Cardiomyopathy is a primary myocardial lesion that is not caused by an inflammatory, tumor or ischemic process. Often the pathology has an unclear etiology. To diagnose a patient with cardiomyopathy, it is necessary to exclude other diseases: congenital developmental anomalies, valvular heart defects, damage caused by systemic vascular diseases, arterial hypertension, pericarditis, etc. Depending on the nature of the anatomical and functional changes in the heart muscle, the following types of cardiomyopathy are distinguished:
- dilatational (stagnant);
- hypertrophic (can be asymmetric and symmetric, obstructive and non-obstructive);
- restrictive (distinguish between obliterating and diffuse);
- arrhythmogenic right ventricular.
Causes
The etiology of this pathology has not been fully studied to date. There are a number of probable causes that can cause the development of cardiomyopathy:
- hereditary predisposition (genetic defect that causes improper formation and functioning of myocardial muscle fibers);
- various viral infections (Coxsackie, herpes, influenza, etc.);
- previous myocarditis;
- damage to heart cells by toxins and allergens;
- disturbances of endocrine regulation (negative effects of growth hormone and catecholamines);
- immune system disorders.
Types and symptoms of cardiomyopathy
Dilatational
There are no obvious symptoms of this type of cardiomyopathy until heart failure develops. Manifestations of the disease depend on the involvement of one or both chambers of the heart in the beginning pathological process. Due to the oxygen deficiency that occurs with cardiomyopathy, shortness of breath occurs, fatigue increases, and heart rate increases. At the initial stage of the disease, the listed symptoms are associated only with exposure to physical activity, and over time they appear at rest. Insomnia, dizziness, pain in the chest and under the left shoulder blade, and swelling occur.
Hypertrophic
With this pathology, relaxation (decreased extensibility) of the heart chambers is impaired, blood circulation worsens, the shape of the left ventricle changes, the septum thickens, as a result, pressure increases, and the walls of the outflow tract become thinner. Symptoms of hypertrophic type cardiomyopathy, along with shortness of breath and chest pain, are the patient’s tendency to faint and increased heartbeat. With this pathology, rhythm disturbance can even lead to sudden death.
Restrictive
At the initial stage, patient complaints are practically no different from those listed for other types of cardiomyopathy. But over time, leg swelling, shortness of breath and fatigue give way to more severe symptoms. The liver stops functioning normally, increases in size, and then dropsy develops. The instability of the heart rhythm reaches such a degree that it causes frequent fainting.
Arrhythmogenic
The most common symptom is ventricular arrhythmia. Among the complaints, patients name paroxysmal rapid heartbeat, most often during significant physical exertion. Patients with the listed symptoms, in whose family there have already been cases of early death with such manifestations, are considered to be at increased risk.
Restrictive cardiomyopathy
Restrictive cardiomyopathy is such a rare and polyetiological pathology that it is difficult to provide reliable statistical data on its prevalence. However, among other types of cardiomyopathies, it traditionally stands out third. Back in 1973, Professor I. F. Goodwin proposed a definition of cardiomyopathy - this is an acute, subacute or chronic lesion of the cardiac muscle of the heart of an unknown or unclear etiology involving the endocardium or pericardium, which is not a consequence of structural deformation of the heart, hypertension in the systemic or pulmonary circulation or coronary atheromatosis. This diagnosis is an exception, but the definition is very detailed. Of course, it has already been revised several times, and the following interpretation has been proposed: cardiomyopathy is a disorder characterized by morphological and functional abnormalities of the myocardium in the absence of other heart pathologies . However, this definition does not tell us about the very essence of the disease, so there are three types of CMP that are completely different from each other in morphology and pathogenesis: hypertrophic, dilated and restrictive , which will be discussed in this post.
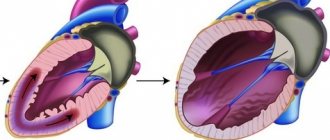
In 2013, the World Heart Federation proposed a new classification MOGE(S) , which in its essence has no practical significance, but is accepted to indicate the morphology, degree of involvement of organs and systems in the process, hereditary predisposition, etiology and stage of development of CMP. Restrictive cardiomyopathy is distinguished by specific symptoms: it is a lesion of the heart in which, due to reduced elasticity of the myocardium and/or endocardium, the diastolic function of the heart is impaired . If you mentally imagine a picture in your head, it will be a heart with hard, inelastic walls of the ventricles, which are filled with blood at each diastole, unable to stretch to accept it, and “choking” with blood.
Etiology In 50% of cases, RCM is considered idiopathic. All other options are independent diseases or pathological processes, ultimately leading to rigidity of the ventricular walls. The frequency of occurrence of diseases causing RCM is as follows:
- amyloidosis (from the course of pathological anatomy we know well that amyloid is an abnormal insoluble heavy protein; when infiltrating the myocardium, it becomes dense and inelastic. In addition, due to compression of arterioles, local myocardial ischemia develops, which is a trigger signal for fibroblasts - fibrosis occurs, which is represented by coarse fibrous connective tissue that prevents normal muscle contraction.The myocardium is most often affected by familial amyloidosis: with this type of amyloidosis, the accumulation of a special protein transthyretin occurs - the transport protein of retinol and thyroxine) ;
- sarcoidosis;
- hemochromatosis (the accumulation of iron itself, of course, will not cause significant compaction of the myocardium. But overfilling of lysosomes with iron, their rupture and release of proteolytic enzymes can cause secondary alteration and lead to inflammation and further fibrosis of the myocardium) ;
- radiation exposure;
- Loeffler's eosinophilia and endomyocardial fibrosis (more common in the tropics and subtropics. The mechanism is associated with parasitic invasion, which causes significant eosinophilia and infiltration of myocardial eosinophils, as a result of which myocarditis and/or endocarditis develops, followed by fibrosis) ;
- systemic scleroderma;
- lysosomal storage diseases (Gaucher's disease, Fabry's disease, etc.);
- carcinoid syndrome and other diseases.
Thus, the main mechanism for the occurrence of ventricular wall rigidity is fibrosis of the heart muscle due to its inflammation and ischemia. Normally, in diastole, the chambers of the ventricles are stretched under the pressure of the blood filling them, the volume reaches a peak (about 130 ml) before the onset of systole. With rigid walls, the diastolic volume of the ventricles is constant, and the atria, figuratively speaking, have to make great efforts to deliver the entire volume of blood. End-diastolic pressure reaches critical levels, so-called diastolic overload occurs. Characterized by stagnation in the systemic and pulmonary circulation - diastolic heart failure develops. It is generally accepted that at the initial stages systolic function does not suffer, but with widespread fibrosis there is simply “nothing to contract”, heart failure progresses, acquiring a new category - systolic and diastolic heart failure. Mortality within two years after the onset of the first symptoms reaches 35–50%, as the risk of life-threatening complications steadily increases: thrombosis, cardiac arrhythmias due to fibrosis in the pathways of the cardiac conduction system (AV block) and direct progression of heart failure.
What are the clinical manifestations of RCM? First of all, these are signs of stagnation in the systemic circulation: ascites, swelling of the legs, hepatomegaly , etc. There are also signs of stagnation in a small circle: shortness of breath, suffocation, cough, hemoptysis, etc. palpitations and syncope is also characteristic . A physical examination often reveals cyanosis (from acrocyanosis to central), congestive wheezing in the lungs, weakening of heart sounds, the appearance of a third sound caused by the impact of a portion of blood on the tight wall of the ventricles, and systolic murmur of regurgitation.
Diagnostics The tasks of diagnosing RCM are to exclude all other myocardial lesions, and above all other types of cardiomyopathies and clinically similar constrictive pericarditis. Laboratory diagnostics cannot help in this case, but you can see a significant increase in eosinophils in a clinical blood test or circulating immune complexes in the corresponding immunological reactions. ECG changes in RCMP are nonspecific; only consequences of damage to the myocardium and conduction system of the heart can be identified:
- Decreased amplitude of the QRS complex;
- Signs of atrial overload: P-pulmonale, P-mitrale;
- ST segment depression;
- T wave inversion;
- Rhythm and conduction disorders: AF, AV block, etc.
Chest X-ray will help to identify blood stagnation in the pulmonary circle (enhanced pulmonary pattern, expansion of the roots of the lungs due to the vascular component), you can also see the size and configuration of the heart - the size is normal or slightly increased, dilatation of the atria. But transthoracic echocardiography will provide more information:
- The main diagnostic criterion is the restrictive type of diastolic dysfunction;
- Systolic function is not impaired (in the later stages of CHF it may be reduced);
- Severe atrial dilatation;
- Reduction of the cavity of the affected ventricle;
- Functional mitral and/or tricuspid regurgitation;
- Signs of pulmonary hypertension;
- The thickness of the walls of the heart is usually not increased (however, with amyloidosis, on the contrary, it can be significantly increased).
To exclude the diagnosis of constrictive pericarditis, a CT or MRI is performed, which can evaluate the condition of the pericardial layers and the presence of calcification. Cardiac catheterization with endomyocardial biopsy is necessary to identify the etiology of RCM (eosinophilic infiltrate, sarcoid granulomas, amyloid, etc.) .
Treatment Conservative treatment in this case is limited to alleviating the symptoms of CHF, according to national recommendations:
ACE inhibitors
ACE inhibitors are indicated for all patients with CHF, regardless of the stage of the process. Of all the ACEIs registered in the Russian Federation, the most relevant for the correction of CHF are the “classical” ACEIs - enalapril and captopril (SOLVD treatment, SOLVD prevention, V - HeFT II and CONSENSUS). The use of, for example, lisinopril in this case is not justified due to the fact that RCM often manifests itself in severe heart failure and in such cases the kidney function is already severely impaired, and since lisinopril is completely eliminated by the kidneys, its use should be limited. In these cases, it is more profitable to use fosinopril and spirapril , which have two routes of elimination from the body. In addition, the ALLHAT study demonstrated that lisinopril was significantly inferior to diuretics in preventing the development of CHF (unlike other ACE inhibitors).
β-adrenergic receptor blockers
Rules for prescribing BAB:
- Bisoprolol, carvedilol, metoprolol succinate and nebivolol are recommended. Metoprolol tartrate is not recommended for the treatment of CHF.
- Treatment with beta blockers should begin carefully, starting with 1/8 ter. doses are increased slowly (no more than once every 2 weeks or 1 month).
- It is necessary to monitor blood pressure, heart rate, and diuresis. When the symptoms of CHF increase, the dose of ACE inhibitors and diuretics is first increased; if ineffective, the dose of beta blockers is temporarily reduced.
- In case of hypotension, first of all, the dose of vasodilators should be reduced; if ineffective, the dose of beta blockers should be reduced; for bradycardia, reduce the dose of drugs that affect heart rate; if ineffective, reduce the dose of beta blockers. When a stable state is achieved, resume taking beta blockers or continue titrating their dose.
- In case of decompensation, phosphodiesterase inhibitors or levosimendan are prescribed.
Contraindications to the use of beta blockers:
- Bronchial asthma or other severe lung pathology;
- Symptomatic bradycardia less than 50 bpm;
- Symptomatic hypotension less than 85 mmHg;
- AV blockade 2-3 degrees;
- Obliterating endarteritis.
Diuretics
Indicated only to reduce edema syndrome. Prescribed only for clinical signs of stagnation (stage IIA, IIFC according to the classification of OSHF). For future use, do not treat with diuretics, because they, as mentioned above, do not slow down the progression of CHF. Algorithm for prescribing diuretics depending on the severity of CHF:
FC I - do not treat with diuretics;
II FC (without stagnation) – small doses of torasemide (2.5-5 mg);
FC II (stagnation) - thiazide (loop) diuretics + spironolactone 100-150 mg;
III FC (maintenance treatment) – loop diuretics (preferably torasemide) daily in doses sufficient for balanced diuresis + spironolactone (small doses) + acetazolamide (0.25 mg 3 times a day for 3-4 days once every 2 weeks);
III FC (decompensation) – loop (preferably torasemide) + thiazide + aldosterone antagonists in doses of 100-300 mg/day + acetazolamide;
IV FC - loop diuretics (sometimes twice a day or IV) + thiazide + spironolactone + acetazolamide +, if necessary, isolated ultrafiltration or mechanical removal of fluid.
Cardiac glycosides
They are used to reduce the frequency of hospitalizations and do not affect mortality. First of all, before all the above drugs, it is used for atrial fibrillation and heart failure. In sinus rhythm, digoxin is the fourth drug after ACE inhibitors, beta blockers and diuretics.
Non-drug treatment is also recommended (smoking cessation, diet, exercise), but taking into account the huge mortality rates, it does not have much effect on the prognosis. There is also the prevention of thromboembolic complications with anticoagulant therapy and normalization of heart rhythm if necessary. However, the only effective type of treatment in this case is heart transplantation .
Sources
- Muchtar E., Blauwet LA, Gertz MA Restrictive cardiomyopathy: genetics, pathogenesis, clinical manifestations, diagnosis, and therapy //Circulation research. – 2021. – T. 121. – No. 7. – pp. 819-837.
- Mankad AK, Shah KB Transthyretin Cardiac Amyloidosis //Current cardiology reports. – 2021. – T. 19. – No. 10. – P. 97.
- Filippetti L. et al. Hypereosinophilic cardiac disease //Acta cardiologica. – 2021. – T. 72. – No. 1. – pp. 9-18.
- Chazov, E. I. Guide to cardiology. In 4 volumes. Volume 4. Diseases of the cardiovascular system (II) / E. I. Chazov. and others - M.: Praktika, 2014. - 976 p.
- Mareev V. Yu. et al. National recommendations of OSHF, RKO and RNMOT for the diagnosis and treatment of CHF (fourth revision). Approved at the OSCH Congress on December 7, 2012, at the OSCH Board on March 31, 2013 and at the RKO Congress on September 25, 2013 // Journal of Heart Failure. – 2013. – T. 14. – No. 7. – pp. 379-472.
Consequences and complications
For all types of cardiomyopathy, a characteristic complication is progressive heart failure. In addition, arterial and pulmonary thromboembolism, cardiac conduction disturbances, and severe forms of arrhythmia may develop. There is a high risk of sudden cardiac death. If the patient has bad habits, such as smoking and drinking alcohol, the prognosis worsens significantly. Life expectancy may also be affected by the presence of thromboembolism and tachycardia, especially if cardiomyopathy is untreated. Today, alleviating the course of the disease for such patients is becoming possible thanks to modern early diagnostic technologies.
Diagnostics
Diagnosis of cardiomyopathy necessarily includes a description of the clinical picture and data from additional studies. The most common method - electrocardiography (ECG) - allows you to record signs of hypertrophy of the heart muscle and identify various forms of rhythm and conduction disorders. Echocardiography (EchoCG) is especially informative, as it helps determine myocardial dysfunction. Thanks to X-ray data, dilatation (persistent increase in the lumen), hypertrophy (increase in volume and mass) of the heart muscle, as well as congestion in the lungs are detected. In some cases, as part of the diagnosis of cardiomyopathy, ventriculography (x-ray examination of the ventricular system), magnetic resonance imaging (MRI) of the heart and multislice computed tomography (MSCT), as well as probing of the cavities of the heart to collect biomaterials for further morphological research are indicated.
Treatment
Due to the lack of specific therapy, treatment of cardiomyopathy is aimed at preventing complications incompatible with life. If the disease is in a stable phase, all measures are prescribed and carried out on an outpatient basis. Must be under the supervision of a cardiologist. The indication for periodic planned hospitalization is the presence of severe heart failure, for emergency - the development of intractable paroxysms of arrhythmias, as well as thromboembolism and pulmonary edema.
Drug treatment. For various manifestations of cardiomyopathy, it is advisable to prescribe:
- diuretics, which reduce pulmonary and systemic venous congestion;
- cardiac glycosides, which help combat disorders of contractility and pumping function of the myocardium;
- antiarrhythmic drugs that help regulate heart rhythm;
- anticoagulants and antiplatelet agents to prevent the occurrence of thromboembolic complications of cardiomyopathy.
Surgery. Indicated in extremely severe cases. Among the methods practiced today are septal myotomy (resection of an enlarged portion of the interventricular septum) and mitral valve replacement, as well as whole heart transplantation.
In addition, experts emphasize the need to reduce physical activity and adhere to a diet, an important condition of which is limiting the consumption of animal fats and salt. It is strongly recommended to eliminate bad habits and exposure to negative external factors. Compliance with these recommendations will significantly reduce the load on the myocardium and slow down the progression of heart failure.
Clinical picture
Circulatory disorders are typical for dilated cardiomyopathy The heart's response to physical activity is somewhat weaker than always, and the output is also reduced. Mitral and tricuspid regurgitation is diagnosed, the level of which is proportional to the degree of heart failure. There are cases of embolism in the pulmonary and systemic circulation.
In the hypertrophic form, the most important circulatory disorders concern diastole, and the ejection fraction from the left ventricle is higher than normal. Very often, an increase in end-diastolic pressure and inhibition of mitral valve opening are diagnosed, which in turn is a sign of regurgitation.
Filling is impaired as a result of improper relaxation and due to pathology of the shape of the ventricular cavity.
With endomyocardial fibrosis, there is a combination of impaired diastolic function with pericardial effusion in the later stages of development and a disorder of the pumping function of the heart.
With hypertrophic cardiomyopathy , complaints and symptoms of disorders are often not detected. But in patients with difficulties in the outflow tract, three characteristic signs are observed: a jerky and uneven pulse,
- murmur during auscultation of the heart, which occurs late and is heard at the apex and at the left edge of the sternum,
- palpable contractions of the left atrium.
In restrictive cardiomyopathy , the clinical symptoms (shortness of breath and weakness) are similar to those of diastolic heart disease, and angina pectoris is rare. This form of cardiomyopathy often affects children.
With some form of endomyocardial fibrosis, inflammatory fluid may be detected in the pericardium, which is sometimes the main symptom. Laboratory blood tests show an increase in the level of leukocytes.
A high degree of reliability in diagnosing cardiomyopathies is provided by a modern approach, which includes electrocardiography, radioisotope ventriculography, radiography, and myocardial biopsy.
Prognosis for cardiomyopathies
With regard to cardiomyopathy, the prognosis is unfavorable: the steady progression of heart failure causes a high probability of arrhythmic, thromboembolic complications, as well as sudden death of the patient. According to statistics, with dilated cardiomyopathy, the 5-year survival rate is 30%. Systematic treatment can stabilize the patient’s condition indefinitely. There are also cases of exceeding 10-year survival after heart transplantation. Surgical treatment, for example, for hypertrophic cardiomyopathy, gives a positive result, but is associated with a high risk of death of the patient during or after surgery. Women who have been diagnosed with cardiomyopathy are not recommended to become pregnant, since pregnancy and childbirth are associated with a high probability of maternal death.
Publications in the media
Restrictive cardiomyopathy (from Latin restrictio - restriction; RCM) is a primary or secondary lesion of the heart, characterized by impaired diastolic function of the ventricles. RCM is characterized by a predominant impairment of diastolic function and an increase in ventricular filling pressure with normal or slightly altered contractile function of the myocardium and the absence of its significant hypertrophy and dilatation.
Statistical data. The disease is observed extremely rarely. In Russia, idiopathic RCM is practically not observed; in the tropics it is known as Loeffler's disease.
Etiology • Idiopathic RCM •• Endomyocardial fibrosis •• Eosinophilic endomyocardial disease (Loeffler's disease) • Secondary RCM •• Hemochromatosis •• Amyloidosis •• Sarcoidosis •• Scleroderma •• Carcinoid heart disease •• Glycogen storage diseases of the heart •• Radiation damage to the heart •• Drugs (anthracycline intoxication).
Genetic aspects. A rare form is known - familial RCM (*115210, Â).
Pathogenesis
• Characterized by increased rigidity (or decreased compliance) of the ventricular wall, which may be a consequence of endo- or myocardial fibrosis of various etiologies (endomyocardial fibrosis, systemic scleroderma) and infiltrative diseases (amyloidosis, hereditary hemochromatosis, tumors).
• The main point in the pathogenesis is impaired filling of the left ventricle due to thickening and increased rigidity of the endocardium and myocardium as a result of amyloid infiltration or fibrosis. There is a significant increase in diastolic pressure in the left and right ventricles and pulmonary hypertension. Subsequently, diastolic heart failure develops. Left ventricular systolic function does not deteriorate for a long time.
• The development of heart failure in such patients is not accompanied by an increase in the volume of the left ventricle - on the contrary, it may decrease. Similar hemodynamic changes are observed in constrictive pericarditis.
Pathomorphology. Usually both ventricles are affected, but the size of their cavities remains within normal limits or decreases (with endomyocardial fibrosis). The atria are usually dilated • With endomyocardial fibrosis, the endocardium and valve apparatus are affected, which leads to the occurrence of a corresponding defect (stenosis and/or insufficiency) • Amyloidosis is characterized by pronounced thickening and compaction of the walls of the heart.
Clinical manifestations
• Patients usually complain of shortness of breath on exertion, cardiac pain on exertion, peripheral edema, pain in the right hypochondrium, and abdominal enlargement.
• Examination may reveal distended jugular veins. The Kussmaul symptom is characterized by increased swelling of the jugular veins during inspiration.
• During auscultation, you can hear a “gallop rhythm”, a systolic murmur of tricuspid and mitral valve insufficiency. In pulmonary hypertension, its characteristic auscultatory signs are determined. In the lungs, with significant stagnation of blood, wheezing is heard.
• Characterized by liver enlargement and ascites.
Laboratory data. Characteristic changes are inherent in the underlying disease.
Instrumental data
• ECG: you can detect signs of blockade of the left branch of the His bundle (rarely - the right one), reduced voltage of the QRS complex (more typical for cardiac amyloidosis), nonspecific changes in the ST segment and T wave, various arrhythmias, signs of left atrium overload.
• EchoCG: the size of the heart cavities is not changed. In some cases, thickening of the endocardium can be detected. A characteristic manifestation of RCM is considered to be disturbances in the diastolic function of the left ventricle: a shortening of the isovolumic relaxation time, with Doppler echocardiography an increase in the peak of early filling, a decrease in the peak of late atrial filling of the ventricles and an increase in the ratio of early to late filling.
• X-ray examination - normal contours of the heart in the presence of signs of venous congestion in the lungs.
• Myocardial biopsy. The study is carried out if glycogen storage diseases are suspected. In Loeffler's disease, eosinophilic infiltration and myocardial fibrosis can be detected. The result of a myocardial biopsy may be normal, which does not exclude the diagnosis of RCM.
Diagnostics. It is necessary to suspect restrictive myocardial damage in patients with congestive heart failure in the absence of dilatation and pronounced disturbances in the contractile function of the left ventricle according to echocardiography; at the same time, the size of the left atrium and often the right ventricle are increased • The diagnosis of restrictive myocardial damage sometimes has to be made in the presence of other signs of the underlying disease. With hypereosinophilia with high leukocytosis, sometimes with hepatolienal syndrome, Loeffler's fibroplastic endocarditis with signs of myocardial damage can develop and progress • With primary amyloidosis, the disease can occur for a long time with predominant myocardial damage, which progresses from restrictive to dilatation of the heart chambers (heart failure can develop with restriction) ; in this case, at early or later stages, damage to the kidneys, intestines (malabsorption with diarrhea), tongue (macroglossia) and other signs may occur. Important for the diagnosis of amyloidosis is a morphological study of the mucous membrane of the gums or rectum, in which amyloid is found with special staining, which, in essence, makes it possible to establish the nature of the heart damage • With hemochromatosis, in addition to heart damage, liver damage, diabetes, darkening of the skin are possible , reminiscent of a tan. The diagnosis can also be made morphologically after a liver biopsy, in which deposition of iron-containing pigment is found • In the other diseases mentioned above, in which restrictive myocardial damage can develop, it is usually secondary compared to other lesions.
Differential diagnosis • With effusion and constrictive pericarditis • With left ventricular localization of fibrosis, other causes of pulmonary hypertension should be excluded (mitral stenosis, cor pulmonale, Lutembashe syndrome).
TREATMENT
As a rule, it is symptomatic and is aimed at reducing congestion in the systemic and pulmonary circulation, reducing end-diastolic pressure in the left ventricle and reducing the risk of thromboembolism.
Drug therapy • Diuretics (hydrochlorothiazide at a dose of 50 mg/day), vasodilators (for example, isosorbide dinitrate and isosorbide mononitrate 20–60 mg/day), indirect anticoagulants are used. Diuretics and peripheral vasodilators in large doses can worsen the condition of patients by reducing cardiac output (due to reduced preload) and causing arterial hypotension • Cardiac glycosides are usually not prescribed, because systolic function of the heart is preserved (they can be used only if systolic function is significantly impaired). It should be remembered that with amyloidosis, patients have increased sensitivity to cardiac glycosides as a result of the binding of digoxin to amyloid • In secondary RCM, the underlying disease is treated (for example, in the acute phase of Loeffler's disease, GCs and cytostatic agents are used) • In case of hemochromatosis, repeated bloodlettings can be effective, in which the release of excess iron from the body is accompanied by its extraction from depots in various tissues, incl. and from the heart.
Surgical treatment for fibroplastic endocarditis consists of excision of the thickened endocardium and release of the chordae tendineae and valve tissue. In case of severe insufficiency of atrioventricular valves, their replacement is performed.
Prognosis and complications. Mortality within 2 years reaches 35–50%. RCM can be complicated by thromboembolism, arrhythmias, and progression of heart failure.
Synonyms • Becker's disease • Loeffler's syndrome • Loeffler's endocarditis • Fibrous endocarditis • Fibroplastic endocarditis • Endomyocardial disease • African cardiomyopathy.
Reduction. RCM - restrictive cardiomyopathy.
ICD-10 • I25.5 Ischemic cardiomyopathy
Prevention
To date, there are no preventive measures for hereditary (congenital) cardiomyopathy. However, some recommendations have been developed to reduce the risk of developing concomitant diseases that worsen its course - myocardial infarction, arterial hypertension. In general, prevention comes down to maintaining a healthy lifestyle, including physical exercise and giving up tobacco and alcohol. To identify the underlying disease (arterial hypertension, hypercholesterolemia or diabetes mellitus) at its early stage, it is important to follow the following recommendations:
- regularly visit a doctor and undergo examinations prescribed by him;
- follow all the specialist’s recommendations regarding lifestyle changes, daily routine, diet, etc.;
- take medications and other medications in strict accordance with the doctor’s prescription.
For patients at high risk of sudden cardiac death, timely implantation of a cardioverter-defibrillator, a device for stopping threatening arrhythmias, is of great importance.
If you want to undergo diagnosis or treatment of various types of cardiomyopathy under the supervision of highly qualified specialists, contact the ABC-Medicine clinic. To sign up for a consultation or ask clarifying questions, please call +7.
What pathologies can provoke the secondary form?
Secondary cardiomyopathy appears against the background of pathologies associated with the functioning of the human cardiovascular system.
The list of these diseases includes:
- IHD, coronary heart disease;
- Infections leading to destructive changes in the heart muscle;
- Endocrine diseases;
- Arterial hypertension;
- Shifts in metabolism and accumulation of substances;
- Electrolyte balance;
- In connective fibers;
- Amyloidosis;
- Neuromuscular pathology;
- Severe poisoning;
- During pregnancy.
Coronary heart disease is distinguished by a number of characteristic symptoms. Against the background of atherosclerosis, the lumen of the coronary arteries narrows, and a lack of oxygen (O2) occurs in the myocardium. This leads to the destruction of cardiomyocytes and replacement with connective fibers.
Myocardial infections also cause disorders in the heart muscle, inflammatory processes, edema, and damage to cardiomyocytes. Acute myocarditis develops, with the replacement of cardiac fibers by connective tissue, resulting in cardiomyopathy.
Endocrine diseases and hormonal disorders disrupt the functioning of the heart as a result of the influence of hormones and hyperstimulation of functions. These complications can cause:
- Thyroid dysfunction;
- Adrenal diseases;
- Diabetes.
Arterial hypertension with a sustained increase in blood pressure is also included in the list, leading to a pathogenic effect on the myocardium. Under these conditions, the load on the heart significantly increases, as a result, the structure of the cardiac fibers is disrupted, with loss of elasticity and the development of cardiomyopathy.
Shifts in metabolism lead to the accumulation of substances that are foreign to the myocardium and cause irreversible effects on the functioning of the heart muscle. Among the main reasons:
- Pathologies of glycogen accumulation;
- Phytanic acid in Refsum syndrome, genetic origin;
- Sphingolipids in Farbi's disease, with a genetic nature;
- Hemochromatosis with accumulation of iron in the fibers.
Problems with maintaining electrolyte balance are accompanied by changes in the amount of ions in the blood, which affects the functioning of the heart and the structure of myocardial fibers. Potassium, phosphorus, chlorine, magnesium, and calcium ions are washed out during severe diarrhea and various kidney diseases.
Pathological processes of connective tissue in the heart area cause systemic damage and disrupt the structure of myocardial fibers. Inflammation of these fibers leads to cardiosclerosis and gradual replacement of the heart muscle with connective tissue with the development of cardiomyopathy.
The list of diseases that provoke the pathological process includes:
- Scleroderma;
- Dermatomyositis;
- Lupus erythematosus;
- Rheumatoid arthritis.
Amyloidosis is characterized by the deposition of amyloid and causes disruption of the heart muscle. Moreover, the accumulation of this complex of proteins and polysaccharides occurs directly in the myocardium, which leads to the development of pathology.
Neuromuscular pathology causes disturbances in the transmission of impulses by nerve fibers with subsequent deviations in the functioning of the myocardium. In this case, asystole or extrasystole is observed, with a pronounced failure in the contraction of the heart muscle. In particularly severe conditions, the muscle tone of the heart decreases sharply. This leads to the development of a severe form of cardiomyopathy.
Poisoning with poisons, alcohol, surrogates, toxins directly affects the functioning of the heart and causes emergency conditions incompatible with human life. Toxic compounds directly affect the damage of cardiomyocytes, while the passage of the nerve impulse is blocked, and acute heart failure develops.
Severe poisoning with the development of cardiomyopathy is caused by various substances :
- Alcohol products and surrogates;
- Medicines, drugs (amphetamines group and others);
- Toxic compounds, heavy metals, including arsenic, lead, mercury and others.
Chronic consumption of these products causes irreversible changes in the heart muscle, pain in the heart area, and myocardial infarction. The high risk of developing emergency conditions leads to the fact that a person is constantly on the verge of life and death.
Radiation activity directly affects the human body and also refers to damaging factors that cause disturbances in the functioning of the heart. In some cases, such as in pregnant women, problems with the myocardium are temporary. But with chronic alcoholism, drug addiction, and the use of chemical substances, the disease continues to progress and the patient cannot be cured.
Reversible conditions include cardiomyopathy in pregnant women . It occurs more often in the last trimester or after childbirth due to stress. During this period, hemodynamics change dramatically, the circulatory system adapts to provide adequate nutrition to the fetus. At the same time, the volume of circulating blood changes, the level of blood pressure increases or decreases. These changes lead to the development of a reversible form of the disease.
Treatment of cardiomyopathy is prescribed by a doctor in accordance with the indications and depends on the cause of the disease. If the source of severe pathology cannot be determined, the disease is classified as a primary form and a course of maintenance therapy is prescribed.
Rate this article
Article rating 4.45 out of 5. Votes: 11.
Latest articles
Sexual transmission of infections
Sexually transmitted infections or STIs are dangerous diseases that can undermine health and lead to dire consequences. Most of the diseases in this group are…
Hormonal disorders
A woman’s well-being largely depends on the endocrine system. Any hormonal imbalance can cause a sharp deterioration in health, weakening the immune system...
Cervical dysplasia
Cervical intraepithelial neoplasia or cervical dysplasia is a precancerous condition expressed by pathological changes in cells. In most...