Hypotensive effect - what is it? This question is asked by women and men who are faced with the problem of high blood pressure or hypertension for the first time and who have no idea what the hypotensive effect of the drugs prescribed to them by their attending physician means. An antihypertensive effect is a decrease in blood pressure under the influence of a particular drug.
Experienced professional therapists of the highest category at the Yusupov Hospital Therapy Clinic, who are proficient in advanced treatment and diagnostic methods, will provide qualified assistance to patients with arterial hypertension and select an effective treatment regimen that eliminates the development of negative consequences.
Hypotensive syndrome
Hypotensive syndrome is a whole complex of symptoms that reflects a persistent decrease in intracranial pressure in women. It occurs only in pregnant women aged 25 to 29 years. This syndrome significantly reduces the quality of life of the expectant mother and requires qualified medical care.
Make an appointment
Causes
The causes of this pathology are the following factors:
- severe dehydration after undergoing drug therapy;
- head injuries;
- leakage of cerebrospinal fluid due to a violation of the integrity of the skull bones or brain tissue;
- a decrease in blood pressure, leading to a decrease in intracranial pressure.
Every pregnant woman should be doubly attentive to her health, since she is also responsible for the life of the child. Any changes in health should be a reason to consult a doctor. Doctors at the Yusupov Hospital are ready to answer all their patients’ questions at any time, either in person or by phone.
Symptoms of hypotensive syndrome in pregnant women are:
- severe constricting sudden headaches;
- increased headaches when raising the head or in a sitting position;
- reduction in the intensity of headaches when lowering the head;
- prostration;
- feeling drowsy;
- irritability;
- attacks of nausea and vomiting.
Of course, many of the above symptoms occur in pregnant women and are a consequence of changes in the functioning of all organs and systems during the period of bearing a baby. They may have nothing to do with hypotensive syndrome.
But in any case, if the expectant mother’s health worsens, she must inform the doctor about it. Caution and attentiveness to your health will help you avoid the development of complications, identify hypotensive syndrome and undergo an effective course of therapy.
Diagnostics
If symptoms of the disease appear during pregnancy, it is necessary to undergo examinations by a gynecologist, neurologist and neurosurgeon. Doctors conduct examinations, analyze all the patient’s complaints and make a preliminary diagnosis. To confirm or refute it, the pregnant woman is prescribed a number of diagnostic measures, namely:
- general and biochemical blood test;
- general urine analysis;
- X-ray of the skull;
- spinal tap;
- MRI of the brain.
At the Yusupov Hospital, all diagnostic procedures are carried out using modern medical equipment, which allows you to obtain accurate data and promptly begin treatment.
Antihypertensive therapy for diabetes mellitus
Diabetes mellitus is a chronic disease, the development of which is associated with an absolute or relative deficiency of the hormone insulin. Lack of insulin or lack of sensitivity to it leads to an increase in blood glucose levels. This condition has a negative impact on all systems and organs of the human body, including the cardiovascular system.
Almost all patients suffering from diabetes complain of high blood pressure, which can be reduced with great difficulty without the help of a doctor.
Hypertension and diabetes mellitus
Hypertension in patients with diabetes is an integral and very dangerous component, which can several times increase the risk of developing the following diseases:
- 3-5 times - heart attack;
- 3-4 times - stroke:
- 10-20 times - blindness;
- 20-25 times – renal failure;
- 20 times - gangrene, requiring limb amputation.
If blood pressure readings exceed 140/90, there is no need to hesitate to contact a specialist, since hypertension that occurs against the background of diabetes mellitus can lead to the development of irreversible consequences, often incompatible with life.
Hypertension in type 1 diabetes mellitus
The main and most dangerous cause of arterial hypertension in type 1 diabetes mellitus is the presence of diabetic nephropathy in patients with this disease. The development of this complication is observed in almost 40% of people suffering from type 1 diabetes. Increased blood pressure is directly related to the amount of protein excreted in the urine.
Hypertension due to renal failure also develops due to poor excretion of sodium in the urine. As sodium increases in the blood, fluid accumulates to dilute it. Due to the increase in circulating blood volume, blood pressure increases. This process may also be associated with an increase in glucose concentration, which occurs in diabetes mellitus. As a result, to reduce blood density, the body produces even more fluid and the volume of circulating blood further increases for this reason.
Hypertension in type 2 diabetes mellitus
One of the factors that provokes the development of type 2 diabetes mellitus is insulin resistance, i.e. decreased sensitivity of tissues to the action of insulin.
To compensate for insulin resistance, excessive amounts of insulin circulate in the blood, which itself causes an increase in blood pressure. Over time, a narrowing of the lumen of blood vessels occurs, caused by atherosclerosis, which also contributes to the occurrence of hypertension. In parallel, patients experience the development of abdominal obesity, and, as is known, it is from adipose tissue that substances that increase blood pressure are released into the blood.
Hypertension in diabetes: features
In patients with diabetes mellitus, there is a disturbance in the natural daily rhythm of blood pressure fluctuations. In a healthy person, blood pressure levels in the morning and at night are usually 10-20% lower than in the daytime. In patients with diabetes, there is no decrease in blood pressure at night. Moreover, their nighttime pressure readings may be even higher than their daytime ones. According to experts, this phenomenon is caused by diabetic neuropathy. An increased concentration of sugar in the blood leads to damage to the autonomic nervous system, which is responsible for regulating the body's vital functions. There is a deterioration in the ability of blood vessels to regulate their tone - narrowing and relaxing depending on the load.
Antihypertensive drugs for diabetes mellitus
To date, eight groups of antihypertensive drugs are known, of which five are considered primary, and three are considered additional. Antihypertensive therapy for diabetes mellitus involves taking the following medications:
- diuretics;
- calcium channel blockers;
- beta blockers;
- centrally acting drugs;
- ACE inhibitors;
- angiotensin II receptor blockers;
- alpha-blockers;
- renin inhibitor (racillosis).
Medicines that make up additional groups are prescribed, most often, as components of combination treatment.
Safe antihypertensive therapy: blood pressure lowering or control?
Russian guidelines for the diagnosis and treatment of hypertension recommend 5 main classes of antihypertensive drugs: angiotensin-converting enzyme inhibitors (ACEIs), angiotensin I receptor blockers (ARBs), calcium antagonists, β-blockers, diuretics. There is no convincing evidence yet that one class of antihypertensive drugs is superior to others [4]. α-blockers, imidazoline receptor agonists, and direct renin inhibitors may also be used as additional classes. When choosing antihypertensive therapy (AHT), it is necessary first to evaluate the effectiveness, the likelihood of side effects and the benefits of the drug in a specific clinical situation.
A meta-analysis, which included 7 randomized studies (including 4 large clinical studies: Dutch TIA trial; PATS; HOPE; PROGRESS) and a total of 15,527 patients, showed that ADT can reduce the risk of recurrent stroke by 24%, MI - by 21% and cardiovascular events – by 21% [5].
In the 2013 European Society of Hypertension (ESH) and European Society of Cardiology (ESC) hypertension treatment working group recommendations for the treatment of hypertension, in the seventh report of the US Joint National Commission on the Prevention, Detection, Evaluation and Treatment of High Blood Pressure (JNC VII) with targeted blood pressure values are defined as a decrease in SBP and DBP less than 140/90 mm Hg. Art. in all patients with hypertension, in patients with diabetes mellitus – DBP <85 mm Hg. Art. In people over 80 years of age, it is recommended to reduce SBP to
140–150 mm Hg. Art. and even to values <140/90 mm Hg. Art. with good tolerance [6, 7].
The fourth revision of Russian recommendations indicates similar target blood pressure values: “Prevention, diagnosis and treatment of arterial hypertension” (RKO/VNOK, 2010): “When treating patients with hypertension, the blood pressure value should be less than 140/90 mm Hg. Art., which is its target level. If the prescribed therapy is well tolerated, it is advisable to reduce blood pressure to lower values. In patients with a high and very high risk of cardiovascular disease, it is necessary to reduce blood pressure to <140/90 mmHg. Art. within 4 weeks. In the future, subject to good tolerance, it is recommended to reduce blood pressure to 130–139/80–89 mmHg. Art. If lowering blood pressure is poorly tolerated, it is recommended to lower it in several stages. At each stage, blood pressure decreases by 10–15% from the initial level in 2–4 weeks. followed by a period for the patient’s adaptation to lower blood pressure values. When achieving target blood pressure levels, it is necessary to take into account the lower limit of reducing SBP to 110–115 mm Hg. Art. and DBP up to 70–75 mm Hg. Art., and also ensure that during treatment the pulse blood pressure does not increase in elderly patients, which occurs mainly due to a decrease in DBP” [4].
The development of drug-induced hypotension, which increases the risk of renal, myocardial and cerebral hypoperfusion, is one of the most serious problems of AHT [8, 9]. The problem most often discussed in the literature is hypotension of the first dose when prescribing ACE inhibitors. However, the incidence of drug-induced hypotension during treatment with antihypertensive drugs reaches 10% [10].
In hypertensive patients, hypotension is a common condition that has received insufficient attention in studies of antihypertensive regimens [11]. The most common causes of hypotensive conditions in patients with hypertension are the use of drugs with a pronounced vasodilation effect or causing a decrease in circulating blood volume (CBV), as well as spontaneous hypotension, which develops mainly at night and is caused by impaired autoregulation of vascular tone [12]. The occurrence of drug-induced hypotonic reactions is more typical for dosage forms with rapid release of the active ingredient, which have low T/P (Trough/Peak) values [11].
The T/P indicator allows us to judge the duration of action of an antihypertensive drug in relation to the residual (i.e., after taking the last dose) to peak (maximum effect at the time of maximum concentration of the drug in the blood) activity. When using drugs with a low T/P index, high blood pressure variability is observed, due to excessive hypotension at the peak of the drug's action or insufficient antihypertensive effect at the end of the dosage interval [13]. A decrease in the total volume of fluid in the body and, as a consequence, BCC can lead to a higher concentration of hydrophilic drugs (atenolol, lisinopril) in the blood. The elimination of antihypertensive drugs from the body may also be slower due to decreased renal filtration and decreased liver enzyme activity, which can often be observed in elderly patients. In addition, due to a decrease in the volume of blood circulation, the use of diuretics is limited.
A significant decrease in blood pressure can occur with combination therapy, when several drugs are used that initially do not provide a rapid antihypertensive effect, the maximum effect of which is delayed and the hypotensive reaction occurs after several hours. It is known that an increase in blood pressure variability in itself is an unfavorable prognostic factor associated with the risk of developing cardiovascular complications in patients with hypertension [14]. At the same time, in elderly people, even while taking long-acting medications, a decrease in DBP during wakefulness may be noted [11]. Often, an excessive decrease in blood pressure is observed when self-administering antihypertensive drugs without blood pressure control due to a deterioration in well-being, which in patients with hypertension is not always associated with an increase in blood pressure [15, 16].
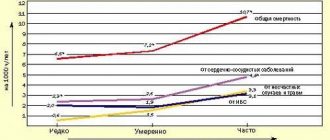
A number of studies in elderly patients or patients with vascular diseases found a paradoxical increase in the incidence of cardiovascular events, most likely due to an excessive decrease in blood pressure [17]. According to the Honolulu Heart Study, orthostatic hypotension in the population over 70 years of age is recorded in 7% of cases, and the mortality rate in this category of patients is 64% higher than in the control group [18].
Neurological complications of antihypertensive therapy, manifested in the form of decreased physical and mental performance, fatigue, tinnitus, dizziness, are observed mainly in elderly patients, especially in the presence of cerebrovascular disease and significant stenoses of the precerebral (carotid and vertebral) and cerebral arteries. In this case, disorders such as sleep disturbances, emotional lability, and depressive states may occur. Sometimes hypoperfusion states can be asymptomatic and can be detected as a decrease in cerebral blood flow based on the results of Doppler ultrasound or magnetic resonance spectroscopy. Apparently, it is hypoperfusion conditions that can be one of the causes of clinically “silent” strokes [19, 20].
Complications of antihypertensive therapy can be caused by a significant decrease in blood pressure as a result of dysfunction of baroreceptors, when its level falls below the lower limit of autoregulation of cerebral circulation, which leads to cerebral hypoperfusion.
In individuals with normal blood pressure, cerebral blood flow is maintained at a constant level (about 50 ml per 100 g of brain matter per minute), the lower limit of autoregulation of cerebral circulation is about 60 mm Hg. Art., and the upper one is about 180 mm Hg. Art., according to average hemodynamic blood pressure. In patients with hypertension, autoregulation of cerebral blood flow adapts to higher blood pressure values, and the higher the usual blood pressure values, the higher the lower limit of autoregulation of cerebral blood flow. In patients with long-term hypertension, the lower limit of autoregulation of cerebral circulation can reach 90–100 mm Hg. Art. Thus, for a patient with hypertension, a decrease in SBP to a level of 120–130 mmHg. Art., especially when trying to quickly “normalize” blood pressure, can be critical and lead to a decrease in perfusion blood pressure and the appearance of symptoms of cerebral ischemia [21].
A study of cerebral blood flow in patients with cerebrovascular pathology shows that cerebral hypoperfusion occurs when blood pressure decreases by an average of 10–20% from normal “working” values [22].
It has been established that repeated cerebrovascular accident depends not only on the nature of the stroke - cerebral infarction or hemorrhage, but also on the level of maintained blood pressure. After hemorrhage, the risk of recurrent cerebral complications was directly proportional to the level of DBP, with the lowest incidence of cerebral damage observed at DBP≤80 mmHg. Art. In patients who suffered an ischemic stroke, the lowest risk of recurrent stroke was found in the DBP range of 80–84 mmHg. Art., and at a lower level, blood pressure increased again. Moreover, after atherothrombotic stroke, the lowest frequency of recurrence of a cerebral event was observed at DBP of 85–89 mm Hg. Art., after lacunar (ischemic cerebral infarction) – 80–84 mm Hg. Art., which was associated with limited possibilities of autoregulation of cerebral blood flow in case of damage to large cerebral arteries [23].
At the same time, in case of intracerebral hemorrhage, it is recommended to reduce blood pressure gradually and only to normal blood pressure levels for the patient, and if they are not known, then SBP to a level of 150–160 mm Hg. Art., and DBP – up to 85–90 mm Hg. Art. [24].
The most important factor that undoubtedly influences the determination of the target blood pressure level is the presence of hemodynamically significant occlusive atherosclerotic lesions of the main arteries. Approximately 20% of patients who have suffered a transient ischemic attack or stroke have severe stenosis or occlusion of at least one carotid artery. Carrying out inadequate AHT in such patients can worsen cerebral perfusion with relatively normal blood pressure values and lead to complications, including the development of ischemic hemodynamic stroke. An analysis of the results of several studies that examined the prognostic value of hypertension and AHT in patients with stenosis or occlusion of the carotid arteries showed the following results.
In patients who have suffered an ischemic stroke or transient ischemic attack and have significant stenosis (narrowing of more than 70% of the lumen) of the internal carotid artery, with an increase in blood pressure, the risk of stroke increases to a lesser extent than in patients without severe atherosclerosis. At the same time, in the UK-TIA study, in patients with clinically symptomatic unilateral occlusive carotid lesions, an increased risk of stroke was found with a decrease in SBP <130 mm Hg. Art. In the presence of bilateral significant stenosis of the carotid arteries, the risk of stroke also increases with a decrease in blood pressure. This is due to a violation of the normal regulation of cerebral blood flow, the value of which is determined by perfusion pressure, which directly depends on systemic blood pressure. In patients in this group who received antihypertensive therapy, the risk of stroke was lowest when SBP values were 150–169 mmHg. Art. and progressively increased multiple times at lower values. Severe bilateral stenosis of the carotid arteries is an indication for surgical treatment, since only after this will patients be able to undergo active antihypertensive therapy and reduce blood pressure to a level safe for the heart, kidneys and other organs [25].
Based on the data presented above, for patients with a history of ischemic cerebral events and suffering from discirculatory encephalopathy, 3 main target levels of SBP are recommended as the most prognostically significant with respect to the risk of recurrent cerebrovascular complications:
• SBP 160–150 mmHg. Art. should be considered minimally acceptable for patients with grade 3 hypertension or bilateral carotid stenosis ≥70%;
• SBP 140–135 mmHg. Art. optimal for patients with stage 2 hypertension and unilateral carotid stenosis ≥70%;
• SBP 120 mm Hg. Art. – the minimum possible for patients with stage 1 hypertension, high normal blood pressure in the absence of severe damage to the main arteries of the head [26].
There is evidence that with a significant decrease in blood pressure, the risk of coronary complications increases [27]. In the INVEST study, which included 22 thousand patients with hypertension and coronary heart disease, DBP was below 90 mm Hg. Art. was associated with an increased risk of MI compared with the group that had the lowest risk of MI at DBP 82.7 mm Hg. Art. [28]. The SHEP study involving 4736 patients with isolated systolic hypertension showed that when DBP decreased below 70 mm Hg. Art. the risk of developing cardiovascular diseases (CVD), including MI, increases, and the risk of CVD increases by 2 times when DBP is less than 55 mm Hg. Art. [29, 30].
Patients with severe (occlusive) coronary artery disease and/or left ventricular hypertrophy have a higher risk of coronary complications with low DBP, although this complication is more typical for patients with stage 1 and 2 hypertension in whom the DBP level has decreased by more than by 25 mm Hg. Art. from the initial value [31, 32].
Another negative aspect of a sharp decrease in blood pressure is a decrease in renal perfusion and, as a result, the development of renal failure. Maintaining optimal blood pressure levels is very important for patients with kidney pathology. For adequate renal perfusion, it is necessary to maintain SBP at a level of 80 to 180 mmHg. Art. When SBP decreases below 80 mm Hg. Art. a decrease in renal perfusion and the development of renal failure are possible [33].
ARBs and ACEIs, by dilating the efferent glomerular arterioles, can cause a decrease in renal perfusion pressure and a decrease in glomerular filtration rate (GFR). The dependence of GFR on the level of angiotensin II becomes especially pronounced with a decrease in blood volume, bilateral renal artery stenosis, and renal artery stenosis of a single kidney [34]. Decreased filtration may result in increased serum creatinine and potassium levels. Hypovolemia and hypotension further exacerbate the decrease in filtration [35].
In recent years, increasing importance has been attached to the indicator of blood pressure variability, since high variability is associated with an increased risk of cardiovascular events [36].
Patients with the greatest BP variability were 6.22 times more likely to develop stroke compared to patients with the least variability [37–39]. It should be noted that in the group of patients with hypertension with increased SBP variability, the incidence of cardiovascular events is 60–70% higher (1372 patients, follow-up time up to 7.5 years) [40]. As a result of a 14-year follow-up of 956 patients, it was revealed that in groups with moderate and high SBP variability, compared with those with low variability, there was an increase in the risk of death by 55 and 49%, respectively [41].
As you know, blood pressure decreases during sleep and rises quickly before waking up. Maximum values are observed after waking up and starting daily activities. The morning rise in blood pressure causes stress on the cardiovascular system, leading to target organ damage and pathological reactions [42].
The magnitude and speed of the morning rise in blood pressure depend on the characteristics of the daily blood pressure profile. Moreover, patients suffering from essential hypertension in the early stages of the disease are characterized by a greater magnitude and speed of the morning rise in blood pressure than in healthy individuals. And in patients with an excessive decrease in blood pressure at night, as well as in patients with an insufficient decrease in blood pressure during night sleep, the morning rise is characterized by a greater magnitude and rate of increase in pressure compared to patients with a normal circadian rhythm [43].
According to a meta-analysis of 4 studies including 3468 patients, high blood pressure variability is an independent predictor of the development of cardiovascular events in patients with hypertension, even without a history of CVD, regardless of age and gender [44].
Based on a clinical and instrumental examination of 65 patients with acute MI, a significant influence of hypertension with increasing variability on the course of the disease and the annual prognosis of patients was proven. The clinical course of the acute period of MI in patients with high blood pressure variability was more severe. In patients with hypertension, a complicated course with the development of acute left ventricular failure was observed 2 times more often (20.8 and 9.8%, respectively), and recurrent infarctions occurred 3 times more often (8.3 and 2.4%, respectively). It was found that during the first year after a heart attack, an increase in blood pressure variability is associated with a 3-fold increase in the risk of death [45]. It has been shown that high blood pressure variability in the acute period of MI correlates with deterioration of left ventricular systolic function [46] and is an unfavorable prognostic criterion for the course of MI [47].
During the morning rise in blood pressure, the maximum number of different cardiovascular events occurs. Thus, it has been shown that most ischemic episodes occur in the morning, which coincides with the frequency of myocardial infarction and sudden death [48]. Most often, MI develops in the first half of the day [49]. In the TIMI II study, the maximum incidence of infarction (34%) was observed between 6:00 and 12:00 hours [50]. The daily rhythm of angina attacks has the same character. The circadian rhythm of variant angina is also characterized by a peak in the morning [51, 52]. It has also been found that there is a relationship between the circadian rhythm and ischemic brain damage: nondippers and overdippers have significantly more “silent” cerebral lesions compared to moderate dippers [53–55]. In a meta-analysis of 31 studies that reported the timing of strokes in 11,816 patients, the odds of having a stroke were 79% higher between 6:00 a.m. and 12:00 p.m. than during other hours. At the same time, in the morning period, the probability of occurrence of all three types of cerebrovascular accident increased (by 55% for ischemic strokes, by 34% for hemorrhagic strokes and by 50% for transient ischemic attack) [56]. It has been shown that the morning rise in blood pressure by 10 mm Hg. Art. is associated with a 22% increased risk of stroke [57].
Even if office BP is normal, BP is often elevated in the early morning hours. Thus, an analysis of blood pressure using the method of monitoring it at home (the ACAMPA study) was carried out in Spain in 290 treated patients with hypertension, as well as a study of morning hypertension J-MORE (Jichi Morning-Hypertension Research) in 1027 treated patients with hypertension. Both studies demonstrated that in 60% of hypertensive patients in whom treatment appears to be quite effective, blood pressure remains elevated in the morning [58, 59].
Drug correction of blood pressure variability not only helps prevent MI, stroke, and deaths, but also explains differences in the effectiveness of different antihypertensive drugs in reducing blood pressure. If an antihypertensive drug does not remain fully effective throughout its duration of action, the result may be uncontrolled blood pressure in the morning, even if office blood pressure is normal. A duration of action of the drug of more than 24 hours seems desirable, since many patients are late in taking the next dose, or even completely forget to take it. For a drug to be effective for 24 hours, it is necessary that at least 50% of the peak activity of the active substance is retained by the end of the 24-hour period of action.
Thus, it is necessary to use drugs with a long duration of action to prevent increased BP variability during the day, avoid sharp rises in BP in the morning, and at the same time prevent episodes of sharp decrease in BP. The long-lasting antihypertensive effect and high T/P index allow for more complete organ protection.
Planning the desired level of blood pressure reduction in patients should be based on the compensatory capabilities of cerebral, coronary and renal hemodynamics. The presence of cerebrovascular diseases, coronary heart disease and left ventricular hypertrophy indicates a decrease in the functional reserve of target organs and requires more careful monitoring of the decrease in blood pressure. In the absence of pronounced disturbances in cerebral hemodynamics, it is permissible to reduce SBP by 20% of the initial values, and DBP by 15%. In patients with hypertension, it is advisable to moderately reduce blood pressure by 10–15% from the initial level over 2–4 weeks. followed by a break to allow the patient to adapt to lower blood pressure values. As the patient adapts to new (lower) blood pressure levels, a further gradual decrease in blood pressure to optimal values for the patient is possible. If moving to the next stage causes the patient's condition to worsen, it is advisable to return to the previous level for some more time. The reduction of blood pressure to the target level occurs in several stages, the number of which is individual and depends on both the initial value of blood pressure and the tolerability of antihypertensive drugs. The use of a step-by-step scheme for lowering blood pressure, taking into account individual tolerance, especially in patients with a high and very high risk of cardiovascular disease, allows one to achieve a target blood pressure level of less than 140/90 mm Hg. Art., avoid episodes of hypotension and an increase in the associated risk of developing MI and MI [60].
Conclusion
Currently, the effectiveness of rational AHT has been convincingly proven in relation to both the prevention of cardiovascular events and the progression of target organ damage. On the one hand, it is necessary to prescribe drugs with the help of which the target blood pressure level is achieved, on the other hand, it is necessary to monitor so that the decrease in blood pressure does not fall below 110–115/70–75 mm Hg. Art. Gradual and sustained normalization of blood pressure leads to a decrease in the incidence of myocardial infarction, a decrease in the number of recurrent strokes and mortality from CVD.
Literature
- Arabidze G.G., Belousov Yu.B., Karpov Yu.A. Arterial hypertension. Reference manual for diagnosis and treatment. M., 1999. 139 p.
- Gusev E.I., Martynov M.Yu., Yasamanova A.N. et al. Etiological factors and risk factors for chronic cerebrovascular insufficiency and ischemic stroke // Stroke. 2001. No. 1. P. 41–45.
- Chalmers J., Chapman N. Challengers for the prevention of primary and secondary stroke. The importance of lowering blood pressure and total cardiovascular risk // Blood pressure. 2001. Vol. 10. R. 344–351.
- Diagnosis and treatment of arterial hypertension Russian recommendations (fourth revision) // Systemic hypertension. 2010. No. 3. P. 5–26.
- Guidelines for the Early Management of Adults with Ischemic Stroke. Stroke. 2007. Vol. 38. R. 1655.
- 2013 ESH/ESC Guidelines for the management of arterial hypertension // Journal of Hypertension. 2013. Vol. 31(7). R. 1281–1357.
- The Seventh Report of the Joint National Committee on // NIH Publication. 2003. No. 03–5233.
- Cleland JGF, Dargie HJ, McAlpine H. et al. Severe hypotension after first dose of enalapril in heart failure // Br. Med. J. 1985. Vol. 291. R. 1309–1312.
- Fauci E., Braunwald U., Isselbacher K. Internal medicine according to Tinsley R. Harrison. In 7 vols / per. from English M.: Praktika, 2005. T. 1. P. 249–260.
- Olbinskaya L.I., Martynov A.I., Khapaev B.A. Blood pressure monitoring in cardiology. M.: Russian doctor, 1998. 99 p.
- Olbinskaya L.I., Martynov A.I., Khapaev B.A. Blood pressure monitoring in cardiology. M., “Russian doctor”, 1998, 99 p.
- Heart Disease. A textbook of cardiovascular medicine/ 6th edition. Ed. by E. Braunwald, D. P. Zipes, P. Libby. WB Saunders Company, 2001. R. 933.
- Chazova I.E., Ratova L.G. The role of daily blood pressure monitoring in assessing the effectiveness of antihypertensive therapy (Results of daily blood pressure monitoring in the CLIP-ACCORD program) // Systemic hypertension. 2007. No. 1. P. 18–26.
- Fratolla A., Parati G., Guspidi C. et al. Prognostic value of 24-hour pressure variability // J. Hypertens, 1993. Vol. 11. P. 1133–1137.
- Parfenov V.A., Gorbacheva F.E. Cerebral complications of antihypertensive therapy // Clinical medicine. 1991. No. 10. P. 46–48.
- Parfenov V.A., Zamergrad M.V. What is hidden behind the diagnosis of “hypertensive crisis” // Neurological journal. 1998. No. 5. pp. 41–43.
- Cruickhank JM, Thorp JM, Zacharias FJ Benefits and potential harm of lowering high blood pressure // Lancet.1987. Vol. 1. R. 581–583.
- Arterial hypertension in special categories of patients / ed. V.N. Kovalenko, E.P. Svishchenko. K.: Morion, 2009. P. 54.
- Pantoni L., Garcia JH The significance of cerebral white matter abnormalities 100 years after Binswanger's report. A review // Stroke. 1995 Jul. Vol. 26 (7). R. 1293–1301.
- Pantoni L., Garcia JH Pathogenesis of leukoaraiosis. A review // Stroke. 1997. Vol. 28. R. 652–659.
- Worlow C.P. et al. Stroke. Practical guide for the management of patients / trans. from English St. Petersburg: Politekhnika, 1998.
- Geraskina L.A. Optimization of antihypertensive therapy in patients with dyscirculatory encephalopathy and residual effects of cerebrovascular accidents: Abstract of thesis. dis. ...cand. honey. Sci. M., 2000.
- Irie K., Yamaguchi T., Minematsu K., Omae T. The J-curve phenomenon in stroke recurrence // Stroke. 1993 Dec. Vol. 24 (12). R. 1844–1849.
- Parfenov V.A. Increased blood pressure and antihypertensive therapy for stroke // Consilium medicum. 2004. No. 1. P. 12–15.
- Rothwell PM, Howard SC, Spence JD For the Carotide Endarterectomy Trialist's Collaboration. Relationship between blood pressure and stroke risk in patients with symptomatic carotid occlusive disease // Stroke. 2003. Vol. 34. R. 2583–2592.
- Fonyakin A.V., Geraskina L.A., Suslina Z.A. Prevention of recurrent stroke. Practical recommendations. M., 2007. 48 p.
- Lewington S., Clarke R., Qizilbash N. et al. Age-specific relevance of usual blood pressure to vascular mortality: A meta-analysis of individual data for one million adults in 61 prospective studies // Lancet. 2002; Vol. 360. R. 1903–1913.
- Messerli FH, Kupfer S., Pepine CJ J curve in hypertension and coronary artery disease /// Am J Cardiol. 2005. Vol. 95. R. 160.
- Somes GW, Pabor M, Sborr RI et al. The role of diastolic blood pressure when treating isolated systolic hypertension // Arch Intern Med. 1999. Vol. 159. R. 2004–2009.
- SHEP Cooperative Research Group. Prevention of stroke by antihypertensive drug treatment in older persons with isolated systolic hypertension: Final results of the Systolic Hypertension in the Elderly Program // JAMA. 1991. Vol. 265. R. 3255–3264.
- Zanchetti A. What Blood Pressure level Should Be treated? P. 1967–1983. In. Hypertension Pathophysiology, Diagnosis and Management / Edited by JH Laragh and BM Brener. Raven Press, Ltd., New York, 1990.
- Bulpitt CJ, Palmer AJ, Fletcher AE et al. Optimal blood pressure control in treated hypertensive patients: Report from the Department of Health Hypertension Care Computing Project (DHCCP) // Circulation. 1994. Vol. 90. R. 225–233.
- Reddit AS Essentials of renal physiology. College Book Publishers, East Hanover (NJ), 1999.
- Dzau VJ Renal effects of angiotensinFconverting enzyme inhibition in cardiac failure // Am. J. KidFney. Dis. 1987. Vol. 10. R. 74–80.
- Morrison G. Kidney. In Current medical diagnosis and treatment, eds Tierney LM, McPhee SJ and Papadakis MA Appleton and Lange, Stamford (CT) 1997. P. 832.
- Mancia G., Parati G., Henning M. et al. on behalf of ELSA investigators. Relation between blood pressure variability and carotid artery damage in hypertension: baseline data from the European Lacidipine Study on Atherosclerosis (ELSA) // J Hypertens. 2001.Vol. 19. R. 1981–1989.
- Rothwell PM Limitations of the usual blood-pressure hypothesis and importance of variability, instability and episodic hypertension // Lancet. 2010. Vol. 375. Issue 9718. P. 938–948.
- Rothwell PM, Howard SC, Dolan E., O'Brien E., Dobson JE, Dahlöf B., Sever PS, Poulter NR Prognostic significance of visit-to-visit variability, maximum systolic blood pressure, and episodic hypertension // Lancet. 2010 Mar 13. Vol. 375 (9718). R. 895–905.
- Rothwell PM, Howard SC, Dolan E., O'Brien E., Dobson JE, Dahlöf B., Poulter NR, Sever PS ASCOT-BPLA and MRC Trial Investigators. // Lancet Neurol. 2010. Vol. 9 (5). P. 469–480.
- Effects of beta blockers and calcium-channel blockers on within-individual variability in blood pressure and risk of stroke // Lancet Neurol. 2010 May. Vol. 9 (5). R. 469–480.
- Kobalava Zh.D., Kotovskaya Yu.V. Blood pressure monitoring: methodological aspects and clinical significance. M.: Servier, 1999. P. 70.
- Muntner P., Shimbo D., Tonelli M., Reynolds K., Arnett DK, Oparil S. The Relationship Between Visit-to-Visit Variability in Systolic Blood Pressure and All-Cause Mortality in the General Population: Findings From NHANES III, 1988 to 1994 // Hypertension. Vol. 57(2). R. 160–166.
- Gosse P., Lasserre R., Minifie C., Lemetayer P., Clementy J. Blood pressure surge on rising // J. Hypertens. 2004. Vol. 22. R. 1113–1118.
- Kobalava Zh.D., Kotovskaya Yu.V., Moiseev V.S. Features of the morning rise in blood pressure in patients with hypertension with different variants of the circadian rhythm // Cardiology. 2000. No. 40 (11). pp. 23–26.
- Fagard RH, Thijs L., Staessen JA, Clement DL, De Buyzere ML, De Bacquer DA Night-day blood pressure ratio and dipping pattern as predictors of death and cardiovascular events in hypertension // J Hum Hypertens. 2009 Oct. Vol. 23 (10). R. 645–653. Epub 2009 Feb 19.
- Tseluiko V.I., Karlov S.M. Prognostic value of 24-hour blood pressure monitoring indicators in the acute period of myocardial infarction. Electronic resource https://thrombolysis.org.ua/education/articles/abp-monitoring-ami.
- Alexandria L.G., Tereshchenko S.N., Kobalava Zh.D., Moiseev V.S. Features of the daily blood pressure profile in patients with acute myocardial infarction with left ventricular dysfunction // Cardiology. 2000. No. 1. pp. 21–23.
- Sirenko Yu. M. Arterial hypertension. K.: MORION, 2002. 204 p.
- Cohen MC, Rohtla KM, Lavery CE, Muller JE, Mittleman MA Meta-analysis of the morning excess of acute myocardial infarction and sudden cardiac death // Am J Cardiol. 1997 Jun 1. Vol. 79 (11). R. 1512–1526.
- Willich S.N., Linderer T., Wegscheider K. et al. Increased morning incidence of myocardial infarction in the ISAM Study: absence with prior beta-adrenergic blockade. ISAM Study Group // Circulation. 1989. Vol. 80 (4). R. 853–858.
- Tofler GH, Muller JE, Stone PH et al. Modifiers of timing and possible triggers of acute myocardial infarction in the Thrombolysis in Myocardial Infarction Phase II (TIMI II) Study Group // J Am Coll Сardiol. 1992. Vol. 20 (5). R. 1049–1055.
- Portaluppi F., Tiseo R., Smolensky MH, Hermida RC, Ayala DE, Fabbian F. Circadian rhythms and cardiovascular health // Sleep Med Rev. 2011 Jun 3.
- Tanaka A. et al. Circadian variation of plaque rupture in acute myocardial infarction // Am J Cardiol. 2004. Vol. 93. R. 1−5.
- Kario K., Matsuo T., Kobayashi H. et al. Nocturnal fall of blood pressure and silent cerebrovascular damage in elderly hypertensive patients. Advanced silent cerebrovascular damage in extreme dippers // Hypertension. 1996. Vol. 27. R. 130–135.
- Goldstein IB, Bartzokis G, Hance DB et al. Relationship between blood pressure and subcortical lesions in healthy elderly people // Stroke. 1998. Vol. 29. R. 765–772.
- Sierra C., de la Sierra A., Mercader J. et al. Silent cerebral white matter lesions in middle-aged essential hypertensive patients // J Hypertens. 2002. Vol. 20. R. 519–524.
- Elliott WJ Circadian variation in the timing of stroke onset: a meta-analysis // Stroke. 1998 May. Vol. 29(5). R. 992–996.
- Kario K., Shimada K., Pickering TG Clinical implication of morning blood pressure surge in hypertension // J Cardiovasc Pharmacol. 2003 Dec. Vol. 42. Suppl 1. R. 87–91.
- Redón J., Roca-Cusachs A., Mora-Maciá J. Uncontrolled early morning blood pressure in medicated patients: the ACAMPA study. Analysis of the Control of Blood Pressure using Abulatory Blood Pressure Monitoring // Blood Press Monit. 2002 Apr. Vol. 7(2). R. 111–116.
- Kario K., Ishikawa J., Pickering TG, Hoshide S., Eguchi K., Morinari M., Hoshide Y., Kuroda T., Shimada K. Morning hypertension: the strongest independent risk factor for stroke in elderly hypertensive patients // Hypertens Res. 2006 Aug. Vol. 29 (8). R. 581–587.
Antihypertensive therapy: general rules
Both symptomatic hypertension and hypertension require correction with drugs that have a hypotensive effect. Antihypertensive therapy can be carried out with drugs that differ in their mechanism of action: antiadrenergic agents, vasodilators, calcium antagonists, angiotensin antagonists, and diuretics.
You can obtain information about the hypotensive effect of the drug and what medications to take for high blood pressure not only from your doctor, but also from your pharmacist.
Arterial hypertension is a chronic disease that requires constant drug support, daily monitoring and regular use of prescribed medications. Not only the state of health, but also the life of a person depends on compliance with these rules.
Despite the general availability of treatment rules for reducing blood pressure, many patients have to be reminded what a treatment regimen for hypertension should look like:
- Antihypertensive medications should be taken regularly, regardless of the patient’s well-being and blood pressure level. This allows you to increase the effectiveness of blood pressure control, as well as prevent cardiovascular complications and target organ damage;
- It is necessary to strictly adhere to the dosage and use the form of the drug prescribed by the attending physician. Independently changing the recommended dose or replacing the drug may distort the hypotensive effect;
- even if you are constantly taking antihypertensive drugs, it is necessary to systematically measure blood pressure, which will allow you to evaluate the effectiveness of therapy, timely identify certain changes and adjust treatment;
- in the case of an increase in blood pressure against the background of constant antihypertensive treatment - the development of an uncomplicated hypertensive crisis, an additional dose of a previously taken long-acting drug is not recommended. Blood pressure can be quickly reduced using short-acting antihypertensive drugs.
Antihypertensive therapy: drugs to lower blood pressure
During antihypertensive therapy, several main groups of drugs that help lower blood pressure are currently used:
- beta blockers;
- ACE inhibitors;
- calcium antagonists;
- diuretics;
- angiotensin II receptor blockers.
All of the above groups have comparable effectiveness and their own characteristics that determine their use in a given situation.
Beta blockers
Drugs in this group reduce the likelihood of developing coronary complications in patients suffering from angina pectoris, prevent cardiovascular accidents in patients with myocardial infarction, tachyarrhythmia, and are used in patients with chronic heart failure. Beta-blockers are not recommended for patients with diabetes mellitus, lipid metabolism disorders and metabolic syndrome.
ACE inhibitors
Angiotensin-converting enzyme inhibitors have pronounced hypotensive properties, they have organoprotective effects: their use reduces the risk of complications of atherosclerosis, reduces left ventricular hypertrophy, and slows the decline in renal function. ACE inhibitors are well tolerated and have no negative effects on lipid metabolism and glucose levels.
Calcium antagonists
In addition to antihypertensive properties, drugs in this group have antianginal and organoprotective effects, help reduce the risk of strokes, atherosclerotic lesions of the carotid arteries and left ventricular hypertrophy. Calcium antagonists may be used alone or in combination with other drugs that have antihypertensive properties.
Diuretics
Diuretic drugs are usually used in combination with other antihypertensive drugs in order to enhance the therapeutic effect.
Diuretics are also prescribed to persons suffering from pathologies such as refractory hypertension and chronic heart failure. To avoid the development of side effects, when taking these drugs continuously, minimal dosages are prescribed.
Angiotensin II receptor blockers
Drugs in this group, which have neuro- and cardioprotective effects, are used to improve control of blood glucose levels. They can increase the life expectancy of patients suffering from chronic heart failure. Antihypertensive therapy using angiotensin II receptor blockers can be prescribed to patients who have had a myocardial infarction, suffer from renal failure, gout, metabolic syndrome and diabetes mellitus.
The results of clinical studies that assessed the incidence of certain clinical outcomes indicate that a sustained reduction in blood pressure (BP) leads to a statistically significant reduction in the risk of coronary heart disease (CHD) and stroke [1, 2]. It is an adequate reduction in blood pressure that is considered one of the necessary conditions for effective prevention of complications of cardiovascular diseases (CVD). The results of a meta-analysis of observational studies that included about 1 million people showed that a decrease in systolic blood pressure of only 2 mm Hg. Art. leads to a reduction in the risk of death from coronary artery disease and stroke by 7 and 10%, respectively [3].
Until recently, it was believed that any antihypertensive drugs recommended as first-line drugs were equally effective in reducing the risk of CVD complications [4, 5]. The first doubts about the effectiveness and safety of representatives of certain classes of antihypertensive drugs arose after receiving data from the ALLHAT (Antihypertensive and Lipid–Lowering Treatment to Prevent Heart Attack Trial) study [6] about a 25% increase in the combined risk of nonfatal myocardial infarction (MI) and cardiac death , as well as a twofold increase in the risk of developing heart failure when using the alpha-blocker doxazosin compared with placebo. Although results from the ALLHAT trial indicated similar effects of the thiazide diuretic chlorthalidone, the calcium antagonist (CA) amlodipine, and an angiotensin-converting enzyme (ACE) inhibitor on the primary composite rate of CAD events, evidence has emerged that thiazide diuretics and ACE inhibitors have different effects on the progression of asymptomatic carotid atherosclerosis. Thus, the use of monotherapy with hydrochlorothiazide (HCTZ) is supported by the recently published results of the PHYLLIS (Plaque HYpertension Lipid Lowering Italian Study) study [7], which show that with the use of HCTZ there is a statistically significant progression of atherosclerosis of the carotid arteries, while taking an ACE inhibitor does not accompanied by such changes.
In the ALLHAT trial [6], antihypertensive therapy with an ACE inhibitor resulted in a statistically significant reduction in the incidence of new cases of diabetes mellitus (DM) compared with a thiazide diuretic (odds ratio [HR] at 95% confidence interval [CI] 0.56 to 0.86).
The data presented showed that monotherapy with a thiazide diuretic cannot in all cases be considered the optimal tactics of antihypertensive treatment. It is not surprising that in real clinical practice, thiazide diuretics are used as first-line drugs in no more than 9% of patients [8].
In addition, in the ALLHAT study, during treatment with a thiazide antibiotic, a high incidence of hypokalemia was noted, which required the use of potassium supplements. In the chlorthalidone group, hypokalemia (plasma potassium concentration less than 3.5 mEq/L) after 2 years was observed in approximately 13% of patients, and by the 5th year of therapy, 8% of patients were forced to take potassium supplements. Thus, doubts arise about the validity of the use of diuretics as first-line drugs, at least in some patients with arterial hypertension (AH).
A recent meta-analysis published in the Lancet suggests that beta-blockers have a significantly lower effect on stroke compared with other antihypertensive agents, but no benefit in preventing MI or death [9]. The authors of the meta-analysis, based on the data obtained, express doubts about the validity of the use of beta-blockers as first-line antihypertensive drugs.
Another recent meta-analysis was performed to compare the effectiveness of ACE inhibitors and angiotensin II receptor blockers in reducing the risk of stroke, heart failure and MI [10]. The analysis technique made it possible to compare the effectiveness of drugs of these classes, regardless of their hypotensive effect. It was shown that ACE inhibitors and angiotensin receptor blockers do not differ statistically significantly in their effect on the incidence of stroke and heart failure, but when taking ACE inhibitors, a significant reduction in the risk of MI by 9% was noted. Taking angiotensin II receptor blockers was accompanied by a tendency to increase the risk of developing MI (by 7%). And although a retrospective analysis of data from the CHARM study [11] indicates a reduction in the risk of MI due to the use of candesartan in patients with heart failure, doubts remain about the equal effectiveness of ACE inhibitors and angiotensin receptor blockers in the prevention of MI.
Thus, the presented data from evidence-based medicine suggest that the most acceptable first-line antihypertensive drugs, which effectively reduce the risk of developing most CVD complications and have a positive effect on the course of atherosclerosis, can be considered dihydropyridine AKs and ACE inhibitors.
In the 1990s the results of individual observational studies [5] raised doubts about the safety of the use of dihydropyridine AA. It should be noted that, despite the widespread use of drugs in this class, until 1997 there were no large controlled studies assessing their effectiveness and safety [13]. It is now generally accepted that the best way to assess the effect of treatment on the incidence of adverse clinical outcomes is through randomized clinical trials that prospectively compare the effectiveness of drugs with each other, and in some cases with placebo or no therapy.
Evidence-based basis for the use of amlodipine in the treatment of hypertension
The possibility of preventing stroke using antihypertensive therapy was proven in the earliest randomized clinical trials of antihypertensive drugs, which are either not used today or are considered “old” [14]. The results of a recent meta-analysis [11], which compared the effectiveness of antihypertensive drugs belonging to different classes with placebo or no treatment, indicate the high effectiveness of AC use in the prevention of stroke. The risk of stroke when using beta-blockers, ACE inhibitors, diuretics and AKs was reduced by 29, 31, 34 and 40%, respectively.
The higher effectiveness of AKs compared to ACE inhibitors was confirmed in another meta-analysis performed on the basis of data from 28 clinical studies, including 179,122 patients [16]. It was shown that, in general, the use of AC or ACE inhibitors leads to a reduction in the risk of stroke by 11% compared with the use of beta-blockers and/or diuretics or placebo (p = 0.005). Taking ACE inhibitors compared with placebo was associated with a 16% reduction in the risk of stroke (p = 0.02). At the same time, the use of AC compared to placebo reduced the risk of stroke by 35% (p = 0.001).
The effectiveness of amlodipine and other dihydropyridine AKs is largely determined by their hypotensive effect. It should be noted that differences in BP levels between treatment groups may account for differences in efficacy between groups in several clinical trials [17–19], even in cases where the benefit of one treatment strategy over another was initially explained by a specific drug effect independent of the drug. blood pressure level [18, 19].
However, the effectiveness of amlodipine as a means of preventing CVD appears to be determined not only by its ability to lower blood pressure, but also by the presence of additional properties. The largest comparative clinical trial of antihypertensive drugs, ALLHAT [6], compared amlodipine with the best-studied diuretic, chlorthalidone. Despite the slightly more pronounced hypotensive effect of chlorthalidone compared to amlodipine (the difference in systolic blood pressure is 0.8 mm Hg), the use of AC was accompanied by a tendency to reduce the risk of stroke (by 8%). These data may indicate greater effectiveness of ACs compared to thiazide diuretics in reducing the risk of stroke in patients with hypertension.
The results obtained are very important, since currently reducing the risk of stroke is becoming one of the main goals of antihypertensive therapy. In the United States, stroke has become the third leading cause of death and one of the leading causes of permanent disability. In Russia, by the end of the 1990s. Mortality from stroke was in second place in the structure of overall mortality, second only to ischemic heart disease [20].
In recent years, the idea of the goals of treatment for hypertension has changed somewhat. This concerns, first of all, the need for more careful monitoring of blood pressure levels and its normalization in most patients, and in many cases, the achievement of an optimal level, which may be lower than the values currently recognized as “normal”. It is believed that the goals of effective antihypertensive therapy may be:
- reduction in the relative risk of developing CVD by at least 50% (corresponds to a decrease in systolic blood pressure by approximately 20 mm Hg);
- achieving generally accepted target blood pressure levels (140/90 mm Hg in most patients, 130/80 in diabetes and kidney disease) [21].
In fact, the optimal blood pressure value has not been established, although it is believed that this is the lowest blood pressure level that ensures the normal functioning of the organs and systems of a given body. To achieve this level, the use of more than one antihypertensive drug is usually necessary. Typically, taking one drug reduces systolic blood pressure by approximately 10 mmHg. Art., so it is obvious that to reduce it by 20 mm Hg. Art. combination use of drugs is required. That is why today it is more correct to talk not about the advantages of one class of antihypertensive drugs over another, but about the advantages of certain types of combination antihypertensive therapy.
In light of these ideas, one should refer to the recently published results of the ASCOT-BPLA (Anglo-Scandinavian Cardiac Outcomes Trial - Blood Pressure Lowering Arm) study [22], which compared the effectiveness of preventing CVD complications in antihypertensive therapy based on the use of amlodipine in combination with perindopril and atenolol in combination with bendroflumethiazide (BFT). The effect of these combinations on the incidence of non-fatal myocardial infarction and mortality from coronary artery disease was assessed. It included 19,257 patients aged 40 to 79 years with untreated hypertension (systolic blood pressure ≥ 160 mm Hg and/or diastolic blood pressure ≥ 100 mm Hg) or treated hypertension (systolic blood pressure ≥ 140 mm Hg Art. and/or diastolic blood pressure ≥ 90 mm Hg) in the presence of at least 3 additional risk factors such as:
- left ventricular hypertrophy according to echocardiography or ECG,
- DM type 2;
- peripheral arterial disease;
- previous stroke or transient cerebrovascular accident;
- male gender;
- age ≥ 55 years;
- microalbuminuria or proteinuria;
- smoking;
- ratio of total cholesterol to high-density lipoprotein cholesterol in the blood ≥ 6;
- presence in the family history of indications of cases of premature development of coronary artery disease.
Patients were randomized to treatment groups based on the use of amlodipine with the addition of perindopril if necessary to enhance the hypotensive effect (amlodipine group; n = 9639) or atenolol with the addition of the thiazide diuretic BFT and potassium (atenolol group; n = 9618). The initial dose of amlodipine was 5 mg/day, if necessary it was increased to 10 mg/day.
The initial dose of atenolol was 50 mg/day, if necessary it was increased to 100 mg/day. If the use of amlodipine and atenolol in such doses was not effective enough, perindopril (4–8 mg/day) was added to amlodipine, and BFT (1.25–2.5 mg/day) was added to atenolol. If the desired effect was not achieved, then in both groups doxazosin was added to therapy (4–8 mg/day in the form of a gastrointestinal transport system).
The study was stopped early when the difference between groups in the primary composite endpoint (nonfatal MI or coronary death) had not yet reached statistical significance. The difficult decision to end the study early was due to the fact that there was a statistically significant difference between the groups in almost all additional indicators, including the risk of stroke. In the amlodipine group, its incidence was 23% lower than in the atenolol group (RR 0.77, 95% CI 0.66 to 0.89; p = 0.0003). Thus, the results of the ASCOT-BPLA study finally confirmed previously obtained data on the higher effectiveness of preventive therapy for stroke based on the use of AKs compared to treatment based on the use of beta-blockers and diuretics.
Some opponents of the ASCOT-BPLA study note that the difference in the effectiveness of the two antihypertensive therapy tactics could be largely due to the achievement of lower blood pressure levels in the group of combined use of amlodipine and perindopril compared with the use of atenolol and BFT. S. Yusuf noted the early appearance of differences in blood pressure levels between the amlodipine and atenolol groups [23]. However, this expert agrees with the study authors that differences in blood pressure levels can only partially explain the differences in the incidence of the clinical outcomes studied. Data from many clinical studies show that the difference between the amlodipine and atenolol groups in the level of systolic blood pressure, reaching 2.7 mm Hg. Art., could cause a difference in the incidence of complications of coronary artery disease, equal to 4–8%, and in the incidence of stroke, equal to 11–14%, and according to observational studies, 8 and 11%, respectively [24, 25]. FH Messerli notes that for him as a doctor it does not matter whether the greater effectiveness of one treatment tactic compared to another depends on the severity of the hypotensive effect or on the presence of additional properties of the drugs used [26]. In his opinion, the answer to this question is of interest primarily to researchers and scientists, but not to practicing doctors.
There is another important result of the ASCOT study regarding stroke prevention. It turned out that the most effective prevention of this complication is achieved with the combined use of AK, an ACE inhibitor and a statin. Compared with the use of a beta-blocker and a diuretic, the combined use of amlodipine, perindopril and atorvastatin led to a reduction in the relative risk of fatal and non-fatal stroke by 44% [26].
There is evidence that amlodipine may be superior in tolerability to other known AKs. In a comparative study of compliance with therapy with amlodipine and felodipine in elderly patients with hypertension, it was shown that after a year of treatment in the amlodipine group, the likelihood of discontinuing therapy was 21% lower than in the felodipine group [27].
Possible mechanisms for the high effectiveness of amlodipine in the treatment of hypertension
Since there is a relationship between elevated blood pressure levels and the risk of stroke, one of the mechanisms determining the high effectiveness of ACs in the prevention of this complication may be their rather pronounced hypotensive effect. A greater reduction in blood pressure with AA compared to other drugs was observed in several randomized clinical trials, for example, VALUE (Valsartan Antihypertensive Lon gamma-term Use Evaluation) [28] and ASCOT-BPLA [19]. This more pronounced hypotensive effect was accompanied in the VALUE study by a clear trend towards a 15% reduction in the incidence of stroke in the amlodipine group compared with the valsartan group (p = 0.08). In the ASCOT-BPLA [19] and FEVER (Felodipine EVent Reduction) studies [29, 30], even a small difference in blood pressure between the AC group and the control group was accompanied by a statistically significant reduction in the risk of stroke.
And yet, why is there such a small difference in systolic blood pressure in the ASCOT-BPLA study - 2.7 mm Hg? Art. – was there such a significant difference in the incidence of stroke between the amlodipine and atenolol groups? Part of the answer to this question was obtained in the CAFE (Conduit Artery Function Evaluation) study [31], which was planned as part of the main ASCOT study. CAFE, which included more than 2000 participants in the pivotal ASCOT trial, assessed the effect of 2 antihypertensive treatment strategies on central aortic pressure measured using a noninvasive technique using the US FDA-approved Sphygmocor system (AtCor Medical).
After measuring the pressure in the radial artery, the computer system generated a pulse wave, the evaluation of which allowed the pressure in the large arteries to be measured. It turned out that with almost the same level of blood pressure measured in the brachial artery, the central systolic blood pressure was 4.3 mm Hg. Art., and the central pulse pressure in the aorta is 3.0 mm Hg. Art. lower with treatment tactics based on amlodipine compared with tactics based on the use of atenolol.
The results of the CAFE study suggest that for the same blood pressure measurements on the arm, the pressure in the central arteries can differ significantly when using antihypertensive drugs, which have different effects on the so-called reflected waves. In particular, amlodipine, due to its active vasodilating effect, more effectively reduces the severity of reflected waves compared to beta-blockers and diuretics. When using a drug with a vasodilating effect, the power of reflected waves weakens, which is accompanied by a decrease in central blood pressure. The CAFE study authors suggest that the statistically significant difference in clinical efficacy between amlodipine and atenolol observed in the ASCOT study can largely be explained by their different effects on central arterial pressure.
The positive effect of long-acting OCs on the risk of stroke may be partly due to their effect in preventing increases in blood pressure in the morning. There is convincing evidence of a connection between morning increases in blood pressure and the risk of stroke [32]. With an increase in blood pressure in the morning and without it, the incidence of stroke over 3.5 years was 19.0 and 7.3%, respectively (p = 0.004). Morning increase in systolic blood pressure by 10 mm Hg. Art. is accompanied by an increase in the risk of stroke by 22–25% [32, 33]. In a comparative study of amlodipine and valsartan, it was shown that the use of AK allows a statistically significant reduction in the level of systolic blood pressure in the morning compared with an angiotensin II receptor blocker (p < 0.02) [34].
The results of a clinical study that included 106 patients with mild and moderate hypertension indicate that the combined use of a small dose of amlodipine (5 mg/day) and an average therapeutic dose of an ACE inhibitor leads to a more pronounced increase in arterial distensibility compared to the use of maximum therapeutic doses of drugs [35]. When using combined therapy, maximum doses of amlodipine and ACE inhibitor, distensibility increased by 0.71 ± 0.51, 0.28 ± 0.69 and 0.39 ± 0.62% ml/mmHg. Art. The use of combination therapy also led to a statistically more pronounced regression of left ventricular myocardial hypertrophy compared to monotherapy with each drug (p < 0.02). These data may be the basis for wider use of combination drugs containing amlodipine and an ACE inhibitor.
Efficacy and safety of dihydropridine ACs for the prevention of stroke in patients with diabetes
In 1999, a review was published in the New England Journal Medicine, which noted that “the use of AA in diabetes may lead to an increased risk of developing CVD” [36]. This opinion was based on an analysis of limited data obtained from clinical trials [37, 38]. The results of a meta-analysis of randomized clinical trials, which were published in 2004, completely refuted the above statement [39]. It was shown that the use of AC in patients with diabetes led to a statistically significant reduction in overall mortality and the incidence of all adverse clinical outcomes associated with heart disease, as well as stroke, compared with placebo.
In patients with diabetes, the use of AC had a similar effect on the risk of developing coronary artery disease and overall mortality as standard therapy, while causing a slight reduction in the risk of stroke (HR = 0.87; p = 0.08) [39]. Thus, the use of AC in patients with diabetes turned out to be an effective and safe method for preventing most CVD complications and death from them. However, the use of ACs did not reduce the risk of heart failure, especially compared with drugs that suppress the activity of the renin-angiotensin system, although drugs of these classes had a similar effect on overall mortality and the incidence of stroke or coronary artery disease. It should, however, be taken into account that the diagnosis of “heart failure” during the use of AC may be established erroneously and be a consequence of slight fluid retention.
It is also known that in patients with diabetes, monotherapy with non-dihydropyridine AA is more effective in reducing the severity of proteinuria than monotherapy with dihydropyridine drugs of this class. However, with the combined use of AKs and ACE inhibitors, such a difference, according to FH Messerli [26], may become clinically insignificant.
Thus, the results of recently completed clinical studies indicate that amlodipine, both due to its fairly powerful hypotensive effect and due to the likely presence of additional properties, is becoming one of the main drugs for the treatment of CVD, since its use not only reduces the symptoms of the disease , but also reduce in many cases the risk of developing such severe complications of CVD as MI, stroke and premature death.
Evidence-based basis for the selection of drugs for combination antihypertensive therapy
The theoretical basis for the combined use of dihydropyridine AA and ACE inhibitors can be data from randomized clinical trials, the results of which indicate a higher effectiveness of initial therapy with drugs of these two classes compared with monotherapy of each of them [40].
The justification for the use of ACE inhibitors as part of combined antihypertensive drugs is determined by the fact that their use not only leads to a decrease in blood pressure, but also allows one to achieve other goals of therapy, including regression of left ventricular hypertrophy [41]. Being an important indicator of target organ damage, left ventricular myocardial mass is considered the most informative prognostic factor for the development of adverse clinical outcomes in patients with hypertension. According to a comparative analysis of the effectiveness of diuretics, AC, beta-blockers and ACE inhibitors, the latter cause the greatest regression of hypertrophy [42, 43]. ACE inhibitors also have a nephroprotective effect [44]. Some ACE inhibitors, in particular lisinopril, have been shown to reduce not only the severity of left ventricular hypertrophy, but also myocardial fibrosis, which is accompanied by an improvement in diastolic heart function [45].
The combined use of a dihydropyridine AK and an ACE inhibitor can be considered an effective treatment tactic for patients with isolated systolic hypertension, since in this case a more pronounced reduction in systolic blood pressure is provided than with monotherapy with these drugs [46]. To make a final judgment about the prospects of the combined use of amlodipine and an ACE inhibitor for the treatment of isolated systolic hypertension, a large clinical trial, Avoiding Cardiovascular events through COMbination therapy in Patients LIving with Systolic Hypertension (ACCOMPLISH) [47], which is planned to include more than 6000 patients with hypertension, is currently being conducted. .
The occurrence of peripheral edema is considered a common complication of dihydropyridine ACs [48] and often becomes the reason for refusal to continue therapy. The occurrence of such edema is due to a pronounced expansion of the lumen of the arterioles while maintaining the same diameter of the lumen of the venules. In this case, insufficient blood outflow from peripheral tissues causes the formation of edema. Additional use of diuretics for these edemas may be ineffective. The combined use of amlodipine and an ACE inhibitor, compared with therapy with AA alone, can almost halve the incidence of edema due to the venodilating effect of ACE inhibitors [48].
Evidence-based basis for the use of lisinopril as part of combination therapy
The choice of any drug for the treatment and prevention of CVD largely depends on the availability of evidence of the effectiveness of its use in at least one of these diseases. Data on the effectiveness of using even small doses of lisinopril in the treatment of heart failure were obtained in the large clinical trial ATLAS (Assessment of Treatment with Lisinopril And Survival) [49]. At the same time, the safety of using high doses of lisinopril was noted [50], which is especially important for patients with hypertension, in whom an increase in the dose of the ACE inhibitor may be required to achieve the necessary hypotensive effect. The results of a secondary analysis of data from 3164 participants in the ATLAS study who had a high risk of developing CVD complications (including patients with diabetes) confirmed the safety of high-dose lisinopril [51].
Further justification for the widespread use of lisinopril in the treatment of hypertension, especially in patients with metabolic syndrome, is data from the ALLHAT trial, indicating that the use of this drug led to a 32% reduction in the risk of developing new cases of diabetes compared with the use of chlorthalidone (RR 0 .68 with 95% CI from 0.50 to 0.80; p = 0.01). At the same time, lisinopril in preventing the development of diabetes was more effective than amlodipine, treatment of which led to a reduction in the risk of developing diabetes by only 21% [6].
The effectiveness of lisinopril in hypertension has been proven in several randomized clinical trials. According to the multicenter placebo-controlled TROPHY (Treatment in Obese Patients With Hypertension) study, lisinopril monotherapy was not inferior to HCTZ monotherapy in terms of the effectiveness of lowering blood pressure in hypertensive patients with obesity [52]. However, it should be noted that in 57% of patients in the lisinopril group, the initial dose of the drug (10 mg/day) was effective, while in the HCTZ group, half of the patients needed to increase the dose of the drug to the maximum (50 mg/day).
The high effectiveness of the combined use of lisinopril and amlodipine was confirmed in a small prospective study that included 98 patients with hypertension [53]. The combined use of these drugs led to a significant decrease in systolic (from 197.7 ± 18.1 to 139.9 ± 10.5 mm Hg) and diastolic blood pressure (from 107.1 ± 13.1 to 82.6 ± 5 .5 mmHg). Treatment was well tolerated - therapy was discontinued in only 3 patients due to the development of swelling of the legs and dry cough.
Recently, when assessing the effectiveness of antihypertensive drugs, they are increasingly focusing on the so-called surrogate evaluation criteria. The results of a small study indicate that the use of lisinopril in elderly patients with systolic hypertension led to a pronounced hypotensive effect, increased blood flow through the cerebral vessels and increased distensibility of the carotid arteries, but did not cause cerebral hypoperfusion [54]. At the same time, there was a decrease in vascular resistance without disruption of autoregulation of cerebral circulation.
The results of the ELVERA study (Effects of amlodipine and lisinopril on Left Ventricular mass) [55], which included patients aged 60–75 years with newly diagnosed hypertension, indicate a statistically significant decrease in the total thickness of the intima and media of the carotid arteries while taking lisinopril (by 0.065 mm) and amlodipine (by 0.089 mm). These data indicate the antiatherosclerotic effect of the drugs.
Microalbuminuria is considered one of the main risk factors for the development of CVD complications, and its reduction is accompanied by a decrease in the incidence of adverse clinical outcomes. Data obtained in the EUCLID (EURODIAB Controlled Trial of Lisinopril in Insulin–Dependent Diabetes Mellitus) study [56] indicate the effectiveness of lisinopril in slowing the progression of renal dysfunction in patients with type 1 diabetes in the presence of microalbuminuria. However, therapy with lisinopril did not lead to an increase in the risk of hypoglycemia.
Thus, according to modern concepts, the optimal tactics of combination antihypertensive therapy in many patients includes the combined use of a long-acting dihydropyridine AA, for example amlodipine, and one of the ACE inhibitors with proven effectiveness, which includes lisinopril.