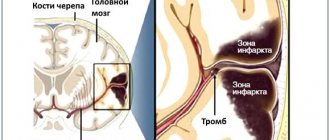
During the diagnostic process, a Chiari or Hiari network was discovered in the right atrium, although I did not feel any special symptoms. What is it, is it dangerous to health, will there be problems in the future and what should be done?
Chiari vasculature (Chiari)
Hello. The Chiari network in the right atrium is a non-pathological, mobile, thin mesh-like structure in the right atrium that is visible on an ultrasound monitor from any position where the inferior vena cava enters the atrium. That is, the mesh consists of remnants of the embryonic coronary sinus valve, which are attached to the Eustachian valve of the inferior vena cava on one side, and on the other to parts of the right atrium (RA). It is discovered truly by chance when diagnosed in 1-2% of the population.
To be more precise, this congenital abnormal structure of the heart in the form of a reticular plate with holes - the atrial septum - begins at the valve of the coronary sinus (Tebesian valve) and the valve of the inferior vena cava (Eustachian valve). It can block the atrium to some extent.
The plate can have different positions, but is generally attached slightly anterior to the Lower (intervenous) tubercle. The Chiari network appears due to insufficient reduction of the right (less often left) sinus valve or due to a false septum. An extended flap of the Eustachian valve and the Chiari network are considered a normal variant.
Treatment process
Drug therapy and physical therapy
If patients experience severe headaches, pain in the neck, muscles and joints, they are prescribed the following groups of drugs:
- Painkillers – “Ketorol”, “Pentalgin”, “Analgin”.
- NSAIDs to reduce pain - Meloxicam, Ibuprofen, Voltaren.
- Muscle relaxants for relieving tension in the neck muscles - “Mydocalm”, “Sirdalud”.
Pathogenetic treatment of the syndrome includes:
- Drugs that improve cerebral circulation - Piracetam, Vinpocetine, Cinnarizine.
- Diuretics to reduce the formation of cerebrospinal fluid and for the purpose of dehydration - Furosemide, Mannitol.
- B vitamins that support the functioning of the nervous system at an optimal level and have an antioxidant effect - “Thiamine”, “Pyridoxine”. The most common vitamin products are “Milgamma”, “Neuromultivit”, “Kombilipen”.
If the patient’s condition is considered extremely serious, he is hospitalized immediately in the intensive care unit. There, the patient is connected to a ventilator, existing cerebral edema is eliminated, infectious pathologies are prevented and neurological disorders are corrected.
Physiotherapeutic effects complement drug treatment, allow you to quickly achieve positive results, accelerate the processes of restoration of body functions and recovery of patients. Neurologists prescribe:
- Cryotherapy, which has an analgesic effect, stimulates the performance of the endocrine glands and strengthens the immune system.
- Laser treatment that improves trophism and microcirculation in the affected area.
- Magnetotherapy, which has a general healing effect and triggers the body's internal reserves.
Currently, kinesiology therapy, which is aimed at developing mental abilities and achieving physical health through movement exercises, is especially popular. It is also included in the treatment regimen for this syndrome.
Treatment is not carried out at all if the pathology was discovered by chance, during a tomographic examination for a completely different reason, and the patient does not have any characteristic symptoms. Specialists conduct dynamic monitoring of the condition of such patients.
Surgery
Persistent neurological disorders with paresthesia, muscle dystonia, paralysis and paresis require surgical correction. Surgery is also indicated in cases where drug therapy does not produce a positive result. The operations have one goal - eliminating compression and pinching of the brain, as well as restoring normal circulation of the cerebrospinal fluid.
Currently, neurosurgeons save the lives of patients by performing decompressive and bypass operations. In the first case, a part of the occipital bone is cut out in order to expand the large hole, and in the second, a bypass is created for the outflow of cerebrospinal fluid through the implantation tubes in order to reduce its volume and normalize intracranial pressure.
After surgery, all patients are recommended to undergo rehabilitation measures. If the treatment was successful, patients regain lost functions - respiratory, motor, cardiovascular, nervous. The pathology may recur within three years. In such cases, patients are recognized as disabled.
Video: about surgery for Arnold-Chiari syndrome
ethnoscience
Folk remedies used for this pathology eliminate pain and relax tense muscles. They effectively complement traditional therapy for the syndrome.
The most popular means:
- Marshmallow infusion for applying compresses,
- Warming the affected area with a hot chicken egg,
- Honey compresses,
- decoction of fern or raspberry for oral administration.
Conclusion
The network itself is not clinically significant, but it is often associated with pathologies: patent foramen ovale (PFO), intraatrial thrombosis, or atrial arrhythmias. The Chiari mesh is complicated by thrombosis followed by thromboembolism, but no treatment is prescribed because it blocks the progression of the thrombus and is a rudiment of the coronary sinus valve.
A reticulate plate with holes has no practical significance. But to detect it, an unusual diagnosis is made, which does not exclude a medical error. Therefore, it is important to perform a thorough echocardiography, which during cardiovascular interventions will make it easier to overcome the difficulties when performing catheterization in the coronary sinus or right heart.
Symptoms
What is vestibulo-atactic syndrome?
Clinical manifestations of Budd-Chiari syndrome may vary slightly depending on what form of pathology is present. With the development of an acute type of disease, a person’s liver becomes enlarged, pain in the lower part of the sternum, nausea, vomiting, general weakness, and fatigue are observed.
To diagnose Budd Chiari syndrome, the doctor must see obstruction of 2 or more veins. Only in this case the symptoms of the disease become noticeable.
The liver begins to enlarge to such an extent that the liver capsule is stretched. This symptom of the syndrome is very painful.
The enlargement particularly affects the caudate lobe of the liver.
Depending on the level of blood stagnation in the hepatic vein, liver function may also be impaired. The consequence of this is hypoxia or oxygen starvation.
This symptom of the disease leads to partial destruction of the liver.
Budd Chiari syndrome develops due to problems with blood clotting. In this case, the following signs appear:
- ascites;
- jaundice;
- enlarged spleen;
- liver enlargement.
Budd Chiari disease has several clinical forms:
- The subacute and acute form is characterized by ascites, an immediate increase in pain in the abdomen, enlarged liver, bloating, jaundice and the appearance of renal failure;
- The syndrome most often occurs in a chronic form. In this case, jaundice may be absent, but ascites only progresses. More than 50% of patients who have this disease suffer from kidney failure;
- The most common form of Budd Chiari syndrome is the fulminant form. With it, all the clinical symptoms of the disease increase very quickly.
Vessels of different sizes can suffer from obstruction in this syndrome. The symptoms of Budd-Chiari syndrome, or rather, the degree of their severity, directly depend on how many veins supplying the liver are damaged.
A hidden clinical picture is observed when the functioning of one vein is disrupted. In this case, the patient does not feel any disturbances in well-being and does not notice the pathological manifestations of the disease.
However, if two or more veins are involved in the process, then the body begins to react to the violation quite violently.
Symptoms of the acute stage of the disease:
- Sudden onset.
- The appearance of high-intensity pain in the right hypochondrium and in the abdomen.
- The appearance of nausea accompanied by vomiting.
- The skin and sclera of the eyes turn moderately yellow.
- The liver increases in size.
- The legs swell greatly, the veins throughout the body swell and protrude from under the skin. This indicates the involvement of the vena cava in the pathological process.
- If the functioning of the mesenteric vessels is disrupted, the patient develops diarrhea, pain spreads to the entire abdominal cavity.
- Renal failure with ascites and hydrothorax develops several days after the onset of the disease. The patient's condition is worsening every day, bloody vomiting develops, drug correction helps little. Vomiting blood most often indicates that the veins of the lower third of the esophagus have ruptured.
The classic triad of abdominal pain, ascites and hepatomegaly is observed in the vast majority of patients with Budd-Chiari syndrome, but this triad is nonspecific.
However, if collaterals have developed in the liver, such patients may remain asymptomatic or may have only a few symptoms or manifestations. However, in some individuals with this syndrome, this asymptomatic state may progress to liver failure and portal hypertension with associated symptoms (eg, encephalopathy, hematemesis).
Below is a list of clinical variants of Budd-Chiari syndrome:
- Acute and subacute forms: characterized by rapid development of abdominal pain, ascites, hepatomegaly, jaundice and renal failure.
- Chronic form: most common form, patients are admitted to hospital with progressive ascites, no jaundice, approximately 50% of patients have impaired renal function
- Fulminant form: an unusual form of the syndrome. Individuals with this form may quickly develop liver failure, along with ascites, hepatomegaly, jaundice and renal failure.
Patients with obstruction typically have acute pain in the right upper quadrant. Bloating can also be an important sign. Jaundice is rare.
Physical examination
A physical examination may reveal:
- Jaundice
- Ascites
- Hepatomegaly
- Splenomegaly
- Swelling of the ankles
Thrombosis of the heart chambers after surgical interventions under artificial circulation (CPB) is a rare and little-studied pathology. Most often, these conditions occur with antiphospholipid syndrome (APS) and other thrombophilias.
The main predisposing factors for thrombus formation in the cavities of the heart are the presence of an obstruction to blood flow, septal defects (congenital and acquired defects of the heart and great vessels), heart rhythm disturbances (atrial fibrillation, atrial flutter), the presence of an intravenous catheter, endocardial electrodes, changes in the blood coagulation system, including including transient ones. In a number of observations, the cause remains unidentified [5]. One of the mechanical causes of thrombus formation and pathological thromboembolism includes a developed Chiari network (incompletely reduced remnants of the venous sinus valve in the right atrium (RA) in the area of the mouth of the inferior vena cava). It can serve as a “trap” for thromboembolism and subsequently as a site for thrombus formation [6].
Various authors [1—3, 5] propose the use of conservative (thrombolytic, antiplatelet and anticoagulant) therapy with varying degrees of effectiveness, as well as surgical correction, for the treatment of patients with thrombosis of the cardiac cavities.
In the available literature [3, 4], we found descriptions of 4 observations of RA thrombosis with the site of thrombus fixation to the Chiari network, which occurred in the delayed period after correction of a congenital heart defect - atrial septal defect (ASD) under CPB.
We present our own description of a rare observation of RA thrombosis in the area of the Chiari network after correction of a congenital heart defect.
Patient K., 14 years old, was admitted to the Federal Research Center for Transplantology and Artificial Organs with a diagnosis of congenital heart disease - MPP defect. She complained of weakness and fatigue during physical activity.
According to X-ray data, the heart is enlarged in volume due to the right sections, signs of hypervolemia of the pulmonary circulation.
The ECG shows sinus rhythm, heart rate up to 80 beats/min, normal position of the electrical axis of the heart, incomplete blockade of the right bundle branch.
According to echocardiography (body weight 53 kg, height 160 cm, body surface area 1.54 m2): end-diastolic size (EDD) of the right ventricle (RV) 3.3 cm; PP 3.7×3.6 cm; Left ventricular (LV) EDV 4.3 cm, end systolic dimension (ESD) 2.8 cm, ejection fraction (EF) 66%; thickness of the interventricular septum (IVS) 0.8 cm; thickness of the posterior wall of the left ventricle (PLW) 0.8 cm; aortic diameter at the level of the fibrous ring is 1.7 cm; pulmonary artery (PA) pressure 30 mm Hg; blood flow speed in the aorta 0.96 m/s; blood flow speed in the LA is 1.36 m/s. In the area of the MR at its lower edge, color Doppler mapping reveals a turbulent oblique flow into the RA cavity, up to 2.1 cm in diameter, with blood discharge from left to right.
Coagulogram before surgery: activated partial thromboplastin time (aPTT) 32 s, prothrombin index 86%, fibrinogen 2600 mg/l, soluble fibrin-monomer complexes (SFMC) 5 mg%. Platelet aggregation with adrenaline is 97% versus 72%, with ADP - 99% versus 87%.
General blood test, general urinalysis, biochemical blood test without any features.
The defect was hemodynamically significant and was subject to surgical correction.
On January 10, 2013, an operation was performed - plastic surgery of the IV defect with a xenopericardium patch under IR conditions. Intraoperatively, during revision, there was an IV defect without a lower edge, measuring 1.8×3.0 cm. In the area of the mouth of the inferior vena cava (IVC), the septum was 5 mm wide, thinned, with multiple fenestrations. Excision of the perforated part of the septum was performed. The defect is closed with a patch of xenopericardium, fixed with four U-shaped sutures (Prolene 4/0) along the posterior semicircle of the IVC and a continuous wrapping suture along the remaining perimeter. When checked, the MPP is sealed.
The postoperative period proceeded without complications. Antibacterial, anti-inflammatory, and desensitizing therapy was carried out. On the 8th day, in satisfactory condition, the patient was discharged under the supervision of a pediatrician and cardiologist at her place of residence. According to the control examination: the ECG shows a sinus rhythm, regular, heart rate 91 beats/min, incomplete blockade of the right bundle branch. With echocardiography, RV EDR is 1.8 cm; PP 2.9×3.2 cm; LV ESD 4.3 cm, LV ESD 2.8 cm; FI 66%; IVS 0.8 cm; PA pressure 25 mm Hg; blood flow speed in the aorta 1.1 m/s; blood flow speed in the LA is 1.12 m/s. Pathological flows in the MPP area are not determined. A consultation at the clinic after 6 months is recommended.
At home, 2 months after discharge, episodes of fever up to 37.3 °C were observed for 2 days against the background of catarrhal symptoms. Symptomatic therapy was carried out with a positive effect.
During a planned control echocardiography 6 months after surgery, a RV ECD of 1.8 cm, RA 4.4×3.8 cm, FI 67% was revealed, the MSP area was intact, a mobile space-occupying RA pedunculated formation was visualized (2.5×1.7 cm), prolapsing into the tricuspid valve (Fig. 1).
Figure 1. Transthoracic echocardiography of the heart of patient K. A mass formation is visualized in the cavity of the right atrium.
The patient was urgently hospitalized. Upon admission, the condition was satisfactory, there were no complaints. According to X-ray multislice computed tomography and magnetic resonance imaging of the chest organs, an additional soft tissue formation of an irregular “grape-shaped” shape measuring 45x30x25 mm, movable, hanging over the mouth of the IVC and prolapsing into the tricuspid valve is determined in the RA cavity (Fig. 2) .
Figure 2. Magnetic resonance computed tomography of patient K. On the left is a mass formation in the cavity of the right atrium, on the right is a mass lesion protruding through the tricuspid valve into the right ventricle.
A differential diagnosis was made between a thrombus and a neoplasm of the PP.
Coagulogram: aPTT 32 s, prothrombin index 82%, fibrinogen 3090 mg/l, RKFM 22 mg%, platelet aggregation with adrenaline 88% versus 44%, with ADP - 86% versus 57%, with ristomycin - 94% versus 72%, antithrombin-3 97% (normal 75-125%), plasminogen 99% (normal 75-150%), D-dimer 523 ng/ml (normal ≤500 ng/ml), protein C 94% (normal 70-130% ).
An increase in D-dimer levels could indicate the possible presence of an organized thrombus in the body in the lysis stage. The formation was regarded as a floating PP thrombus, and the patient underwent surgery for vital indications (due to possible pulmonary embolism).
Intraoperatively: due to the risk of thrombus destruction and pulmonary embolism, IVC cannulation was performed under visual control through the opened RA. The intervention was performed on a beating heart (CPB duration 17 min) and normothermia. When revising the PP in the area of the IVC mouth, the Chiari network is visible, to which a multi-lobular formation (4.2×2.9×1.2 cm) of dense consistency, shaped like a cauliflower, is fixed (see Fig. 3 on the color insert).
Figure 3. Macroscopic specimen of an extracted thrombus attached to a Chiari network (on tweezers). In the area of plastic surgery, the IVS is intact, the patch is endothelialized, and there is no connection between the patch and the neoplasm. No other formations were identified in the RA cavity. Excision of the Chiari network was performed en bloc with the formation.
According to the pathomorphological examination, the formation excised during the operation had a variegated appearance on the section from pink to gray-white with a thin strand of the Chiari network extending from it.
Histological examination (see Fig. 4 on color insert)
Figure 4. Microscopic examination of a remote mass. a — erythrocyte thrombus, Masson staining, uv. 400; b - area of white (leukocyte) thrombus, Masson staining, uv. 400; c — areas of fibrin thrombus at the stage of organization, stained with hematoxylin and eosin, UV. 400; d - close connection of the thrombus (left, red color) with the Chiari network (right, blue color), Masson stain, uv. 400; d — organization of a thrombus in the area of the Chiari network, Masson staining, uv. 400; e — Chiari network, Masson staining, uv. 100. It was established that the removed formation was a thrombus of mixed structure: erythrocyte, leukocyte, fibrin, the degree of maturity of which was different, from a fibrin network to homogeneous eosinophilic clumps. The base of the thrombus was attached to a Chiari network. In these areas, the thrombus was in a state of organization, proliferation of connective tissue cells and the formation of collagen fibers were noted. Thus, there was recurrent Chiari network thrombosis. The Chiari network itself was a connective tissue fibrous structure covered with endothelium.
The postoperative period proceeded without complications. On the 2nd day after surgery, prophylactic anticoagulant (Fragmin) and antiplatelet (Cardiomagnyl) therapy was started, and on the 4th day, warfarin was started. When the target international normalized ratio (INR) of 2.0-2.5 fragmin is reached, the treatment is cancelled. On the 7th day, the central venous catheter was removed and the sutures were removed.
The patient was examined to identify APS and hereditary thrombophilias. Antibody titers to phospholipids IgG, phospholipids IgM, cardiolipin, IgG, cardiolipin, IgM, b2 glycoprotein I, IgG, b2 glycoprotein I, IgM, annexin V, IgG, annexin V, IgM were below the reference values, which made it possible to exclude APS. Data confirming genetic pathology (Leiden mutation, prothrombin gene mutation) were not obtained.
Ultrasound examination of the veins of the lower extremities and pelvis did not reveal any evidence of thrombosis.
On the 10th day, the patient was discharged from the hospital in satisfactory condition under the supervision of a cardiologist and hematologist at her place of residence. At discharge, aPTT was 34 s, prothrombin index 59%, fibrinogen 3102 mg/l, EKFM 28 mg%, platelet aggregation with adrenaline 25% versus 20%, with ADP - 78% versus 40%, D-dimer 1082 ng/ml (< 500), INR 2.79.
During routine examinations 1, 3 and 6 months after surgery, no data were obtained confirming a neoplasm of the heart and great vessels. The patient's condition is satisfactory, there are no complaints. Antiplatelet (cardiomagnyl) and anticoagulant (warfarin) therapy continues, INR is maintained within 2.0-2.5.
Discussion
Our observation should obviously be considered as spontaneous thrombosis of the Chiari network after correction of congenital heart disease under cardiopulmonary bypass, in the absence of pathological prerequisites (APS, thrombophilia). It is impossible to exclude the fixation of a microembolus in the Chiari network as a trigger for thrombus formation, although there were no vascular catheters in the veins of the lower extremities.
To prevent such complications, all patients with a relevant history (venous thrombosis, recurrent miscarriage) require careful additional examination in order to identify coagulopathies, thrombophilias or APS. The threat of thrombosis of the cardiac cavities in the postoperative period is the reason for in-depth preoperative examination and appropriate therapy after surgery.
The question of the advisability of preventive resection of the Chiari network when it is detected during the primary operation as a measure to prevent postoperative RA thrombosis is controversial [6].
Literature
- Neurology and neurosurgery: textbook: in 2 volumes/E. I. Gusev, A. N. Konovalov, V. I. Skvortsova. — 2nd ed., rev. and additional - M.: GEOTAR-Media, 2010. - T.1: Neurology. — 624 p.:ill.
- KLEKAMP, J., SAMII, M., "Syringomyelia". Spinger-Verlang 2002, pag. 65.
- AGHAKHANI, J., PARKER, F., TADIE, M. (1999). “Syringomyelia and Chiari abnormality in the adult. Analysis of the results of a comparative series of 285 cases". Neurochirurgie 45(Suppl. 1): 23-36.
- LORENZO, D.N., FORTUNA, A., GUIDETTI, B. (1982) “Craneovertebral junction malformations. Cranioradiological findings, long term results and surgical indications in 63 cases. J Neurosurg 57: 603–608.
- PAUL, K. S., LYE, R. H., STRANG, F. A., DUTTON, J. (1983). "Arnold-Chiari Malformation. Review of 71 cases. J Neurosurg 58:183–187.
Astheno-neurotic syndrome
Symptoms
Iliotibial tract syndrome
The clinical picture of Budd-Chiari syndrome is determined by its form. The main reason that forces a patient to see a doctor is pain that deprives sleep and rest.
- The acute form of the pathology occurs suddenly and is manifested by sharp pain in the abdomen and right hypochondrium, dyspeptic symptoms - vomiting and diarrhea, jaundice of the skin and sclera, hepatomegaly. Swelling of the legs is accompanied by expansion and bulging of the saphenous veins in the abdomen. Symptoms appear unexpectedly and progress quickly, worsening the general condition of patients. They move with great difficulty and can no longer care for themselves. Kidney dysfunction develops rapidly. Free fluid accumulates in the chest and abdominal cavity. Lymphostasis appears. Such processes are practically untreatable and end in coma or death of patients.
- Signs of the subacute form of the syndrome are: hepatosplenomegaly, hypercoagulability syndrome, ascites. Symptoms increase over the course of six months, and the patients’ ability to work decreases. The subacute form usually becomes chronic.
- The chronic form develops against the background of thrombophlebitis of the liver veins and the growth of fibrous fibers into their cavity. It may not manifest itself for many years, that is, it may be asymptomatic, or it may manifest itself with signs of asthenic syndrome - malaise, weakness, fatigue. In this case, the liver is always enlarged in size, its surface is dense, the edge protrudes from under the costal arch. The syndrome is identified only after a comprehensive examination of patients. Gradually, they develop discomfort and unpleasant sensations in the right hypochondrium, lack of appetite, flatulence, vomiting, icterus of the sclera, swelling of the ankles. The pain syndrome is moderate.
- The fulminant form is characterized by a rapid increase in symptoms and progression of the disease. In just a matter of days, patients develop jaundice, kidney dysfunction, and ascites. Official medicine knows of isolated cases of this form of pathology.
In the absence of supportive and symptomatic therapy, severe complications and dangerous consequences develop:
- internal bleeding,
- dysuria,
- increased pressure in the portal system,
- varicose veins of the esophagus,
- hepatosplenomegaly,
- cirrhosis of the liver,
- hydrothorax, ascites,
- hepatic encephalopathy,
- hepatorenal insufficiency,
- bacterial peritonitis.
a consequence of increasing portal hypertension – the “head of the jellyfish” symptom and ascites (right)
At the final stage of progressive liver failure, a coma occurs, from which patients rarely emerge and die. Hepatic coma is a disorder of the central nervous system caused by severe liver damage. The comatose state is characterized by a consistent development. At first, patients experience an anxious, excited or sad, apathetic state, often euphoria. Thinking slows down, sleep and orientation in space and time are disrupted. Then the symptoms worsen: patients become confused, scream and cry, and overreact to ordinary events. Symptoms of meningism, “liver” odor from the mouth, hand tremors, hemorrhages in the oral mucosa and gastrointestinal tract appear. Hemorrhagic syndrome is accompanied by edematous-ascitic syndrome. Sharp pain in the right side, pathological breathing, hyperbilirubinemia are signs of the terminal stage of pathology. Patients experience convulsions, pupils dilate, blood pressure drops, reflexes fade, and breathing stops.
Clinical significance of the Chiari network
The clinical significance of the Chiari network is primarily determined by its high connection with the patent foramen ovale. In the studies conducted, 82% with a patent foramen ovale were additionally found to have the Eustachian valve or Chiari network.
The Chiari network and Eustachian valve may prevent the closure of a patent foramen ovale. They predispose to the formation of atrial septal aneurysm and paradoxical embolism by directing blood flow from the inferior vena cava to the interatrial septum (AS). There is also an association between the presence of a Chiari network and migraine with aura in patients with patent foramen ovale (PFO).
Cases of infective endocarditis involving the Chiari network have been described. Also, the Chiari network can look like a tumor formation, and thereby lead to a false diagnosis.
Rice. 3. A thread-like formation is visualized in the right atrium - the Chiari network
If we consider the Chiari network from the perspective of thromboembolic complications, then the opinion may be twofold. On the one hand, it can act as a thromboembolic trap, protecting the patient from fatal pulmonary embolism (PE). On the other hand, the Chiari network can promote the formation of blood clots in situ.
The assumption that the Chiari network may impede blood flow has not been convincingly confirmed.
Cases of intraoperative complications caused by difficulty in passing catheters into the right chambers of the heart or into the coronary sinus due to the presence of this atrial formation have been described.
Tags: intracardiac formations, right atrium, Chiari network, Chiari network, Chiari network
Diagnostics of the Chiari network
Often the Chiari network is diagnosed together with:
- open foramen ovale (OOF) - 83% of cases
- aneurysm of the interatrial septum (ASA) – 21%
- Eustachian valve – 79% of cases
To visualize the Chiari network during transthoracic echocardiography, positions are used in which the right atrium is usually examined. To assess the site of attachment of the Chiari network, a polypositional study is necessary. Such research from different points is justified because possible sites of attachment of the Chiari network are not traced in the same scanning plane.
Identification of thin, linear, mobile structures in the right atrium, which are characterized by whip-like movements and are attached to the Eustachian valve, suggests the presence of a Chiari network.
Rice. 2. Macropreparation. Chiari network.
Arnold Chiari malformation: symptoms
There are 4 most common symptoms of Chiari malformation:
- a pressing headache in the back of the head, which intensifies with physical activity and coughing, often with pain in the neck;
- hoarseness and difficulty swallowing;
- weakness and decreased sensitivity in the limbs;
- impaired coordination and balance.
This condition may remain asymptomatic for a long time. It can appear in adolescence during the period of active growth or in adults. In this case, there is a whole list of symptoms that may indicate this anomaly:
- headaches usually begin in the occipital region;
- dizziness;
- pain in the neck;
- numbness in hands
- “goosebumps” in the fingers;
- waking up in the middle of the night due to numbness in the arm;
- unsteadiness when walking;
- feeling of lack of air. Occurs due to prolonged compression of the brain stem;
- pressure behind the sternum;
- constipation
Symptoms of Chiari malformation may vary between patients and do not necessarily correspond to the degree of herniation of the cerebellar tonsils. Some patients with significant levels of tonsil prolapse do not have any symptoms. In turn, patients with a small herniation may experience severe symptoms. When symptoms do exist, they are often vague, vague, and nonspecific, and as a result, a correct diagnosis of Arnold Chiari malformation may be delayed for a long time. The appearance of symptoms is a consequence of impaired cerebrospinal fluid circulation and compression of nerve structures. In some cases, damage to the head or neck as a result of trauma can be the onset of the disease.
Diagnosis of Chiari Malformation
Arnold Chiari syndrome may have symptoms similar to other diseases. This leads to misdiagnosis and delays proper treatment. Diagnoses that are often confused with Chiari malformation:
- cervical osteochondrosis;
- vertebrobasilar insufficiency;
- fibromyalgia;
- chronic fatigue syndrome;
- migraine;
- multiple sclerosis;
- mental disorder;
- depression;
- trigeminal neuralgia.
Arnold Chiari syndrome
Some patients wait years to be properly diagnosed with Arnold Chiari syndrome because there is no specific pathognomonic criterion to confirm Chiari malformation other than imaging. Typically, the diagnosis is established based on a comprehensive assessment of the patient’s complaints, objective and neurological examination data, as well as MRI signs of pathology:
- herniation of tonsils,
- bone deformity,
- violation of liquor circulation,
- hydrocephalus,
- cyst in the spinal cord.
- The main methods for diagnosing the disease “Arnold Chiari Syndrome” are:
Clinical significance
Isolated network is less common than in combination with communications between the atria. If it is detected, then this gives grounds to look for LLC and AMSA (atrial septal aneurysm) by polypositional study, using standard and intermediate positions.
Clinically, due to the pathology, thromboembolic complications (thrombus in situ), infective endocarditis, difficulties with differential diagnosis due to various intra-atrial formations (tumors, blood clots, cysts) are possible, and difficulties are possible when conducting endovascular approaches to the heart.
Echocardiography
Echocardiography shows the Chiari network (CN):
- in panel A, the tricuspid valve (TV) is displaced in the apical 4-chamber view;
- in panel B, it is in the inflow of the right ventricle;
- Panel C shows laminar flow through an atrial septal defect.
Lamina reticulum fibers
In the video in this article you can see the work of the heart with the presence of the Chiari network.
Possible complications
Often, people suffering from Arnold Chiari pathology experience progression of the disease, as a result of which quite serious complications develop. The most common consequences include:
- Hydrocephalus – a fairly large amount of excess fluid accumulates in the brain;
- Paralysis – can be caused by severe compression of the spinal cord. It should be noted that it may remain even after surgery and subsequent rehabilitation;
- Syringomyelia - a cyst or cavity forms inside the spine, which gradually fills with fluid and often disrupts the normal functioning of the spinal cord;
- Heart disease - diagnosed only in isolated cases;
- Respiratory dysfunction;
- Congestive pneumonia;
- Reduced level of intelligence.
Treatment in adults
The main treatment method is surgery. Conservative therapy can only be considered as an additional method. But in most cases, the disease is accompanied by significant neurological disorders, including the development of paresis and other life-threatening complications. In this case, surgical treatment cannot be delayed.
Most often, specialists use craniovertebral decompression. The operation involves removing a bone fragment with widening of the foramen magnum. Specialists also eliminate signs of compression of neurological structures, remove the cerebellar tonsils and parts of the first two cervical vertebrae. To restore the normal flow of cerebrospinal fluid, artificial materials and transplants are used, which are sutured into the area of the dura mater as patches.
Carrying out bypass operations
In neurosurgery, shunt systems are actively used to eliminate hydrocephalus. The purpose of this surgical intervention is to restore the outflow of cerebrospinal fluid. Shunts have one-way valves. In the future, it is possible to replace these systems or revise them during repeated neurosurgical interventions.
The outflow of cerebrospinal fluid is achieved by draining the ventricles of the brain. The shunt system can be connected to the right atrium or the abdominal cavity. It is possible to use modern endoscopic methods of surgical treatment. They are characterized by minimally invasiveness and a short rehabilitation period.
With a highly qualified neurosurgeon, operations take place without any complications. The risk of infection increases if the basic rules of infection safety are not followed, the shunt is disconnected, or a sharp decrease in intracranial pressure. By using special shunt systems, such adverse consequences can be avoided.
Manifestations
Based on the frequency of occurrence, the following symptoms are distinguished:
- headaches – in a third of patients;
- pain in the limbs – 11%;
- weakness in the arms and legs (in one or two limbs) – more than half of the patients;
- feeling of numbness in the limb – half of the patients;
- decrease or loss of temperature and pain sensitivity – 40%;
- unsteadiness of gait – 40%;
- involuntary eye vibrations – a third of patients;
- double vision – 13%;
- swallowing disorders – 8%;
- vomiting – 5%;
- pronunciation disorders – 4%;
- dizziness, deafness, numbness in the facial area - in 3% of patients;
- syncope (fainting) – 2%.
Pain in the head and neck area is a common symptom of pathology.
Chiari disease of the second degree (diagnosed in children) combines dislocation of the cerebellum, brainstem and fourth ventricle. An integral symptom is the presence of a meningomyelocele in the lumbar region (herniation of the spinal canal with protrusion of the substance of the spinal cord). Neurological symptoms develop against the background of an abnormal structure of the occipital bone and cervical spine. In all cases, hydrocephalus is present, often a narrowing of the cerebral aqueduct. Neurological signs appear from birth.
Surgery for meningomyelocele is performed in the first days after birth. Subsequent surgical expansion of the posterior cranial fossa allows achieving good results. Many patients require bypass surgery, especially with stenosis of the aqueduct of Sylvius. With an anomaly of the third degree, a cranial hernia in the lower occiput or in the upper cervical region is combined with developmental disorders of the brain stem, cranial base and upper vertebrae of the neck. The formation involves the cerebellum and in 50% of cases the occipital lobe.
This pathology is very rare, has an unfavorable prognosis and sharply reduces life expectancy even after surgery. It is impossible to say exactly how long a person will live after timely intervention, but most likely not for long, as this pathology is considered incompatible with life. The fourth degree of the disease is an isolated hypoplasia of the cerebellum and today does not belong to the Arnold-Chiari symptom complex.
Clinical manifestations in the first type progress slowly over several years and are accompanied by the involvement of the upper cervical spinal cord and distal medulla oblongata with disruption of the cerebellum and caudal group of cranial nerves. Thus, in individuals with Arnold-Chiari malformation, three neurological syndromes are distinguished:
- Bulbar syndrome is accompanied by dysfunction of the trigeminal, facial, vestibulocochlear, hypoglossal and vagal nerves. In this case, disturbances in swallowing and speech, downward spontaneous nystagmus, dizziness, respiratory distress, paresis of the soft palate on one side, hoarseness, ataxia, incoordination of movements, and incomplete paralysis of the lower extremities are observed.
- Syringomyelitic syndrome is manifested by atrophy of the tongue muscles, difficulty swallowing, lack of sensitivity in the facial area, hoarseness of the voice, nystagmus, weakness in the arms and legs, spastic increase in muscle tone, etc.
- Pyramidal syndrome is characterized by slight spastic paresis of all extremities with hypotonicity of the arms and legs. Tendon reflexes in the limbs increase, abdominal reflexes are not evoked or are decreased.
The operation is performed for severe forms of the disorder
Pain in the back of the head and neck may intensify when coughing or sneezing. Temperature and pain sensitivity in the hands, as well as muscle strength, decreases. Fainting and dizziness often occur, and patients' vision deteriorates. In advanced cases, apnea (short-term cessation of breathing), rapid uncontrolled eye movements, and deterioration of the pharyngeal reflex appear.
An interesting clinical sign in such people is the provocation of symptoms (syncope, paresthesia, pain, etc.) by straining, laughing, coughing, and Valsalva maneuver (forced exhalation with the nose and mouth closed). With an increase in focal symptoms (stem, cerebellar, spinal) and hydrocephalus, the question arises of surgical expansion of the posterior cranial fossa (suboccipital decompression).
Modern echocardiography, heart murmurs, pregnant women and diving
Ultrasound scanner WS80
An ideal tool for prenatal research.
Unique image quality and a full range of diagnostic programs for an expert assessment of a woman’s health.
Experience in the diagnostic and treatment department allows us to divide patients who come for echocardiography into certain groups, depending on the reasons for their visit.
The first category will be pregnant women
, since an echocardiographic examination is considered mandatory and is included in the examination plan.
The second, numerous category will consist of young people
with cardialgia.
The third group will consist of patients with chronic heart pathology
who need dynamic monitoring (congenital and acquired defects, etc.) or clarification of the diagnosis.
The fourth group will consist of patients with new complaints of pain in the heart area
, shortness of breath, manifestations of heart failure.
This group of patients is the most serious, because among them one can find “acute” pathology (aneurysm of the thoracic ascending aorta, thromboembolism in the pulmonary artery system, development of aneurysm of the left ventricle, etc.). The fifth group will consist of patients with a heart murmur
. We will try to explain the capabilities of echocardiography in the diagnosis of heart pathology and differential diagnosis. To do this, we will try to analyze the above groups of patients.
Echocardiography during pregnancy
During pregnancy, a healthy woman can experience minor changes in the size of the heart cavities and changes in hemodynamics compared to the baseline. Systolic pressure in the pulmonary artery can increase to 40 mmHg. Art. The diameter of the aortic root, left atrium and left ventricle may increase by 2 - 3 mm. The heart rate increases by 25 - 30%, and already in the first trimester of pregnancy the minute volume of blood flow and stroke volume increase. Blood pressure does not change. The degree of valve regurgitation increases (on the tricuspid valve and pulmonary artery valve to degree 3, on the mitral valve to degree 2). In rare cases, a reaction of the pericardial layers can be observed - the presence of a small amount of fluid in the pericardium. The fluid disappears 1 to 3 months after birth in the absence of treatment.
One of the features in pregnant women is dynamic stenosis of the inferior vena cava. This phenomenon may be accompanied by an auscultatory picture - noise during auscultation and syncope that occurs when the body position in space changes. In some cases, during pregnancy, the oval window opens and a slight shunt of blood from left to right is noted. All of the above changes usually disappear after childbirth. Dynamics are best carried out 1 - 3 months after birth.
Causes of cardialgia - pain simulating pain in the heart
The most common cause of cardialgia in young people is overwork, stress and hypokalemia (potassium deficiency). Sometimes in this category of patients one can observe a slight prolapse of the anterior leaflet of the mitral valve into the cavity of the left atrium, which is a variant of the hole for young people and children (Fig. 1). This prolapse should not be confused with pathological prolapse when there are organic changes in the valves (for example, with myxomatous degeneration - Fig. 2).
Rice. 1.
Minor prolapse of the anterior leaflet of the mitral valve (normal variant).
Rice. 2.
Myxomatous degeneration of the mitral valve leaflets.
A differential diagnosis can be made at an appointment with a cardiologist or therapist. As a rule, after a conversation with the patient and auscultation, the doctor prescribes an ECG and EchoCG examination. If an electrolyte imbalance is suspected, a biochemical blood test is recommended.
In patients with chronic heart disease
, for example, rheumatic heart disease, congenital heart disease, prosthetic heart valve, etc. Echocardiography is performed once a year or once every 2 years. Echocardiography allows you to assess the condition and structure of the heart valves, the degree of defect, the condition of the prosthesis, the systolic function of the ventricles of the heart, the condition of the aortic walls, the degree of pulmonary hypertension, the condition of the pleural cavities and pericardium, etc. (Fig. 3 and 4). In some cases, patients come to clarify the degree or nature of the defect.
Rice. 3.
Rheumatic heart disease - mitral valve stenosis.
Rice. 4.
Congenital heart disease - atrial septal defect. Dilation of the right chambers of the heart, shunting blood through the defect in color Doppler mode.
Patients with new complaints of pain in the heart area and clinical manifestations of heart failure
are the most serious group of those examined and often require a more detailed examination (for example, coronary angiography) or consultation with a cardiac surgeon or vascular surgeon (Fig. 5).
Rice. 5.
Aneurysm of the ascending aorta.
The causes of heart failure are varied. The echocardiography technique allows for closer verification of the diagnosis, and in some cases, an accurate diagnosis.
Heart murmurs
One of the most common reasons for referral to echocardiography is the presence of a heart murmur.
In the “pre-echocardiographic” era, it was in some cases difficult to distinguish normal functional murmur from pathological one. Let's try to list the causes of the most common normal functional murmurs in the heart area. They are especially good for children, teenagers and thin people.
Additional chord in the cavities of the ventricles (false chord or false chord)
- a filamentous structure located in the cavity of the left or right ventricle. Located between the interventricular septum (IVS) and the wall of the heart, the head of the papillary muscle and the wall, etc. The base of the accessory chord does not thicken during systole. The number of chords may vary. Occurs in 98% of cases (Fig. 6).
Rice. 6.
A minor developmental anomaly is an additional chord in the cavity of the left ventricle (normal variant).
Additional muscle trabecula in the ventricular cavity (false trabecula)
- a muscular structure located in the cavity of the left or right ventricle. Often located parallel to the interventricular septum or transversely between the walls of the ventricle. The base of the accessory muscle trabecula thickens during systole. Occurs in 85% of cases (Fig. 7).
Rice. 7.
A minor developmental anomaly is an additional muscle trabecula in the cavity of the left ventricle and two additional chords (normal variant).
Eustachian valve of the inferior vena cava
- vestigial valve. Does not play any role in cardiac hemodynamics. Occurs in 20% of cases.
Hiari network
- rudiment, continuation of the Eustachian valve of the inferior vena cava into the coronary sinus. Occurs in 2% of cases.
Aneurysm of the interatrial septum
Atrial septal aneurysm (ASA)
- a congenital feature of the development of the interatrial septum. The membrane of the fossa oval is elongated and bulges to the side (Fig. 8). There are a number of types of atrial septal aneurysm:
- type L - bulging of the fossa ovale membrane towards the left atrium.
- type R - bulging towards the right atrium (Fig. 9).
- Type R - L - bulges to the right and then to the left.
- Type L - R - bulging to the left and then to the right - occurs in 5% of cases.
Rice. 8.
Aneurysm of the interatrial septum.
Rice. 9.
Aneurysm of the interatrial septum - type R.
If the aneurysm is very large and protrudes significantly into the atrium cavity, it can be regarded as a congenital defect of the interatrial septum (extremely rare). If there is an atrial septal defect in the area of the atrial septal aneurysm, the situation is regarded as a congenital heart defect.
Aneurysm of the membranous part of the interventricular septum
- rare (0.5 - 1% of cases).
Accessory heads of papillary muscles
- their number can be different and, according to anatomists, can reach 16, the sizes of the heads are also different. The more papillary muscles in the ventricular cavity, the more chordae extend from them.
Non-closure of the oval window
- a variant of the development of the membrane of the fossa oval, occurs in 25% of people. The valve of the fossa ovale membrane covers the oval window. There is no shunting of blood, but it can occur in a number of situations (for example, with a sharp increase in pressure in the cavity of the left or right atrium).
Patent foramen ovale
- occurs less frequently (1 - 2% of people).
Currently, in pediatric practice
there is an overdiagnosis of an open oval window. In this case, blood shunting occurs from left to right, is intermittent, and the volume of the shunt is small. There is no pulmonary hypertension or dilatation of the right chambers. Color Doppler allows you to clarify the presence or absence of an open oval window. These patients require observation once every 2-3 years.
Contraindications for diving
The only contraindication for people with a patent oval window is diving (scuba diving). In any case, whether you are going to Egypt or Thailand and want to plunge into the enchanting world of the seabed, or spend time in the city, do not be lazy to go to a cardiologist and undergo an echocardiographic examination. This will avoid tragic consequences.
Ultrasound scanner WS80
An ideal tool for prenatal research.
Unique image quality and a full range of diagnostic programs for an expert assessment of a woman’s health.
Symptoms
Chiari malformation type I is the most common form of the syndrome, the clinical signs of which are conventionally combined into five syndromes:
- Hypertension syndrome is manifested by cephalgia, a rise in blood pressure in the morning, tension and hypertonicity of the cervical muscles, discomfort and pain in the cervical spine, dyspeptic symptoms, general asthenia of the body. Newborn children experience general anxiety, vomiting in a fountain, tremor of the chin and limbs, disturbed sleep . The child constantly cries and refuses to breastfeed.
- In the presence of cerebellar disorders, patients' pronunciation changes, speech becomes scanned, and vertical nystagmus occurs. They complain of frequent dizziness, uncoordinated movements, unsteadiness of gait, trembling of hands, imbalance, disorientation in space. Patients have great difficulty performing simple purposeful actions; their movements lack clarity and coordination.
- Damage to the cranial nerves manifests itself as signs of radicular syndrome. Patients have limited mobility of the tongue and soft palate, which leads to difficulty speaking and swallowing food. Their voice changes towards nasality and hoarseness, speech becomes unclear, breathing becomes difficult. Impaired night breathing is observed in most patients. They experience hypopnea, central or obstructive apnea, with the progression of which acute respiratory failure develops. Persons with the syndrome have difficulty hearing and seeing, they have double vision and noise in their ears. On the part of the visual organs, patients note the presence of photophobia and pain when moving the eyeballs. Ophthalmologists often detect anisocoria, accommodation spasm, or scotomas. One of the main symptoms of the syndrome is hypoesthesia - decreased sensitivity of the skin of the face and limbs. Such pathological changes are associated with a muted response of skin receptors to external stimuli: heat or cold, injections, blows. In severe cases, the nerve endings generally cease to perceive various exogenous influences.
- Syringomyelic syndrome is a complex symptom complex manifested by paresthesia or numbness of the extremities; changes in muscle tone and hypotrophy, leading to myasthenic disorders; damage to peripheral nerves, manifested by pain in the limbs; dysfunction of the pelvic organs in the form of difficulty defecating or spontaneous urination; Possible arthropathy - damage to the joints.
- In patients with pyramidal insufficiency, strength in the lower extremities and the ability to perform fine movements are reduced, the range of movements is limited, and muscle tone increases - the so-called spasticity, for example, a spastic gait. An increase in tendon reflexes is combined with a simultaneous decrease in skin reflexes - abdominal ones. Pathological reflexes may appear. Patients suffer from fine motor skills.
Any careless movement intensifies the symptoms of the pathology, making them more pronounced and vivid. Changes in head position are a common cause of loss of consciousness
Symptoms
The main signs of this syndrome include:
- Pain is almost always felt in the cervical-occipital region, which usually intensifies with sneezing and coughing;
- Headaches that occur because intracranial pressure becomes higher or the neck muscles become tense;
- Frequent attacks of dizziness and loss of consciousness, especially when turning the head or sudden movements;
- A sharp deterioration in vision;
- Deterioration of general condition;
- Significant reduction in temperature and pain sensitivity in the hands;
- Feeling of severe weakness in the muscles of the upper limbs;
- Spasticity in fingers;
- Regularly recurring attacks of apnea (short pauses in breathing);
- Noticeable weakening of the swallowing reflex;
- Sudden movement of the pupils of the eyes, which is not controlled by the brain;
- Difficulty or involuntary urination;
- Nystagmus is an abnormal twitching of the eyeballs;
- The occurrence of extraneous noise in the ears, especially when turning or tilting the head low;
- Manifestation of tremor of the upper and lower extremities;
- Impaired coordination of movements;
- Clearly expressed impairment of fine motor skills;
- Decreased body sensitivity;
- The muscles of some parts of the body are much weaker, so it can be painful to lift even light objects;
- A condition that can cause a heart attack of the brain or spinal cord.
Symptoms of the disease
Symptoms of the disease depend on the type of Arnold-Chiari malformation. A neurologist or neurosurgeon can qualify the pathology. In the clinical practice of neurosurgeons, grade 1 Arnold-Chiari malformation is often encountered. The disease develops after the end of puberty or in adult patients.
The main signs of pathology in adults:
- headache in the neck and back of the head, which tends to get worse with muscle tension, coughing and sneezing;
- vomiting that does not depend on food intake;
- increased muscle tone;
- cerebellar ataxia;
- tendency to nystagmus and speech disorders;
- decreased visual and hearing acuity.
Other symptoms may also appear, including short-term loss of consciousness. Patients with this disease complain of dizziness whenever they turn their head. In some cases, fainting may even occur. A common symptom is atrophic changes in the tongue and larynx. They are accompanied by breathing problems and chronic hoarseness. Similar consequences arise in the absence of effective medical care for a long time.
Arnold-Chiari malformation type 2 causes noisy breathing, combined with laryngeal paresis and reflux of food into the nose. An accurate diagnosis can be made based on examination and diagnostic data. A neurological examination in combination with magnetic resonance imaging of the brain and spine can reveal characteristic abnormalities. Once the diagnosis is confirmed, appropriate treatment should be started as soon as possible.
Magnetic resonance imaging is the most widely used diagnostic method for this disease. During the study, it is possible to detect dislocation of the tonsils and obtain information about the composition of brain tissue. To study the flow of cerebrospinal fluid, phase-contrast MRI is necessary.
Arnold-Chiari malformation grade 1
The cerebellar tonsils are located below the foramen magnum. Arnold-Chiari malformation grade 1 is more common in adults. As the disease progresses, cerebrospinal fluid begins to accumulate in the central canal of the spinal cord. When the disease is combined with syringomyelia, sensitivity is impaired, signs of numbness and atrophic processes in the muscles appear. Peritoneal reflexes may disappear.
Arnold-Chiari malformation grade 2
With this disease, not only the tonsils, but also the cerebellum itself, the fourth ventricle, and the medulla oblongata begin to emerge through the foramen magnum. The disease is associated with congenital spina bifida. The pathology is accompanied by myelomeningocele and spina bifida.
Arnold-Chiari malformation grades 3 and 4
Arnold-Chiari malformation of 3-4 degrees is accompanied by the transition of descended brain formations into meningocele of the back of the head and neck. With stage 4 disease, hypoplastic processes in the cerebellum are often combined with signs of hydrocephalus.
The development of combined pathology is possible. The disease can occur against the background of dysplastic processes in the nervous system, including disturbances in the functionality of the corpus callosum and underdevelopment of subcortical structures.
Diagnosis of the disease
To make the most accurate diagnosis, determine the stage of development of the disease, and also make a further prognosis, you need to conduct a thorough examination and several neurological examinations:
- Echoencephalography of the brain;
- Electroencephalography;
- Rheoencephalography.
However, even their results do not make it possible to make an accurate diagnosis, because with their help they can only determine signs of increased intracranial pressure.
X-ray of the skull is required to determine the level of bone development disorders that often accompany Arnold Chiari syndrome. CT, as well as MSCT of the brain, despite fairly good visualization of the bone structures of the craniovertebral junction, do not allow neurologists to fully determine the state of soft formations in the posterior fossa of the skull.
In this regard, MRI (magnetic resonance imaging) has recently been most often used - the only simple and reliable way to diagnose this anomaly in the development of the brain and spinal cord. Since it requires complete immobility of a person, for examination young children are put into a state of so-called medicated sleep.
In addition to MRI of the brain, neurologists can provide a referral for MRI of the thoracic and cervical spine. The indication for this is the suspicion of parallel development of syringomyelic cysts or meningoceles. Another important advantage of this technique is that it helps to detect even mild disorders in the development of the central and peripheral nervous system that may accompany Chiari malformation.
Diagnostics
To visualize the Chiari network, echocardiography is used. In this case, positions are used in which the PP is simultaneously examined: apical 4CP, modified parasternal biccaval position and short axis at the level of AOC from the left parasternal approach, but this can only be performed by professional diagnosticians.
Subcostal positions are also used: 4KP, short axis at the level of the Aoc and long axis of the vena cava from below. To assess the insertion site of the Chiari network, it is necessary to perform a polypositional study and include intermediate attachment positions on the eustachian and coronary sinus valve.
In other possible locations in the same plane, the network may not be visualized. Then a 3D EchoCG study is used. The best way to assess the mouth of the coronary sinus is with a sensor from the esophagus, or more precisely, from its middle sections.
Snapshot of the Chiari network