its measurement is used as a screening test for dyslipidemia, a disorder of lipid metabolism, and as an indicator for assessing the effect of antiepileptic treatment. - Triglycerides
– determines the level of simple fats, the main energy reserve in adipose tissue - LDL cholesterol
is low-density lipoprotein or “bad” cholesterol. LDL is an indicator for assessing cardiovascular risk. Atherosclerosis and coronary heart disease are more common in patients with elevated LDL levels. - HDL cholesterol
is high-density lipoprotein or “good” cholesterol. High levels of HDL reduce the risk of developing atherosclerosis and coronary heart disease.
Blood test for cholesterol - lipid profile
- Triglycerides (TG)
- Total cholesterol (CHOL).
- Cholesterol-HDL (HDL)
- LDL cholesterol (LDL)
- VLDL cholesterol (VLDL)
- Atherogenicity index (coefficient)
In order to determine the risk of developing vascular atherosclerosis, it is enough to take a total cholesterol test. If the indicator is normal, there is no need to worry. True, if nothing bothers you, and you have a good heredity behind you for cardiovascular diseases. If not, or the indicator is elevated, it is important to take a full lipid profile and find out the “balance of power” between different fractions of cholesterol. And consult a specialist in a timely manner.
Triglycerides (TG). Normal – 0.41−1.8 mmol/l
Triglycerides are the main store of fats in our body; they are formed in the liver. In most cases, elevated levels of triglycerides (the so-called blood chylosis) are a consequence of poor nutrition with excess fatty foods and carbohydrates, so the test should be taken no earlier than 9 hours after the last meal. The cause of the increase may be primary (hereditary) hyperlipidemia , and, much more often, secondary hyperlipidemia, including poor nutrition, obesity, impaired glucose tolerance and diabetes mellitus, hypothyroidism, gout, liver, pancreas and kidney diseases. Also, the cause of the increase may be stress, alcohol abuse, and taking certain medications (beta blockers, corticosteroids, diuretics and some others). A decrease in values is recorded with malnutrition, hyperthyroidism, malabsorption, and long-term intake of vitamin C.
Total cholesterol (CHOL). Normal – 3.2−5.6 mmol/l
The most important lipid, which is a structural component of all cell membranes, a precursor of sex hormones, corticosteroids, bile acids and vitamin D. Up to 80% of cholesterol is synthesized in the liver, the rest enters our body with food. The cholesterol content in the blood largely depends on age, so for an infant the upper limit of normal is 5.25 mmol/l , and for a man over 70 – 6.86 mmol/l . Cholesterol is carried by couriers called lipoproteins, of which there are three main types - high density, low density and very low density. An increase in total cholesterol, as well as triglycerides, occurs with primary and secondary hyperlipidemia.
Despite the fact that screening studies have adopted average limits for total cholesterol (5.6 mmol/l) and its components, doctors currently use tables of norms in accordance with gender and age. Therefore, if the indicators deviate, consult a doctor to decipher the analysis.
Cholesterol-HDL (HDL). Normal – not less than 0.9 mmol/l
This cholesterol fraction is involved in the transport of cholesterol from peripheral tissues to the liver. This means that they take cholesterol from the surface of blood vessels, including the legs, heart, and brain, and carry it to the liver. This means that HDL plays an important anti-atherogenic role, preventing the formation of cholesterol plaques and the development of atherosclerosis. And if the level of total cholesterol is increased due to HDL cholesterol, this is considered a good prognostic factor, and cholesterol should not be reduced. At the same time, a decrease in the level of “good” cholesterol below 0.90 mmol/L for men and 1.15 mmol/L for women is considered a risk factor for atherosclerosis.
LDL cholesterol (LDL). Normal – 1.71−3.5 mmol/l
Low-density lipoproteins are the main carrier of cholesterol in our body. It is he who carries the fat synthesized in the liver to organs and tissues. It is believed that the level of LDL cholesterol has a much greater influence on the development of atherosclerosis than the level of total cholesterol. That is why it came to be called “bad” cholesterol. In conditions where the vascular wall is compromised by risk factors (nicotine, high concentrations of glucose, homocysteine, increased blood pressure), LDL cholesterol is deposited in it, forming an atherosclerotic plaque. For people with risk factors for atherosclerosis (age over 45 years for men and 55 years for women, cases of early death from cardiovascular diseases among relatives, smoking, diabetes mellitus, hypertension, obesity), the LDL cholesterol level should not exceed 3.37 mmol/l , values from 3.37 to 4.12 mmol/l are regarded as a medium risk factor for the development of atherosclerosis, and above 4.14 mmol/l - as high.
VLDL cholesterol (VLDL). Normal – 0.26−1.04 mmol/l
These lipoproteins are synthesized in the liver and small intestine and serve as precursors of LDL, that is, they are also carriers of “bad” cholesterol.
Atherogenicity index (coefficient)
This is an indicator that can be calculated based on the lipid profile results.
2.0 to 2.5 units is considered normal The maximum normal values are 3.2 for women and 3.5 for men. Everything above indicates a significant risk of developing atherosclerosis and requires measures to reduce it, which can be either non-medicinal (changing diet, losing weight, quitting smoking, combating physical inactivity, taking various dietary supplements) or medicinal (taking medications from various groups, mainly statins). If necessary, the doctor will individually select a drug for you
Who should have a lipid profile?
Lipid profile testing is recommended for patients with problems such as:
- high cholesterol/lipid metabolism disorders;
- if a family member is diagnosed with a lipid metabolism disorder;
- suspicion of hereditary hypercholesterolemia;
- family history of myocardial infarction, especially at a young age;
- overweight and obesity;
- smoking.
In addition, a lipid profile study is useful for:
- monitoring lipid-lowering therapy;
- monitoring the condition of patients who have suffered myocardial infarction and ischemic stroke.
Diagnostics (lipid profile)
The main method for diagnosing lipid metabolism disorders is the determination of 4 main indicators of lipid metabolism in venous blood (total cholesterol, low and high density lipoproteins, triglycerides), which is called a lipid profile. To make a diagnosis, such an analysis is performed at least twice, one to several weeks apart. Blood is taken on an empty stomach, and it is recommended to avoid a heavy dinner the night before.
If a person is healthy and does not have cardiovascular diseases, diabetes mellitus or serious kidney disorders, the main indicator is total cholesterol. The norm is less than 5 mmol/l.
In the presence of pathologies of the heart and blood vessels, as well as a high risk of their development (determined by the cardiovascular risk scale - SCORE), another control criterion is used: low-density lipoprotein cholesterol.
The target depends directly on the level of risk:
- for low-risk patients – less than 3 mmol/l;
- for patients with moderate risk – less than 2.6 mmol/l;
- for high-risk patients – less than 1.8 mmol/l;
- for patients with a very high risk level - less than 1.4 mmol/l.
The risk of developing cardiovascular accidents is considered high with a score of 5 or more on the SCORE scale.
Elevated levels of LDL cholesterol can cause lipid deposits in the walls of blood vessels, usually in the arteries. It is LDL cholesterol that leads to the appearance of atherosclerotic plaques, which narrow the lumen of blood vessels or completely clog them, thereby blocking the flow of blood.
Andrey Pristrom: “In people with a severe lipid profile disorder, it is also recommended to perform an ultrasound of the brachiocephalic arteries in order to identify atherosclerotic plaques. Atherosclerosis, which develops against the background of lipid metabolism disorders, is a systemic process. If there are changes in the brachiocephalic arteries, then they will be in other vessels.”
The consequences of atherosclerosis are very severe. This is the development of myocardial infarction, stroke, chronic coronary heart disease, occlusion of peripheral arteries, which can lead to amputation of the lower extremities.
Hereditary hypercholesterolemia can be suspected by a blood test: the level of low-density lipoprotein cholesterol will be above 5 mmol/l. In addition, in such people, yellow formations (xanthomas) and white cloudy stripes on the cornea can be seen on the eyelids. Another sign of a hereditary form of lipid metabolism disorders is the appearance of growths on the extensor tendons of the fingers and in the area of the Achilles tendon. In such cases, genetic testing is recommended to confirm or refute hereditary hypercholesterolemia.
The frequency of studies depends on the presence of a risk of cardiovascular accidents. If the risk is low, a blood lipid profile should be performed approximately once every five years; if the risk is high, once a year. However, after 40 years, it is advisable to do a blood test for cholesterol levels annually.
Normal lipid profile or control values
In a healthy person, the following values should be maintained:
| total cholesterol | less than 190 mg/dl |
| LDL fraction | <115 mg/dL – for low to moderate cardiovascular risk |
| <100 mg/dL – for high cardiovascular risk | |
| <70 mg/dL – for very high cardiovascular risk | |
| HDL for men | more than 40 mg/dl |
| HDL for women | more than 45 mg/dl |
| triglycerides | less than 150 mg/dl |
Lipid profile results
Total cholesterol is increased when:
- various forms of hypercholesterolemia;
- violation of the outflow of bile due to obstruction of the biliary tract, cholestasis; pancreatic diseases;
- hypothyroidism;
- diabetes;
- alcoholism;
- type of diet high in fat.
A decrease in total cholesterol is observed with:
- alipoproteinemia;
- fatty diarrhea with malabsorption syndromes - impaired absorption of essential nutrients;
- myeloproliferative diseases - uncontrolled growth of blood cells;
- hyperfunction of the thyroid gland.
An increase in triglyceride levels is observed with:
- hereditary and acquired dyslipidemias;
- metabolic diseases - diabetes, gout;
- overweight and obesity;
- liver diseases and alcoholism;
- kidney diseases;
- hypothyroidism of the thyroid gland.
A decrease in triglyceride levels occurs when:
- hyperthyroidism;
- abetalipoproteinemia – a disease that prevents the normal absorption of fats and fat-soluble vitamins from food;
- malnutrition;
- malabsorption - insufficient absorption of nutrients in the digestive tract.
LDL cholesterol increases when;
- hypercholesterolemia;
- hyperlipoproteinemia;
- a diet high in saturated fat;
- hypothyroidism;
- diabetes;
- chronic renal failure;
- anorexia;
- porphyria – a hereditary disorder of pigment metabolism with an increased content of porphyrins in the blood and tissues and their increased excretion in urine and feces.
A decrease in LDL cholesterol occurs when:
- hypo- or abetalipoproteinemia;
- overactive thyroid gland;
- chronic anemia;
- severe damage to the liver and biliary system.
HDL cholesterol levels should be maintained within normal limits as it is a factor that reduces the risk of cardiovascular disease. This is achieved through proper nutrition, moderate alcohol consumption, regular exercise and a healthy lifestyle.
A decrease in HDL cholesterol occurs with obesity, elevated triglyceride levels, and taking certain medications - androgens, diuretics, beta-blockers and others.
How to prepare for the test?
Blood test material should be taken on an empty stomach, that is, with an 8-12 hour break from the last meal. The recommendation applies to all studies because changes caused by food intake are difficult to predict and the values obtained are interpreted in comparison with reference values established under standard conditions.
The day before the blood test, you should avoid heavy and fatty foods and alcohol consumption.
On the day of the test
Immediately before taking a blood test, you are allowed to drink a small amount of water.
It is recommended to collect blood in the morning from 7:00 to 10:00. If blood is collected at other times of the day, this should be taken into account when interpreting the test results.
Immediately before collection, a 15-minute rest is advisable.