Accelerated metabolism and increased oxygen demands cause children's hearts to beat faster. Heart rate norms are individual for each age. If for some reason this indicator exceeds the norm for no apparent reason (emotional experiences or physical exertion, overheating), tachycardia is diagnosed. At the medical center (Moscow, Otradnoye metro station, North-East Administrative District), cardiologists diagnose and treat tachycardia in children. Therapy begins with eliminating the root cause, and along the way, doctors select medications that alleviate the condition.
Causes and types
Restlessness is considered one of the causes of cardiac tachycardia in childhood. Children are constantly moving, which naturally causes an increase in heart rate and heart rate. Other factors are also possible:
- dehydration;
- heart murmurs;
- anemia;
- cardiopathy;
- thyrotoxicosis;
- Congenital heart defect.
In addition, there are two forms of the disease: sinus and paroxysmal, which also develop for certain reasons. Sinus tachycardia in children is a consequence of:
- accelerated growth;
- stress;
- disorders of the endocrine or cardiovascular systems;
- overwork.
Diagnosing the cause of the paroxysmal form is more difficult, since in this case the heart rate increases and slows down suddenly. Seizures occur at any age, including in newborns.
Fever varies:
- with the flow:
- acute (fever up to 2 weeks),
- subacute (up to 6 weeks),
- chronic (over 6 weeks).
- according to the degree of increase in the indicator:
- subfebrile (increase to +38.0 degrees)
- febrile (from +38.0 to +39.0 degrees),
- pyretic (from + 39.0 to +41.0 degrees),
- hyperpyretic (over +41.0 degrees).
- by type of temperature curve:
- constant (temperature fluctuations during the day do not exceed 1 degree).
- laxative (daily fluctuations up to 2 degrees),
- atypical (oscillations are chaotic, varied and irregular),
- debilitating (a combination of laxative and atypical fever with fluctuations during the day of more than 2-3 degrees),
- intermittent (a combination of short-term periods of increase and decrease in temperature to normal values),
- recurrent (alternating periods of temperature increase with periods of temperature normalization from 2 to 7 days).
According to the recommendation of the WHO (World Health Organization), antipyretic drugs are prescribed to children according to age:
- from birth to 2 months at a temperature of +38.0 degrees,
- children from 3 months to 24 months with a temperature of +38.5 degrees,
- children from 1 to 5 years old with a temperature of +39.0 degrees,
- children over 5 years old at + 39.5- +40.0 degrees.
Symptoms
In addition to palpitations, cardiac tachycardia in children manifests itself:
- chest pain;
- shortness of breath;
- dizziness and fainting;
- lethargy and pallor;
- nausea;
- sweating
At such moments, infants become restless and capricious, refusing to eat and sleep. It is important to consult a doctor as soon as you notice the first signs of illness. If tachycardia in children is not treated, the severe pathologies that caused it will lead to serious complications:
- arrhythmogenic shock;
- pulmonary edema;
- heart failure;
- cardiac arrest.
Journal "Child's Health" 5(8) 2007
The structure of cardiovascular pathology in childhood has undergone significant changes over the past decades. It has become obvious that the problem of heart rhythm disturbances is one of the most pressing and complex in pediatric cardiology and pediatrics in general due to a number of circumstances [16, 33]. First of all, this is due to the significant prevalence of heart rhythm disturbances in children of different ages, starting from the prenatal period, the diversity of types, evidence of a long and asymptomatic course in a number of patients, the complexity of diagnosis and treatment, the possible development of complications, as well as a serious prognosis for some types [13, 15, 16, 33, 38, 39]. In addition, cardiac arrhythmias affect not only the physical, but also the psycho-emotional development of the child. In the absence of adequate therapy, over 4–6 years, most rhythm disturbances progress, and persistent and irreversible disorders of myocardial function are formed, leading to early disability and requiring surgical intervention. At the same time, it is necessary to remember the possibility of complete restoration of normal rhythm control with timely and correct correction [27, 38].
The purpose of this work was to present possible etiopathogenetic factors, developmental mechanisms, classification approaches, clinical manifestations, and a diagnostic algorithm for tachycardia as one of the most common types of heart rhythm disturbances in children.
According to modern concepts, all tachycardias are divided into sinus, supraventricular and ventricular; paroxysmal and non-paroxysmal; reciprocal and automatic (ectopic); congenital and acquired; primary (idiopathic) and secondary, observed in pathology of the cardiovascular or other system. Let's take a closer look at each of them.
Sinus tachycardia is understood as an increase in heart rate (HR) above the age norm by 10–60%. In children, heart rate depends on age (Table 1). Sinus tachycardia is distinguished:
1) moderate (I degree) - increased heart rate 10–20% above the age norm;
2) average (II degree) - by 20–40%;
3) pronounced (III degree) - by 40–60% [21].
Sinus tachycardia can be physiological and pathological, and pathological is divided into extracardiac and cardiac [2, 21]. Physiological tachycardia occurs during physical and psycho-emotional stress, transition to orthostasis, fear, when the ambient temperature rises, after a heavy meal and liquid intake, in a stuffy room and during high-altitude hypoxia. It is characterized by a rapid (within 3–5 minutes) restoration of the rhythm after the end of the load or exposure to the listed environmental factors. Extracardiac pathological sinus tachycardia occurs with increased body temperature, acidosis, hypoglycemia, hypoxemia associated with anemia or lung damage, with pheochromocytoma and thyrotoxicosis, infectious toxicosis (neurotoxicosis), with taking or overdose of drugs: adrenaline, isadrine, aminophylline, atropine, inhalation large doses of β2-adrenergic receptor agonists (terbutaline, salbutamol, etc.). It is characterized by a moderate increase in heart rate at rest and an inadequate increase in heart rate in response to normal physical and psycho-emotional stress, and an extended restitution time. Such sinus tachycardia most often occurs in prepubertal girls and is associated with hypercatecholaminemia and hypersympathicotonia (sympathicotonic-type autonomic dysfunction syndrome) [2, 21]. Thus, physiological and pathological extracardiac tachycardia are caused by an adequate response of the heart to extracardiac stimuli (increased heart rate against the background of hyperdynamic cardiac activity) in the absence of cardiac pathology [1].
Organic (cardiac) pathological sinus tachycardia is caused by organic damage to the heart of an inflammatory (myocarditis, endocarditis, pericarditis), ischemic-necrotic (ischemic heart disease, myocardial infarction), degenerative (idiopathic cardiomyopathies) or dystrophic-sclerotic nature (myocardial dystrophy, myocardiosclerosis), as well as hyper- and hypokalemia, hypomagnesemia. Constant sinus tachycardia of varying severity is characteristic of cardiac and vascular insufficiency, congenital and acquired heart defects. Thus, this type of tachycardia is caused by impaired cardiac activity and is characterized by a persistent increase in heart rate at rest, which does not correspond to the level of physical, emotional, pathological or pharmacological stress [1, 2, 21].
Sinus tachycardia occurs as a result of neurohumoral effects on pacemaker cells and morphological changes in the sinus node (SN) itself and is caused by an increase in the automaticity of the main pacemaker - the sinoatrial node [4, 22]. It may be based on an increase in the tone of the sympathetic and/or a decrease in the tone of the parasympathetic nervous system, increased sensitivity to adrenergic receptor catecholamines, even when their content is normal [2]. As a result, functional dissociation develops in the sinus node with a short-term blockade in the sinoatrial conduction, which can lead to the development of tachycardia. There are clinical observations proving that atrial extrasystole leads to the development of sinus tachycardia [4].
Thus, the pathological basis of sinus tachycardia likely involves many factors, but suggests two main mechanisms:
1) increased automation of the control system;
2) disruption of the autonomic regulation of the SU with an increase in sympathetic tone and a decrease in parasympathetic tone.
Hemodynamically, sinus tachycardia is most often accompanied by an increase in cardiac output and coronary blood flow. However, with prolonged severe tachycardia (more than 150 beats/min) and shortened diastole, there is a discrepancy between the coronary blood flow and the increased work of the heart, resulting in the development of myocardial dystrophy [2, 21].
Clinically, children most often tolerate moderate sinus tachycardia satisfactorily, but with severe tachycardia there are complaints of palpitations, discomfort, sometimes pain in the heart, beating in the ears, especially in emotionally labile children in the prepubertal period. Physically, with functional tachycardia, changes in the color of the skin (sharp pallor or redness) and increased breathing are possible. On the part of the cardiovascular system, the first heart sound is increased; with organic damage to the heart (myocarditis, dilated cardiomyopathy, etc.), sinus tachycardia is usually accompanied by a weakening of the first sound at the apex, and an accentuation of the second sound over the pulmonary artery.
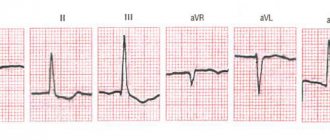
The following electrocardiographic signs are characteristic of sinus tachycardia [1, 2, 20–22]:
1) the TP interval is shortened or absent;
2) the P wave is nomotopic, pointed, increased in amplitude and decreased in duration;
3) PQ and QT intervals are shortened;
4) the ST segment may be shifted below the isoline;
5) the amplitude of the T wave is reduced and the amplitude of the U wave is increased.
Sinus tachycardia should be differentiated from paroxysmal and non-paroxysmal tachycardia, especially if the heart rate exceeds 210–220 beats/min in young children and 150–160 beats/min in school-age children. With paroxysmal tachycardia, the heart rate is usually much more frequent and more rigid (without respiratory fluctuations). Tachycardia is better detected by cardiorhythmometry, occurs in paroxysms, and is accompanied by a pronounced feeling of discomfort [2, 7, 21]. The attack may spontaneously stop after performing the Aschner maneuver, Valsalva maneuver, pressing on the carotid sinus, etc. The differences between sinus tachycardia and atrial non-paroxysmal tachycardia are as follows:
1) with sinus tachycardia, the P waves are better defined, and with atrial tachycardia they are smaller and have an unusual configuration;
2) with sinus tachycardia, the contraction frequency can change, with atrial tachycardia it remains constant;
3) when taking an ECG on a long tape, you can register a return from the ectopic rhythm to the sinus rhythm [2].
Chronic sinus tachycardia is diagnosed in the presence of sinus tachycardia at rest (according to ECG data) for 3 months or more in the absence of causes causing secondary sinus tachycardia [35]. In the occurrence and maintenance of this type of tachycardia, the decisive role is played by an increase in the level of cortical activation, which is due to the absolute or relative hyperfunction of the sympathetic department of the central nervous system. Hypercatecholaminemia, hypersensitivity of the sinus node to catecholamines, as well as hypovagotonia determine the pathogenesis, clinical picture and treatment tactics of this type of tachycardia [35]. According to O.N. Voronina [9], in children with chronic sinus tachycardia, the leading one is pronounced autonomic dysfunction with high tone of the parasympathetic division of the autonomic nervous system. Treatment of such tachycardia should include basic therapy (metabolic drugs, correctors of neurovegetative disorders - biogenic stimulants, tranquilizers with sympatholytic action, GABAergic and nootropic drugs), psychotherapy with mandatory consideration of the initial autonomic tone of children.
It is fundamental for clinical practice to distinguish between paroxysmal and non-paroxysmal tachycardia. Paroxysmal heart rhythm disturbances are one of the most pressing problems of modern cardiology. According to the American Heart Association, these disorders cause the death of 300-600 thousand people annually, that is, one death every minute. In recent decades, there have been significant changes in clinicians' understanding of the fact that arrhythmia can serve as a harbinger of sudden cardiac death. At the same time, the symptoms of arrhythmia, while not life-threatening, negatively affect the patient’s quality of life, and in some cases, arrhythmia can affect short-term and long-term prognosis [31, 39].
Paroxysmal tachycardia (PT) is a heterogeneous group of tachyarrhythmias characterized by sudden onset, high heart rate with normal sequence, short duration (from several seconds to several hours, rarely days) and sudden normalization of heart rhythm [1, 2, 19–21 ].
PTs account for 10.2–29% of all cardiac arrhythmias in children; they are detected with a frequency of 1:25,000 in the pediatric population and in 5% of sick children with congenital heart defects [2, 21]. Depending on the location of the pathological focus of excitation, supraventricular and ventricular PTs are distinguished.
Most often, supraventricular PTs are recorded in children (80–90%), mainly from the atrioventricular (AV) junction [2], their frequency is 1–3 per 1000 children [1], and supraventricular PTs are relatively often observed in girls [1]. Ventricular forms of PT in childhood are ten times less common than supraventricular ones (2%), and they are more typical for severe heart lesions, such as myocardial infarction [1, 2, 25].
Factors predisposing to the occurrence of PT attacks are pre- and perinatal pathology with early residual organic damage to the central nervous system and hypertensive-hydrocephalic syndrome, leading to cerebral dysfunction predominantly at the diencephalic-stem level, unfavorable social and family history, infectious diseases (ARVI, pneumonia and etc.), catheterization of cardiac cavities and angiocardiography, closed cardiac injuries, cardiac surgery [21, 34]. Provoking factors also include stress and emotional excesses, increased body temperature, physical and mental stress, overdose of cardiac glycosides and sympathomimetics. Organic causes of PT include congenital and acquired carditis, endomyocardial fibroelastosis, idiopathic cardiomyopathies, congenital heart defects (atrioventricular communications, ASD, Ebstein's anomaly, etc.). However, in 50–70% of children with PT, organic heart pathology cannot be detected [2, 21].
The triggering mechanism for the occurrence of this type of tachyarrhythmia is an extrasystole, often very early, atrial or ventricular (“R to T”), and the paroxysm of tachycardia ends with a compensatory pause. The origin of PT is based on two mechanisms:
- 1st - the occurrence of a circular movement of the re-entry excitation wave with re-entry and a closed circle of impulse circulation at any level of the conduction system of the heart;
- 2nd - the emergence of a pathological heterotopic focus (focus) of automatism in any part of the conduction system with high pesmaker activity, reminiscent of a group or continuous extrasystole.
More often, tachyarrhythmias are based on the re-entry mechanism with longitudinal dissociation and the presence of two impulse pathways: normal (α) and blocked (β). The impulse travels anterograde along the normal path and is delayed along the blocked one. Having passed along the normal α path and excited a certain muscle segment, the impulse returns retrograde along the β path, which was previously blocked in the anterograde direction. By this time, the α path has already left the refractory phase, and the impulse can re-enter it again. If this cycle is repeated, then a circular regular re-excitation of the myocardium occurs in the form of a short “volley” paroxysm or a longer attack of tachyarrhythmia [1, 2, 4, 20–22, 45].
Among all heart rhythm disorders, supraventricular tachycardias (SVT) occupy a special place, steadily attracting the attention of researchers and clinicians over the past decade. SVT is a group of clinically and electrophysiologically polymorphic arrhythmias, united by a common feature: the presence of at least three consecutive heartbeats emanating from the zone of abnormal myocardial excitation proximal to the His bundle branch with a frequency of more than 100 beats/min in adults and a frequency exceeding the upper limit age norm by 15% in children [19]. They belong to narrow QRS complex tachycardias.
Being the second most common rhythm disorder after extrasystole, tachyarrhythmias in childhood are accompanied by a significantly larger number of complications, which is the main reason for sending children with rhythm disturbances to a cardiac surgery clinic [34]. SVT is less commonly associated with organic heart disease and left ventricular dysfunction, but there is a significant number of complaints, a marked decrease in exercise tolerance, leading in some cases to the development of heart failure and patient disability, the presence of such dangerous clinical manifestations as presyncope and syncope, sudden arrhythmic death (2–5%) allow us to consider SVT as a potentially life-threatening arrhythmia [31].
The main mechanisms of development of SVT include re-entry, ectopic automaticity and trigger activity [1, 2, 4, 21, 31].
Re-entry, or re-entry of the excitation wave, is the most common mechanism for the occurrence of paroxysmal cardiac arrhythmias, which is caused by the circular movement of the excitation wave in the myocardium and the fibers of the conduction system of the heart. For the development of re-entry, four conditions are necessary: the presence of at least two conduction pathways, a unilateral blockade in one of them, a slowdown in conduction along the other pathway, and a retrograde return of excitation along the previously blocked pathway to the point of depolarization. The re-entry circle can arise both in the presence of an anatomical basis (additional conduction pathways, AV dissociation - macro-re-entry) and functional heterogeneity of the myocardium (micro-re-entry).
Ectopic automaticity is a normal property of cells of the specialized conduction system of the heart. The cells of the sinus node have this ability to carry out spontaneous depolarization during diastole, which determines the maximum frequency of the impulses generated by it, as a result of which this node acts as the dominant pacemaker of the heart. Paroxysmal supraventricular arrhythmias can be caused by increased diastolic depolarization in ectopic foci located in the contractile atrial myocardium or in the fibers of its conduction system, as well as within the AV junction. Ectopic focal tachycardia often becomes the cause of non-paroxysmal supraventricular tachycardia, one of the signs of which is that its onset does not depend on conduction delay, and it can begin at any time in the atrial diastolic cycle, and the morphology of the P wave changes depending on the location of the source of excitation in the atria.
Under certain pathological conditions that cause a decrease in the resting potential, cells of the conduction system of the heart and myocardium also acquire the ability for automatic activity due to a different mechanism - the so-called trace potentials, which lead to a single or repeated excitation of the cell in response to previous depolarization. This type of activity is called trigger activity. It can manifest itself in various parts of the conduction system of the heart and serve as a mechanism for the occurrence of paroxysmal supraventricular arrhythmias. Trigger activity differs from ectopic automatism in that there is no spontaneous depolarization phase, and the focus of automatism begins to function only after a premature contraction. It is assumed that some types of arrhythmias that occur during an overdose of glycosides are the result of trigger activity. Afterpotentials may be enhanced after administration of catecholamines or frequent myocardial stimulation. Potassium salts, by reducing the amplitude of trace potentials, have a therapeutic effect.
In cardiological practice, the most common clinical forms of paroxysmal supraventricular tachyarrhythmias are the following [1, 8, 31, 42, 43, 45]:
- atrial tachycardia;
- atrioventricular nodal tachycardia;
- atrioventricular reciprocal tachycardia.
According to modern concepts, atrial tachycardia is a supraventricular tachycardia with localization of an abnormal electrophysiological mechanism of excitation in the atrial myocardium, including re-entry and ectopic tachycardia from the region of the sinus node and excluding atrioventricular nodal and reciprocal tachycardia [18]. Reciprocal atrial tachycardias are more often paroxysmal, and automatic ones are chronic (constant or continuously recurrent). Although, based on clinical and ECG data, it is difficult to distinguish automatic atrial tachycardia from arrhythmia developing by the re-entry mechanism, there are also a number of differential diagnostic signs. Automatic atrial tachycardia cannot be caused or stopped by pacing, which is typical for reciprocal arrhythmias. Stimulation of the atria at a rate higher than the rate of automatic atrial tachycardia only temporarily suppresses the arrhythmia; after cessation of stimulation, it resumes. The first P wave of automatic atrial tachycardia is similar to subsequent P waves. In reciprocal tachycardia, the shape of the atrial extrasystole complex, with which the attack usually begins, differs from subsequent P waves, the morphology of which depends on the location of the impulse circulation [4].
In addition, almost all researchers agree on the following: in children, a violation of automaticity can be considered the predominant cause of the development of atrial tachycardia, and the arrhythmia itself is quite often persistent or chronic, lasting months and sometimes years, and can lead to the development of cardiomegaly [1 –3, 7, 10, 21, 27, 31].
According to etiological factors, atrial tachyarrhythmias can be divided into congenital (aneurysms, diverticula, cardiomyopathies) and acquired (postmyocardial cardioscleosis or other diseases with damage to the atrial myocardium, congenital heart defects, etc.). A separate group consists of the so-called incisional atrial tachyarrhythmias that occurred after open-heart intervention.
A clinical and pathogenetic classification of atrial tachycardias has been developed [7, 12]. Yu.M. Belozerov divides atrial tachyarrhythmias into sinus, inappropriate sinus, sinus nodal reciprocal, atrial, multifocal atrial tachycardia, flutter and atrial fibrillation [1].
Inappropriate sinus tachycardia (NST) is an accelerated baseline sinus rhythm in the absence of a stressor. In this situation, healthy children may have an elevated resting heart rate and an excessive heart rate response even to minimal physical activity. The mechanism underlying NST may be increased sensitivity of the sinus node to autonomic input or an anomaly within the sinus node, its autonomic output.
Sinus nodal reentrant tachycardia is caused by a reentrant circuit located within or adjacent to the sinus node, so it has a sudden onset and end.
Multifocal atrial tachycardia occurs within the atrium; It is based on P waves of 3 or more morphologies. This type of tachycardia is rare.
Atrial fibrillation - chaotic atrial rhythm with atrial wave frequency up to 600 beats/min (350–600 beats/min); characterized by complete disorganization of electrical processes in the atrial myocardium. Chaotic, asynchronous excitation covers individual muscle fibers or small groups of fibers, which excludes full systolic contraction of the atria [1, 11]. In childhood, atrial fibrillation occurs in congenital and rheumatic heart defects, conditions after Mustard surgery, ASD, tetralogy of Fallot, primary and secondary cardiomyopathies, thyrotoxicosis, and is also associated with atrioventricular reentrant tachycardias [41, 45].
Atrial flutter is a type of tachyarrhythmia originating above the AV node, with an atrial rate of 250–359 beats/min. The mechanism of atrial flutter is based on the circulation of excitations, i.e. repeated return of the impulse to the same area. In older patients, frequent relapses of atrial flutter occur in 95% of cases due to organic heart diseases [44, 45]. In contrast to fibrillation, atrial flutter is characterized by a regularly coordinated atrial rhythm with a frequency of 250 to 300 beats per minute [19].
Atrial flutter and atrial fibrillation are combined into one concept - atrial fibrillation, which occurs in acute (paroxysmal) and chronic forms. And although it is not a common rhythm disorder in childhood, in the absence of adequate therapy it has an extremely unfavorable prognosis and a high risk of sudden cardiac death [1, 2, 4, 11, 20, 21, 24, 37].
Atrial tachycardia in some cases must be differentiated from sinus tachycardia. Differential diagnosis can be difficult, but it is important for choosing treatment tactics. Physical activity and vagal maneuvers significantly affect the frequency characteristics of sinus tachycardia and have little or no effect on them in atrial tachycardias. Long-term ECG recording in patients with chronic atrial tachycardia can reveal short periods of sinus rhythm (especially at night), which also helps in differential diagnosis.
In patients with atrial tachycardia, the prognosis is usually determined by the underlying disease. Mortality among them in the absence of other pathology other than heart rhythm disturbances is very low. However, if the arrhythmia occurs with high frequency and for a long time, then even in patients without organic heart damage, cardiomegaly develops, the ejection fraction decreases and congestive heart failure appears.
Paroxysmal AV nodal tachycardia is more common in school-age children and adolescents and rare in newborns and preschool children. It is believed that the trigger factor in the development of this type of tachycardia is physical activity [45, 46]. The electrophysiological basis of paroxysmal AV nodal tachycardia is the presence inside the node of two conduction pathways that have different functional properties. One of these pathways (fast) is located in the lower part of the interatrial septum and conducts impulses from the atria to the ventricles at a higher speed, having a longer effective refractory period. The other path (slow) is located above the mouth of the coronary sinus closer to the tricuspid valve annulus and conducts the impulse at a lower speed, having a shorter duration of the effective refractory period. These two pathways connect at the entrance to the AV node, closing the circulation ring of the excitation wave. In normal sinus rhythm, the impulse is usually conducted through the fast pathway, so the functioning of the slow pathway of the AV node is not evident on the ECG. There are 2 forms of this tachycardia: typical (slow-fast), accounting for 90% of all cases and characterized by the fact that the slow pathway conducts the impulse in the anterograde direction, and the fast one in the retrograde direction, and atypical (fast-slow), characterized by the opposite direction of the impulse. and the resulting prolongation of the RP interval [1, 19, 21, 42, 45]. Due to the fact that the excitation of the ventricles and atria occurs almost simultaneously during a paroxysm of tachycardia, it is rarely possible to register P waves on the ECG. They, as a rule, merge with the ventricular complexes. If the P waves can still be identified, then they are negative in leads II, III and aVF, which indicates retrograde excitation of the atria.
There are 3 variants of paroxysmal AV reciprocal tachycardia:
1) AV nodal reciprocal AT with circular circulation of the impulse in the AV node or in the paranodal pathways;
2) AV-reciprocal AT in Wolff-Parkinson-White (WPW) syndrome (with orthodromic and antidromic impulse circulation);
3) AV-reciprocal AT with hidden additional retrograde pathways [8, 21].
Transesophageal electrophysiological study, which is a non-invasive and valuable method for establishing the pathogenetic features of tachyarrhythmias in childhood, helps to correctly differentiate these types of tachycardias, as well as distinguish AV-reciprocal antidromic tachycardia from ventricular tachycardia, and identify additional hidden pathways [8].
It has now been proven that the circular movement of the impulse occurs not in the sinus node itself, but in the paranodal (in the lower part of the right atrium) atrionodal bundles, which have different speeds of anterograde and retrograde conduction [21].
In AV-reciprocal AT against the background of WPW syndrome and the presence of additional conduction pathways (APP), the circular movement of the impulse is a typical macro-re-entry, since the loop includes the AV node, the trunk of the atrioventricular bundle, the Purkinje network, the ventricular myocardium, the AP, and AV -knot. This loop is represented in the upper part by the atrium, and in the lower part by the ventricle of the heart. The movement of an impulse along the re-entry loop can be carried out in two directions. In the orthodromic version of the AV reciprocal AT, the impulse moves anterograde through the AV node and retrograde through the AP. This is the most common type of AV reciprocal AT in WPW syndrome. The attack begins after an early atrial extrasystole, the heart rate quickly reaches a stable maximum (220–250 beats/min), regular. The QRS complexes are narrow, since the impulse spreads evenly to both ventricles of the heart, but sometimes a tachydependent functional blockade of one of the branches of the atrioventricular bundle occurs [1, 2, 4, 8, 20–22, 24, 43, 45].
The antidromic variant of AV-reciprocal AT in WPW syndrome also begins with an atrial extrasystole and is characterized by anterograde movement of the impulse through the AP and retrograde through the His-Purkinje system and the AV node to the atrium. Due to the faster conduction of the impulse anterogradely along the AP to the ventricles, early activation of part of the myocardium of the ventricle of the heart occurs with the formation of a delta wave. The QRS complexes are widened by the value of the delta wave, aberrant, but monomorphic, the P waves are inverted in leads II, III, aVF, the RP interval is widened, recorded behind the QRS complex. The heart rate exceeds 200–250 beats/min [1, 2, 4, 20–22, 24, 43, 45].
In addition, there is a variant of AV-reciprocal AT, in which during the attack period almost all the signs of orthodromic AV-reciprocal AT are revealed (as in WPW syndrome), but outside the attack, a delta wave is never recorded on the ECG. This allows us to deny the presence of ventricular preexcitation and assume the existence of hidden additional pathways with selective retrograde impulse conduction. Just as with orthodromic AV-reciprocal AT, the attack begins with an atrial extrasystole with a critical coupling interval [1, 8, 19, 21].
ECG signs of various types of supraventricular tachycardia are presented in table. 2.
The clinical picture of supraventricular PT does not depend on the location of the PT focus. The attack begins suddenly, with a heart “push” and a feeling of palpitations. Some children, anticipating the onset of an attack, sit up or go to bed [36]. Many school-age children with a long “seizure history” clearly define the beginning and end of an attack. In addition to the feeling of heartbeat, unpleasant sensations appear, sometimes pain in the heart and epigastrium, and nausea. Severe weakness and dizziness occur. Depending on the characterological characteristics and emotionality of the patients, some endure the attack relatively calmly, others complain of fear of death, “abnormal pulsation in the temples,” the readiness of the heart to “jump out of the chest,” incomplete inspiration and lack of air. Children also present asthenovegetative complaints: fatigue, sleep disturbance, headache, sudden attacks of weakness, dizziness, poor transport tolerance, cardialgia. The main symptoms of supraventricular PT are reflected in table. 3.
Young children have no specific complaints. The reason for contacting a pediatrician is the mother’s complaints about restless sleep, refusal to feed, and severe sweating of the child. Restlessness followed by lethargy, shortness of breath, cough, cold sweat, fainting, and sometimes convulsions can occur during a paroxysm [2, 21, 26].
Analysis of the pulsogram in children with paroxysmal tachycardia showed that they are characterized by a decrease in vagosympathetic influences on the heart rate, expressed in lower daytime and nighttime heart rate values compared to healthy ones, combined with a low functional reserve for heart rate adaptation [34].
To be continued in the next issue
Diagnostics
The task of a cardiologist who examines a child with suspected tachycardia is to make sure that the signs he has do not indicate other diseases, for example, bronchial asthma. Also during the examination, he looks for the cause of the disease. To do this, the specialist uses:
- ECG and daily monitoring to analyze how the heart rhythm changes during the normal activity of a small patient;
- EchoCG and MRI to make sure there are no heart pathologies;
- an electrophysiological study to check how the electrical impulse travels through the heart muscle;
- laboratory methods: urine, blood analysis;
- EEG of the brain to make sure that the activity of the central nervous system is not impaired.
Classification of congenital heart defects in children:
- With unchanged or slightly changed pulmonary blood flow (anomalies of the location of the heart, pathologies of the aortic arch, aortic stenosis, atresia of the aortic valve, insufficiency of the pulmonary valve, stenosis, atresia and insufficiency of the mitral valve, heart with three atria, pathologies of the arteries and conduction system).
- With hypervolemia of the pulmonary circulation: Without early cyanosis (open duct in the arteries, defective septa between the ventricles or atria, aortopulmonary fistula, Lutambashe syndrome).
- With cyanosis (atresia with a septal defect between the ventricles, open ductus in the arteries with pulmonary hypertension and blood flow into the aorta from the pulmonary trunk).
- Without cyanosis (isolated pulmonary stenosis).
There is also a classification of congenital heart defects in newborns, which is more understandable for the common man:
- So-called “blue” defects (accompanied by early cyanosis (blue skin); among them are tetralogy of Fallot, pulmonary atresia, transposition of the great vessels).
- So-called “white” or “pale” defects (may be accompanied by pallor of the skin or occur without pronounced symptoms and are detected randomly during a preventive examination of the child; among them are defects of the septa between the ventricles and atria).
Treatment and prognosis
In case of sudden attacks of tachycardia, the child should be taken out into the fresh air, tight clothes should be removed, a damp handkerchief should be placed on the forehead, and then a doctor should be called. If there is no pathology, and hormonal changes and stress lead to an acceleration of the heart rate, to treat tachycardia in children, the cardiologist will prescribe drug therapy (beta-blockers, cardiac glycosides, calcium antagonists, sedatives). Auxiliary measures: physical therapy, valgus techniques. To alleviate the condition, a diet is recommended in which it is undesirable to consume chocolate, tea, spicy, and salty foods.
Children who follow the doctor's recommendations usually return to their previous lives and activities. In rare cases, when the disease develops due to other serious pathologies that cannot be treated conservatively, surgery is prescribed.
Treatment for the diagnosis of congenital heart disease in newborns
Treatment methods depend on the type of heart defect:
- Minimally invasive procedures
- Radical surgery
- Heart transplant
- Drug therapy
- Long-term therapy
If the heart defects are not very serious, minimally invasive procedures can be used. Their essence is that a thin catheter is inserted into the heart through the femoral vein, and the necessary instruments are delivered to the defect inside the catheter.
The most radical but effective method of treating congenital heart disease is surgery. This is a traditional open intervention with opening of the chest and the heart itself. Most of these operations are performed using a heart-lung machine. After heart surgery, a child faces a long and difficult recovery period, but sometimes it is the only possible way to cure.
Heart transplantation is used in the most severe cases, in which traditional surgery is helpless in case of severe congenital heart disease.
Drug therapy is used mainly for auxiliary purposes, improving the functioning of the heart and blood flow.
Long-term therapy involves several consecutive operations on congenital heart disease.