Large blood vessel in the hand
| Cephalic vein | |
| Superficial veins of the upper limb | |
| The most common variations of the veins of the forearm. | |
| Details | |
| Drains from | Dorsal venous network of the hand |
| Drains into | Axillary vein and median ulnar vein |
| Artery | Deltoid branch of the thoracoacromial artery |
| Identifiers | |
| Latin | Vein head |
| TA98 | A12.3.08.015 |
| TA2 | 4964 |
| F.M.A. | 13324 |
| Anatomical terminology [edit in Wikidata] | |
In human anatomy, the cephalic vein
[1] are superficial veins in the arm.
It communicates with the basilic vein through the median ulnar vein at the elbow joint and is located in the superficial fascia along the anterolateral surface of the biceps muscle.
Near the shoulder, the cephalic vein runs between the deltoid and pectoralis major muscles (deltopectoral groove) and through the clavipectoral triangle, where it joins the axillary vein.
Clinical significance[edit]
The cephalic vein is often visible through the skin, and its location in the deltopectoral sulcus is quite stable, making this site a good candidate for venous access. Permanent pacemaker leads are often placed in the cephalic vein in the deltopectoral groove. The vein can be used for intravenous access as a large bore cannula can be easily inserted. [1] However, cannulating the vein as close as possible to the radial nerve rather than the cephalic vein can sometimes result in nerve damage. [1]
Intensive care nurse: venous catheterization
One of the main responsibilities of an intensive care nurse is organizing venous access for a patient, or, more simply, catheterizing a vein. A catheter is placed in different cases: to take blood for analysis (sometimes tests are taken several times a day, and pricking again each time is painful and traumatic for the patient) or to administer drugs and nutritional solutions to the patient. Placing a catheter is almost no different from a regular injection - you just need the vein to be straight in a certain area.
Where you can inject and where you can’t
To select a vein, you need to roughly estimate why the catheter is being placed in the first place. For emergency patients with severe injuries, bleeding, or those who are being prepared for abdominal surgery, a large-diameter catheter is placed, and a large vein is selected accordingly. For a grandmother of a very elegant age, whose diagnosis is not so serious, a smaller catheter is selected - the veins at this age are most often no longer the same.
How to choose the injection site? Nurses start with the distal veins, i.e. those that are “on the periphery”: the veins of the hand, forearm. The principle of ascending from the hand above also works (bad veins on the hand - move to the forearm).
The veins on the elbow are clearly visible, but this place is not very suitable for catheterization. The person bends and straightens the arm, sometimes unintentionally, and the catheter can become kinked or broken. Although, if you don’t need to insert a catheter, but only one or two injections are expected, the elbow bend is what you need. The vein on it is thick enough and will withstand all this.
Elsewhere, the vein may not be visible, but with a tourniquet applied, it can be easily felt with the fingers (palpated). In this case, an experienced nurse will be able to give an injection without even seeing the vein. In some patients, the median ulnar vein is not visible, but you can feel another one, which is a little closer to the outside of the arm, the lateral saphenous vein (it is also not visible with the eyes). I have had cases when I fell into such veins almost blindly - my veins also have this feature, so I am well aware of it.
How to properly place an IV: procedure algorithm
In order to administer an intravenous infusion, appropriate knowledge, experience and strict adherence to technique are required. Correct placement of a drip is not only about inserting a needle without consequences for the patient, but also about choosing a system, infusion rate, etc.
Tools and accessories
To carry out the infusion, it is necessary to prepare the medications prescribed by the doctor (check the expiration date, volume and other important indicators), as well as instruments and consumables:
- Dropper stand. It is a portable stand with hooks onto which containers with solutions are placed. Its height is 1.5-2 m, which provides sufficient pressure for insertion.
- Infusion system. Droppers differ in the diameter of needles, tubes and the speed of infusion of drugs. It is very important to decide on the size of the needle, which is inversely proportional to the number: twenty-second is the thinnest, fourteen is the thickest. It depends on the anatomical features of the patient and the characteristics of the drug.
- Related accessories. In addition to a tripod and a system for placing an IV, you will need a tourniquet (it helps to find the vein), a patch to fix the needle and cotton wool.
In addition to the prescribed medications, you need to prepare an antiseptic liquid. Most often, alcohol is used; if a person has allergies, they take alcohol-free solutions (for example, Chlorhexidine).
Preparation for the procedure
Before manipulations, be sure to wash your hands and wipe them with an antiseptic. Failure to comply with hygiene rules can lead to infection and sepsis, even if the health worker has perfect infusion technique.
- Connect the system to the container or package with the drug. To do this, you need to wipe the needle with alcohol and pierce the cork - this is not difficult, since they are made of soft rubber or other materials.
- Hang the containers on the racks and secure them well. Be sure to check that there is no air in the system - fill the tubes and drip chamber about a third with liquid. Small bubbles are usually not dangerous - they will stick to the walls of the container and will not enter the bloodstream.
If sterility is violated at one of the stages, infusion is strictly prohibited. This can lead to blood poisoning and other dangerous consequences.
Placement of the IV
Before the procedure, it is necessary to familiarize the patient with the features of its implementation. Each drug has a special effect on the body, and some sensations may frighten a person. It is important to distinguish the side effects of drugs from the alarming symptoms that develop when infusions are performed incorrectly. Pain, dizziness, nausea, weakness and other discomfort should be reported to a healthcare professional immediately. The procedure algorithm is as follows:
- the patient takes a comfortable position - it is best to do the IV while lying down, but it is also possible in a semi-sitting or sitting position;
- the arm in the biceps area is tied with a tourniquet, the needle insertion site is thoroughly disinfected;
- the needle is inserted into the darkest, well-filled vein parallel to the surface of the arm at an angle of 35-45 degrees;
- after blood appears in the catheter, it is positioned as parallel to the limb as possible and fixed with an adhesive tape;
- connect the system tube to the catheter, make sure the connection is tight, and additionally secure it with a bandage;
- The rate of supply of the solution is adjusted using a dial with a wheel - sometimes the number of drops is marked on it to make counting easier.
During the procedure, it is necessary to monitor the patient and the needle insertion site. If the fluid flows too quickly, the person may become dizzy. In such a situation, it is better to simply reduce the infusion rate by turning the wheel in the desired direction.
After completing the procedure, it is necessary to close the system, carefully remove it, apply cotton wool soaked in alcohol to the injection site and press well. You need to keep it for at least 10-15 minutes, and preferably 20-25 minutes. During this time, a blood clot will form, which will clog the wound. If you remove the cotton too quickly, drops of blood will get under the skin, resulting in a bruise or bruise. Do not rub or touch the injection site, as this can also lead to the accumulation of blood clots.
Course of the disease
The course of the disease is divided into two stages: acute (lasts about three weeks; at the initial stage, symptoms appear during physical activity) and chronic (symptoms last for more than two months).
The acute phase is characterized by increasing swelling of the arm, pain, and a feeling of fullness. The patient's ability to work decreases. Gradually, tense saphenous veins develop, which take on the function of outflow of venous blood and contribute to the subsidence of the process.
The chronic phase is the consequences of thrombosis. With inadequate treatment, occlusion of the subclavian vein persists and chronic Paget-Schroetter syndrome develops. It is characterized by the development of a powerful collateral network of saphenous veins around the shoulder joint. Patients are concerned about the increase in volume of the sore arm, sometimes there is pain and increased fatigue.
How can you tell if the medicine is going past the veins?
To prevent infiltration and extravasation, the patient must be closely monitored during the procedure. List of warning signs:
- unnaturally shiny, dense, stretched skin at the site of needle insertion;
- tension and the appearance of swelling (rapidly growing swelling is especially dangerous);
- change in the shade and temperature of the hand - redness, blueness, too cold skin;
- self-slowing or stopping the flow of medication;
- continuation of the infusion after applying a tourniquet to the vein;
- leakage of solution around the injection site;
- burning or discomfort in the area where the needle is located.
If such symptoms occur, stop the infusion immediately and remove the needle. The injection site must be carefully examined, and if a large amount of solution is injected past a vein (especially if it is viscous or caustic), you must immediately consult a doctor. To eliminate the consequences in such cases, the introduction of an antidote is required.
If the amount of the drug that gets into the tissue is small, you need to monitor the affected area for 2-3 days. At the first manifestations of necrosis, immediately contact a medical facility.
If a vein is damaged, it is necessary to press it for a few minutes, and then apply a dry sterile bandage; if a hematoma appears, apply a compress. If the patient's condition has not worsened, the IV can be reinserted into another vein.
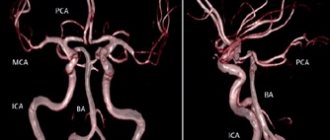
Headache and venous congestion
Venous stagnation (or disturbances of venous outflow from the cranial cavity) is a syndrome that often occurs with headaches of various types. Unfortunately, it is a common situation when venous outflow disorders are not taken into account in the treatment of tension headaches and migraines; as a result, patients suffer for years.
Even though venous outflow disorders are often described during head studies (MRI, vascular ultrasound), they are practically not taken into account in combination with other signs and complaints of the patient.
Manifestations of venous stagnation
Venous pressure inside the cranial cavity normally changes constantly - it increases with straining, coughing, sneezing, and decreases with rest. If venous outflow becomes difficult, characteristic complaints may appear:
- Heaviness in the head and pain in the morning.
- Swelling of the face (especially the eyelids) after sleep.
- Bursting headache.
Disturbances of venous outflow and nature of pain
Disturbances in venous outflow can change the nature of pain in patients with tension-type headaches. For example, pressing pain in the temples is accompanied by heaviness in the head after sleep.
There are even situations when disturbances in venous outflow are the main and only cause of headaches, and tension headaches come later.
The situation is no easier for migraine patients. In addition to the migraine itself, many also experience tension in the neck muscles and impaired venous outflow. In such patients, headaches almost never stop.
In practice, it turns out that an incorrect diagnosis (without taking into account venous outflow disorders) leads to long-term and ineffective treatment of headaches.
Difficulties in diagnosis
How can a doctor suspect the presence of a “venous factor”? After all, as we see, complaints with venous stagnation are not so specific. Only on the basis of symptoms such as swelling of the face and heaviness in the head in the morning, a correct diagnosis cannot be made.
The patient should be asked about changes in pain patterns and headache frequency. Since the tone of the veins can change with changes in atmospheric pressure, weather or cycle phase in women, all this must be taken into account.
Venous congestion can be confirmed using the following methods:
– Consultation with an ophthalmologist - dilated veins will be visible in the fundus. – Ultrasound examination of blood vessels - a decrease in the speed of blood flow through the veins will be noted. – Magnetic resonance imaging in phlebographic mode - dilated venous sinuses and veins will be noticeable.
However, the conclusion “impaired venous outflow” in itself does not carry much value - what is more important is the full clinical picture with the specifics of your complaints.
How to treat?
With regard to drugs for disrupting venous outflow from the cranial cavity, the situation is complex. There are currently no effective drugs with proven action against veins inside the skull. In practice, vascular drugs (for example, Cavinton) and metabolic drugs (Mexidol) are often prescribed, which may cause some improvement (although their effect has not been proven). Sometimes venotonics (for example, Detralex) are prescribed with a positive effect
Among other methods of treating headaches with impaired venous outflow, the methods of manual therapy, massage, and physiotherapy (if there is tension in the neck muscles or the effect of osteochondrosis on the blood vessels) have proven themselves to work well in practice.
Timely detection of venous outflow disorders and consultation with a neurologist can protect against progression and chronicity of pain.
Be healthy!
Maria Meshcherina
Photo istockphoto.com
Risk factors
Many factors can increase your risk of developing DVT, which include:
- Age. At age 60, the risk of DVT increases, although it can happen at any age.
- Sitting for long periods of time, such as while driving or flying. When your legs remain motionless for several hours, your calf muscles do not contract. Muscle contractions promote blood circulation.
- Prolonged bed rest, such as during a long hospital stay or paralysis. Blood clots can form in the calves if the calf muscles are not used for a long time.
- Trauma or surgery. Injury to the veins or surgery may increase the risk of blood clots.
- Pregnancy. Pregnancy increases pressure in the veins of the pelvis and legs. Women with an inherited bleeding disorder are at particular risk. The risk of blood clots from pregnancy can last up to six weeks after the baby is born.
- Birth control pills (oral contraceptives) or hormone replacement therapy. Both factors can increase the blood's ability to clot.
- Exposure to drugs or chemicals. Certain drugs can cause blood clots. Consult your physician before use.
- Overweight or obese. Excess weight increases pressure in the veins of the pelvis and legs.
- Smoking. Smoking affects clotting and circulation, which may increase the risk of DVT.
- Cancer. Some forms of cancer increase levels of substances in the blood that cause blood clotting. Some forms of cancer treatment also increase the risk of blood clots.
- Heart failure. Increases the risk of developing deep vein thrombosis and pulmonary embolism. Because people with heart failure have limited heart and lung function, symptoms caused by even a small pulmonary embolism are more noticeable.
- Inflammatory bowel diseases. Bowel diseases such as Crohn's disease or ulcerative colitis increase the risk of DVT.
- Personal or family history of DVT or PE. If you or someone in your family has had one or both of these, you may be at greater risk of developing DVT.
- Genetics. Some people inherit genetic risk factors or disorders, such as factor V Leiden, that make their blood clot more easily. The hereditary disease itself may not cause blood clots unless it is combined with one or more other risk factors.
- Risk factor unknown. Sometimes a blood clot in a vein can occur without an obvious underlying risk factor. This is called unprovoked VTE.