Decoding an ECG is the job of a knowledgeable doctor. This method of functional diagnostics evaluates:
- heart rate - the state of the generators of electrical impulses and the state of the heart system conducting these impulses
- the condition of the heart muscle itself (myocardium), the presence or absence of its inflammation, damage, thickening, oxygen starvation, electrolyte imbalance
However, modern patients often have access to their medical documents, in particular, to electrocardiography films on which medical reports are written. With their diversity, these recordings can drive even the most balanced but ignorant person to panic disorder. After all, the patient often does not know for certain how dangerous to life and health is what is written on the back of the ECG film by the hand of a functional diagnostician, and there are still several days before an appointment with a therapist or cardiologist.
To reduce the intensity of passions, we immediately warn readers that with not a single serious diagnosis (myocardial infarction, acute rhythm disturbances), a functional diagnostician will not let a patient leave the office, but, at a minimum, will send him for a consultation with a fellow specialist right there. About the rest of the “open secrets” in this article. In all unclear cases of pathological changes in the ECG, ECG monitoring, 24-hour monitoring (Holter), ECHO cardioscopy (ultrasound of the heart) and stress tests (treadmill, bicycle ergometry) are prescribed.
Numbers and Latin letters in ECG interpretation
- When describing an ECG, the heart rate (HR) is usually indicated. The norm is from 60 to 90 (for adults), for children (see table)
- The following are the various intervals and teeth with Latin designations. (ECG with interpretation, see Fig.)
PQ- (0.12-0.2 s) – atrioventricular conduction time. Most often it lengthens against the background of AV blockade. Shortened in CLC and WPW syndromes.
P – (0.1s) height 0.25-2.5 mm describes atrial contractions. May indicate their hypertrophy.
QRS – (0.06-0.1s) -ventricular complex
QT – (no more than 0.45 s) lengthens with oxygen starvation (myocardial ischemia, infarction) and the threat of rhythm disturbances.
RR - the distance between the apices of the ventricular complexes reflects the regularity of heart contractions and makes it possible to calculate heart rate.
The interpretation of the ECG in children is presented in Fig. 3
Heart Rate Description Options
Sinus rhythm
This is the most common inscription found on an ECG. And, if nothing else is added and the frequency (HR) is indicated from 60 to 90 beats per minute (for example, HR 68`) - this is the best option, indicating that the heart works like a clock. This is the rhythm set by the sinus node (the main pacemaker that generates electrical impulses that cause the heart to contract). At the same time, sinus rhythm implies well-being, both in the state of this node and the health of the conduction system of the heart. The absence of other records denies pathological changes in the heart muscle and means that the ECG is normal. In addition to sinus rhythm, there may be atrial, atrioventricular or ventricular, indicating that the rhythm is set by cells in these parts of the heart and is considered pathological.
Sinus arrhythmia
This is a normal variant in young people and children. This is a rhythm in which impulses leave the sinus node, but the intervals between heart contractions are different. This may be due to physiological changes (respiratory arrhythmia, when heart contractions slow down during exhalation). Approximately 30% of sinus arrhythmias require observation by a cardiologist, as they are at risk of developing more serious rhythm disturbances. These are arrhythmias after rheumatic fever. Against the background of myocarditis or after it, against the background of infectious diseases, heart defects and in persons with a family history of arrhythmias.
Sinus bradycardia
These are rhythmic contractions of the heart with a frequency of less than 50 per minute. In healthy people, bradycardia occurs, for example, during sleep. Bradycardia also often occurs in professional athletes. Pathological bradycardia may indicate sick sinus syndrome. In this case, bradycardia is more pronounced (heart rate from 45 to 35 beats per minute on average) and is observed at any time of the day. When bradycardia causes pauses in heart contractions of up to 3 seconds during the day and about 5 seconds at night, leads to disturbances in the supply of oxygen to tissues and is manifested, for example, by fainting, an operation is indicated to install a cardiac pacemaker, which replaces the sinus node, imposing a normal rhythm of contractions on the heart.
Sinus tachycardia
Heart rate more than 90 per minute is divided into physiological and pathological. In healthy people, sinus tachycardia is accompanied by physical and emotional stress, drinking coffee, sometimes strong tea or alcohol (especially energy drinks). It is short-lived and after an episode of tachycardia, the heart rate returns to normal within a short period of time after stopping the load. With pathological tachycardia, heartbeats bother the patient at rest. Its causes are fever, infections, blood loss, dehydration, thyrotoxicosis, anemia, cardiomyopathy. The underlying disease is treated. Sinus tachycardia is stopped only in case of a heart attack or acute coronary syndrome.
Extarsystole
These are rhythm disturbances in which foci outside the sinus rhythm give extraordinary cardiac contractions, after which there is a pause of twice the length, called compensatory. In general, the patient perceives heartbeats as uneven, rapid or slow, and sometimes chaotic. The most worrying thing is the dips in heart rate. There may be unpleasant sensations in the chest in the form of tremors, tingling, feelings of fear and emptiness in the stomach.
Not all extrasystoles are dangerous to health. Most of them do not lead to significant circulatory disorders and do not threaten either life or health. They can be functional (against the background of panic attacks, cardioneurosis, hormonal imbalances), organic (with ischemic heart disease, heart defects, myocardial dystrophy or cardiopathy, myocarditis). Intoxication and heart surgery can also lead to them. Depending on the place of occurrence, extrasystoles are divided into atrial, ventricular and anthrioventricular (arising in the node at the border between the atria and ventricles).
- Single extrasystoles are most often rare (less than 5 per hour). They are usually functional and do not interfere with normal blood supply.
- Paired extrasystoles, two at a time, accompany a certain number of normal contractions. Such rhythm disturbances often indicate pathology and require further examination (Holter monitoring).
- Allorhythmias are more complex types of extrasystoles. If every second contraction is an extrasystole, this is bigymenia, if every third contraction is trigymenia, every fourth is quadrigymenia.
It is customary to divide ventricular extrasystoles into five classes (according to Lown). They are assessed during daily ECG monitoring, since the readings of a regular ECG in a few minutes may not show anything.
- Class 1 - single rare extrasystoles with a frequency of up to 60 per hour, emanating from one focus (monotopic)
- 2 – frequent monotopic more than 5 per minute
- 3 – frequent polymorphic (of different shapes) polytopic (from different foci)
- 4a – paired, 4b – group (trigymenia), episodes of paroxysmal tachycardia
- 5 – early extrasystoles
The higher the class, the more serious the violations, although today even classes 3 and 4 do not always require drug treatment. In general, if there are less than 200 ventricular extrasystoles per day, they should be classified as functional and not worry about them. For more frequent cases, ECHO CS is indicated, and sometimes cardiac MRI is indicated. It is not the extrasystole that is treated, but the disease that leads to it.
Paroxysmal tachycardia
In general, a paroxysm is an attack. A paroxysmal increase in rhythm can last from several minutes to several days. In this case, the intervals between heart contractions will be the same, and the rhythm will increase over 100 per minute (on average from 120 to 250). There are supraventricular and ventricular forms of tachycardia. This pathology is based on abnormal circulation of electrical impulses in the conduction system of the heart. This pathology can be treated. Home remedies to relieve an attack:
- holding your breath
- increased forced cough
- immersing face in cold water
WPW syndrome
Wolff-Parkinson-White syndrome is a type of paroxysmal supraventricular tachycardia. Named after the authors who described it. The appearance of tachycardia is based on the presence of an additional nerve bundle between the atria and ventricles, through which a faster impulse passes than from the main pacemaker.
As a result, an extraordinary contraction of the heart muscle occurs. The syndrome requires conservative or surgical treatment (in case of ineffectiveness or intolerance of antiarrhythmic tablets, during episodes of atrial fibrillation, and with concomitant heart defects).
CLC – syndrome (Clerk-Levi-Christesco)
is similar in mechanism to WPW and is characterized by earlier excitation of the ventricles than normal due to an additional bundle along which the nerve impulse travels. The congenital syndrome is manifested by attacks of rapid heartbeat.
Atrial fibrillation
It can be in the form of an attack or a permanent form. It manifests itself in the form of atrial flutter or fibrillation.
Atrial fibrillation
Atrial fibrillation
When flickering, the heart contracts completely irregularly (the intervals between contractions of very different durations). This is explained by the fact that the rhythm is not set by the sinus node, but by other cells of the atria.
The resulting frequency is from 350 to 700 beats per minute. There is simply no full contraction of the atria; contracting muscle fibers do not effectively fill the ventricles with blood.
As a result, the heart’s output of blood deteriorates and organs and tissues suffer from oxygen starvation. Another name for atrial fibrillation is atrial fibrillation. Not all atrial contractions reach the ventricles of the heart, so the heart rate (and pulse) will be either below normal (bradysystole with a frequency of less than 60), or normal (normosystole from 60 to 90), or above normal (tachysystole more than 90 beats per minute ).
An attack of atrial fibrillation is difficult to miss.
- It usually starts with a strong beat of the heart.
- It develops as a series of absolutely irregular heartbeats with a high or normal frequency.
- The condition is accompanied by weakness, sweating, dizziness.
- The fear of death is very pronounced.
- There may be shortness of breath, general agitation.
- Sometimes there is loss of consciousness.
- The attack ends with normalization of the rhythm and the urge to urinate, during which a large amount of urine is released.
To stop an attack, they use reflex methods, drugs in the form of tablets or injections, or resort to cardioversion (stimulating the heart with an electric defibrillator). If an attack of atrial fibrillation is not eliminated within two days, the risks of thrombotic complications (pulmonary embolism, stroke) increase.
With a constant form of heartbeat flicker (when the rhythm is not restored either against the background of drugs or against the background of electrical stimulation of the heart), they become a more familiar companion to patients and are felt only during tachysystole (rapid, irregular heartbeats). The main task when detecting signs of tachysystole of a permanent form of atrial fibrillation on the ECG is to slow down the rhythm to normosystole without trying to make it rhythmic.
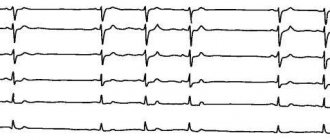
Examples of recordings on ECG films:
- atrial fibrillation, tachysystolic variant, heart rate 160 b'.
- Atrial fibrillation, normosystolic variant, heart rate 64 b'.
Atrial fibrillation can develop in the course of coronary heart disease, against the background of thyrotoxicosis, organic heart defects, diabetes mellitus, sick sinus syndrome, and intoxication (most often with alcohol).
Atrial flutter
These are frequent (more than 200 per minute) regular contractions of the atria and equally regular, but less frequent contractions of the ventricles. In general, flutter is more common in the acute form and is better tolerated than flicker, since circulatory disorders are less pronounced. Fluttering develops when:
- organic heart diseases (cardiomyopathies, heart failure)
- after heart surgery
- against the background of obstructive pulmonary diseases
- in healthy people it almost never occurs
Clinically, flutter is manifested by rapid rhythmic heartbeat and pulse, swelling of the neck veins, shortness of breath, sweating and weakness.
Frequency and rhythm of contractions
In medicine, disturbances in the rhythm of heart contractions are called arrhythmia, and percentages are used to measure instability of rhythm. If the speed and distance between the teeth on the cardiogram exceeds 15%, this indicates an abnormal rhythm or sinus arrhythmia. The state of arrhythmia with sinus rhythm is the norm for children in adolescence and students, but often this indicates that a pathological process has begun.
A common arrhythmia is untimely depolarization, which causes unscheduled contractions. Healthy women and men are also susceptible to normal single extrasystoles, but if they appear very often on the electrocardiogram, this indicates systolic inflammation of the heart muscle, coronary artery disease or heart disease.
Heart rate is a clear and simple characteristic that allows you to determine the number of contractions in 60 seconds. The number of heartbeats may deviate from the norm and indicate diseases:
- above normal - tachycardia;
- below normal - bradycardia.
In adults, the number of heartbeats in a normal ECG should range from 65 to 85 beats. It is worth noting that “normal” is a relative concept, and phenomena such as tachycardia and bradycardia can be observed even in healthy people. For example, tachycardia occurs during stressful situations or after intense physical activity, and bradycardia occurs during sleep.
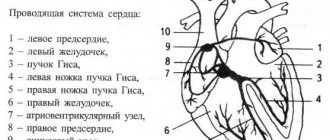
Conduction disorders
Normally, having formed in the sinus node, electrical excitation travels through the conduction system, experiencing a physiological delay of a split second in the atrioventricular node. On its way, the impulse stimulates the atria and ventricles, which pump blood, to contract. If in any part of the conduction system the impulse is delayed longer than the prescribed time, then excitation to the underlying sections will come later, and, therefore, the normal pumping work of the heart muscle will be disrupted. Conduction disturbances are called blockades. They can occur as functional disorders, but more often they are the result of drug or alcohol intoxication and organic heart disease. Depending on the level at which they arise, several types are distinguished.
Sinoatrial blockade
When the exit of an impulse from the sinus node is difficult. In essence, this leads to sick sinus syndrome, slowing of contractions to severe bradycardia, impaired blood supply to the periphery, shortness of breath, weakness, dizziness and loss of consciousness. The second degree of this blockade is called Samoilov-Wenckebach syndrome.
Atrioventricular block (AV block)
This is a delay of excitation in the atrioventricular node longer than the prescribed 0.09 seconds. There are three degrees of this type of blockade. The higher the degree, the less often the ventricles contract, the more severe the circulatory disorders.
- In the first, the delay allows each atrial contraction to maintain an adequate number of ventricular contractions.
- The second degree leaves some of the atrial contractions without ventricular contractions. It is described, depending on the prolongation of the PQ interval and the loss of ventricular complexes, as Mobitz 1, 2 or 3.
- The third degree is also called complete transverse blockade. The atria and ventricles begin to contract without interconnection.
In this case, the ventricles do not stop because they obey the pacemakers from the underlying parts of the heart. If the first degree of blockade may not manifest itself in any way and can be detected only with an ECG, then the second is already characterized by sensations of periodic cardiac arrest, weakness, and fatigue. With complete blockades, brain symptoms are added to the manifestations (dizziness, spots in the eyes). Morgagni-Adams-Stokes attacks may develop (when the ventricles escape from all pacemakers) with loss of consciousness and even convulsions.
Impaired conduction within the ventricles
In the ventricles, the electrical signal propagates to the muscle cells through such elements of the conduction system as the trunk of the His bundle, its legs (left and right) and branches of the legs. Blockades can occur at any of these levels, which is also reflected in the ECG. In this case, instead of being simultaneously covered by excitation, one of the ventricles is delayed, since the signal to it bypasses the blocked area.
In addition to the place of origin, a distinction is made between complete or incomplete blockade, as well as permanent and non-permanent blockade. The causes of intraventricular blocks are similar to other conduction disorders (ischemic heart disease, myocarditis and endocarditis, cardiomyopathies, heart defects, arterial hypertension, fibrosis, heart tumors). Also affected are the use of antiarthmic drugs, an increase in potassium in the blood plasma, acidosis, and oxygen starvation.
- The most common is blockade of the anterosuperior branch of the left bundle branch (ALBBB).
- In second place is right leg block (RBBB). This blockade is usually not accompanied by heart disease.
- Left bundle branch block is more typical for myocardial lesions. In this case, complete blockade (PBBB) is worse than incomplete blockade (LBBB). It sometimes has to be distinguished from WPW syndrome.
- Blockade of the posteroinferior branch of the left bundle branch can occur in individuals with a narrow and elongated or deformed chest. Among pathological conditions, it is more typical for overload of the right ventricle (with pulmonary embolism or heart defects).
The clinical picture of blockades at the levels of the His bundle is not expressed. The picture of the underlying cardiac pathology comes first.
- Bailey's syndrome is a two-bundle block (of the right bundle branch and the posterior branch of the left bundle branch).
How to decipher a cardiogram of the heart?
A strict plan for deciphering an ECG consists of analyzing the resulting graph. In practice, only the total vector of the QRS complex is used. The work of the heart muscle is presented in the form of a continuous line with marks and alphanumeric designations. Any person can decipher an ECG with certain training, but only a doctor can make the correct diagnosis. ECG analysis requires knowledge of algebra, geometry and an understanding of letter symbols.
Not only cardiologists, but also general practitioners (for example, paramedics) have to read ECGs and make conclusions. Timely interpretation of the ECG makes it possible to provide effective first aid to victims.
ECG indicators that need to be taken into account when interpreting the results:
- intervals;
- segments;
- teeth.
There are strict indicators of normality on the ECG, and any deviation is already a sign of disturbances in the functioning of the heart muscle. Pathology can only be excluded by a qualified specialist - a cardiologist.
ECG interpretation in adults - the norm in the table
Myocardial hypertrophy
With chronic overload (pressure, volume), the heart muscle in certain areas begins to thicken, and the chambers of the heart begin to stretch. On the ECG, such changes are usually described as hypertrophy.
- Left ventricular hypertrophy (LVH) is typical for arterial hypertension, cardiomyopathy, and a number of heart defects. But even normally, athletes, obese patients and people engaged in heavy physical labor may experience signs of LVH.
- Right ventricular hypertrophy is an undoubted sign of increased pressure in the pulmonary blood flow system. Chronic cor pulmonale, obstructive pulmonary diseases, cardiac defects (pulmonary stenosis, tetralogy of Fallot, ventricular septal defect) lead to RVH.
- Left atrial hypertrophy (LAH) – with mitral and aortic stenosis or insufficiency, hypertension, cardiomyopathy, after myocarditis.
- Right atrial hypertrophy (RAH) – with cor pulmonale, tricuspid valve defects, chest deformities, pulmonary pathologies and PE.
- Indirect signs of ventricular hypertrophy are deviation of the electrical axis of the heart (EOC) to the right or left. The left type of EOS is its deviation to the left, that is, LVH, the right type is RVH.
- Systolic overload is also evidence of hypertrophy of the heart. Less commonly, this is evidence of ischemia (in the presence of angina pain).
Changes in myocardial contractility and nutrition
Early ventricular repolarization syndrome
Most often, this is a variant of the norm, especially for athletes and people with congenital high body weight. Sometimes associated with myocardial hypertrophy. Refers to the peculiarities of the passage of electrolytes (potassium) through the membranes of cardiocytes and the characteristics of the proteins from which the membranes are built. It is considered a risk factor for sudden cardiac arrest, but does not provide clinical results and most often remains without consequences.
Moderate or severe diffuse changes in the myocardium
This is evidence of a malnutrition of the myocardium as a result of dystrophy, inflammation (myocarditis) or cardiosclerosis. Also, reversible diffuse changes accompany disturbances in water and electrolyte balance (with vomiting or diarrhea), taking medications (diuretics), and heavy physical activity.
Nonspecific ST changes
This is a sign of deterioration in myocardial nutrition without severe oxygen starvation, for example, in case of disturbances in the balance of electrolytes or against the background of dyshormonal conditions.
Acute ischemia, ischemic changes, T wave changes, ST depression, low T
This describes reversible changes associated with oxygen starvation of the myocardium (ischemia). This can be either stable angina or unstable, acute coronary syndrome. In addition to the presence of the changes themselves, their location is also described (for example, subendocardial ischemia). A distinctive feature of such changes is their reversibility. In any case, such changes require comparison of this ECG with old films, and if a heart attack is suspected, troponin rapid tests for myocardial damage or coronary angiography. Depending on the type of coronary heart disease, anti-ischemic treatment is selected.
Indications for an ECG
In clinical practice, there are several indications for electrocardiography:
- severe chest pain;
- constant fainting;
- dyspnea;
- exercise intolerance;
- dizziness;
- heart murmurs.
During a routine examination, an ECG is a mandatory diagnostic method. There may be other indications determined by the attending physician. If you experience any other alarming symptoms, consult your doctor immediately to determine their cause.