The study of the health of a person with cardiovascular diseases needs to determine “reserves” and functional capabilities. Such characteristics are especially important in the selection of treatment tactics for severe cases, cardiogenic and toxic shock, and in preparation for cardiac surgery.
The cardiac index is not measured by any device. It belongs to the group of calculated indicators. This means that to determine it it is necessary to know other quantities.
How to calculate cardiac index
In the clinical literature, the concept of “ minute volume of blood circulation
” (
MVC
) is more often used.
In the oxygen transport system, the circulatory apparatus
is a limiting link, therefore the ratio of the maximum value of IOC, manifested during maximally intense muscular work, with its value under basal metabolic conditions gives an idea of the functional reserve of the cardiovascular system. The same ratio also reflects the functional reserve of the heart in its hemodynamic function. The hemodynamic functional reserve of the heart in healthy people is 300-400%. This means that resting IOC can be increased by 3-4 times. In physically trained individuals, the functional reserve is higher - it reaches 500-700%.
For conditions of physical rest and horizontal position of the subject's body, the normal values of minute volume of blood circulation (MCV)
correspond to the range of 4-6 l/min (values of 5-5.5 l/min are more often given). The average values of the cardiac index range from 2 to 4 l/(min • m2) - values of the order of 3-3.5 l/(min • m2) are more often given.
Rice.
9.4. Left ventricular diastolic capacity fractions. Since the blood volume in humans is only 5-6 liters, a complete circulation of the entire blood volume occurs in approximately 1 minute. During periods of heavy work, the IOC in a healthy person can increase to 25-30 l/min, and in athletes - up to 30-40 l/min.
Factors determining the value of minute volume of blood circulation (MCV)
, are systolic blood volume, heart rate and venous return of blood to the heart.
Systolic blood volume
. The volume of blood pumped by each ventricle into the main vessel (aorta or pulmonary artery) during one contraction of the heart is referred to as systolic, or stroke, blood volume.
Resting blood volume
, ejected from the ventricle, normally constitutes from a third to a half of the total amount of blood contained in this chamber of the heart at the end of diastole.
The reserve volume of blood
remaining in the heart after systole is a kind of depot, providing an increase in cardiac output in situations in which rapid intensification of hemodynamics is required (for example, during physical activity, emotional stress, etc.).
Table 9.3. Some parameters of systemic hemodynamics and pumping function of the heart in humans (under basal metabolic conditions)
The value of systolic (stroke) blood volume
is largely determined by the end-diastolic volume of the ventricles. Under resting conditions, the diastolic capacity of the ventricles of the heart is divided into three fractions: stroke volume, basal reserve volume and residual volume. All these three fractions together make up the end-diastolic volume of blood contained in the ventricles (Fig. 9.4).
After ejection of systolic blood volume
The volume of blood remaining in the ventricle is the end-systolic volume.
It is divided into basal reserve volume and residual volume. Basal reserve volume is the amount of blood that can be additionally ejected from the ventricle when the force of myocardial contractions increases (for example, during physical activity of the body). Residual volume
is the amount of blood that cannot be pushed out of the ventricle even with the most powerful heart contraction (see Fig. 9.4).
The amount of reserve blood volume
is one of the main determinants of the functional reserve of the heart for its specific function - the movement of blood in the system. As the reserve volume increases, the maximum systolic volume that can be ejected from the heart under conditions of intense activity increases accordingly.
Regulatory influences on the heart are realized in changes in systolic volume
by influencing the contractile force of the myocardium. As the power of cardiac contraction decreases, systolic volume decreases.
In a person with a horizontal body position under resting conditions, the systolic volume
ranges from 60 to 90 ml (Table 9.3).
Source
Features of the indicator assessment
The cardiac index allows you to choose the right treatment at different stages of shock and obtain more accurate diagnostic information.
It is important to keep in mind that this indicator is never self-assessed. It is included in the group of hemodynamic quantities as equivalent information together with:
- pressure in the arteries, veins, chambers of the heart;
- saturation of blood with oxygen;
- shock indices of the work of each ventricle;
- indicator of peripheral resistance;
- coefficients of oxygen delivery and utilization.
Interpretation of ultrasound (EchoCG) of the heart
Among diagnostic cardiac procedures that are informative, it is worth highlighting echocardiography or ultrasound examination of the heart. This is a hardware procedure performed using high-frequency sound waves. It is indispensable for accurately identifying problems that are directly related to the work of the myocardium and the entire cardiovascular system.
The effectiveness of echocardiography is directly related to the evaluation of its results. Competent interpretation of cardiac ultrasound is a direct path to a speedy diagnosis and drawing up an effective treatment plan. Entrust the solution to the problem to an experienced specialist, contact us for qualified medical support!
Why is cardiac echocardiography needed?
There are a myriad of reasons why a doctor might recommend an echocardiogram. A harmless and inexpensive procedure is indispensable for:
The attending doctor can prescribe a procedure, and then conduct a full interpretation of the ultrasound of the heart, in case of constant dizziness, arrhythmia, atherosclerosis, pericarditis, heart muscle defects, coronary artery disease. Indications are often multiple pregnancy, hereditary predisposition, medical examination at the enterprise.
Ultrasound cardiography is performed for both adults and children. When a baby is suspected of having abnormalities in myocardial development, shortness of breath appears without symptoms of an acute respiratory infection, loss of consciousness is observed, it is imperative to check the functioning of the main organ. The pediatrician can refer for diagnostics when, during the use of a phonendoscope, extraneous sounds were noticed against the background of normal contractile activity.
The above-mentioned cardiac examination also plays an important role for a teenager. The test is aimed at assessing the normal development of the organ during puberty, because it is at this time that a sharp increase in body size is often observed.
Reasons for decreased qi
The factor is always cardiac.
- Heart failure. The main pathological process that ends with a decrease in myocardial contractility, a small volume of blood ejection into the systemic circle and disruption of the functioning of all organs and systems. Poses the greatest danger. Develops as a result of a long course of arterial hypertension or a heart attack.
Read more about the symptoms of acute heart failure in this article.
- Cardiomyopathy. Growth, thickening of the walls of the muscular organ, expansion of the chambers always causes the circadian rhythm to decrease. Recovery as such is impossible. This is an anatomical phenomenon, it exists constantly. On the other hand, there is a chance of compensation through medication, then the circadian index will return to normal.
- Inflammation of the heart muscle (myocarditis, pericarditis). Autoimmune or infectious origin, when the pathology goes far in its development. It manifests itself as bradycardia, which is not typical for this diagnosis. This is a terrible sign. Urgent treatment is required. Although it needs to start even earlier, as soon as the process has begun.
A drop in CI may be the result of taking antiarrhythmic drugs. Then you need to wait a while and do the research again.
Interpretation of ultrasound of the heart
In order for the interpretation of cardiac echocardiography to be carried out without errors and completely, the patient’s age, general state of health, and the presence of chronic diseases (pancreatitis, tonsillitis, asthma, vasculitis, etc.) are taken into account. It is impossible to determine the pathology on your own (without knowledge and experience). Only a doctor can correctly assess the answer. There is no place for experiments and guesswork. It is inappropriate to look for answers on the Internet on the websites of companies with a dubious reputation. Trust your health to professionals who provide guarantees and value each patient.
Reasons for increasing QI
They are relatively rarely pathological. More often, a deviation in the circadian index indicates that the body is highly trained.
The violation (relatively speaking) is inherent in professional athletes and representatives of physical labor. In this case, recovery is not required, but the patient must be monitored.
You never know how your heart will behave next. Fatal consequences as a result of decompensation of the condition are quite possible.
Also, the cause of increased CI is an increase in pressure in the pulmonary artery and the accompanying dysfunction of the organ, anatomical defects, the so-called cor pulmonale.
Interpretation of EchoCG results in adults
The diagnostic conclusion is made only by the attending physician. The document in written (sometimes electronic) form is transferred to the patient in the diagnostic room, after which it is recorded in the hospital record. The individual indicators of the person undergoing the examination are entered into a special table, which already contains the normal figures for a specific age and gender.
Trying to decipher an ultrasound of the heart on your own is stupid and unsafe. The combination of several deviations may indicate different pathologies. You can’t do without experience and knowledge here.
| Cardiac parameter | Men's answers | Women's answers |
| LVMM—left ventricular myocardial mass | 135-180 g | 95-142 g |
| LVMI—left ventricular mass index | 71-92 g/m2 | 71-88 g/m2 |
| ESD – LV end-systolic size | 31-42 mm | 31-42 mm |
| ESD – LV end-systolic size | 31-42 mm | 31-42 mm |
| EDV - end diastolic size | 46-58 mm | 45-58 mm |
| Volume of fluid in the pericardial cavity | 10-30 ml | 10-30 ml |
| LV wall thickness in diastole | up to 11 mm | up to 10 mm |
| Blood ejection volume during LV systole | 60-100 ml | 60-100 ml |
| Wall thickness of the RV - right ventricle | 5 mm | 4.8-5 mm |
| LA size - left atrium | 18.5-33 mm | 17.5-33 mm |
| LA end-diastolic volume | 50-82 ml | 38-57 ml |
| End-diastolic volume of the RA – right atrium | 20-100 ml | 20-100 ml |
| Thickness of the IVS - interventricular septum in systole | 5-9.5 mm | 5-9.0 mm |
| IVS thickness in diastole | 7.5-11 mm | 7.5-11 mm |
| Aortic opening area | 20-35 mm2 | 20-35 mm2 |
| Thickness of the outer membrane of the pericardium | 1.2-1.7 mm | 1.2-1.7 mm |
Only a cardiologist can evaluate an ultrasound of the heart; the results are interpreted according to standard values, taking into account the general health of the patient, the medications he is taking and other factors. The size, weight, volume and location of the organ, the condition of the valves and tissues are studied. Parameters for contractions, blood vessels and blood flow, wall thickness and other important nuances are recorded. The speed of blood distribution through the chambers of the heart helps to determine Doppler measurements. It is often performed in conjunction with traditional ultrasound examination.
Cardiac output, its fractions. Systolic and minute blood volumes. Cardiac index.
The amount of blood ejected by the ventricle of the heart into the arteries per minute is an important indicator of the functional state of the cardiovascular system (CVS) and is called minute blood volume (MBV). It is the same for both ventricles and at rest is 4.5–5 liters.
An important characteristic of the pumping function of the heart is the stroke volume, also called systolic volume or systolic ejection. Stroke volume is the amount of blood ejected by the ventricle of the heart into the arterial system in one systole. (If you divide the IOC by the heart rate per minute, we get the systolic volume (SV) of blood flow.) With a heart contraction of 75 beats per minute, it is 65–70 ml; during work it increases to 125 ml. In athletes at rest it is 100 ml, during work it increases to 180 ml. The determination of MOC and CO is widely used in the clinic.
Ejection fraction (EF) is the percentage ratio of the stroke volume of the heart to the end-diastolic volume of the ventricle. EF at rest in a healthy person is 50-75%, and during physical activity it can reach 80%.
The volume of blood in the ventricular cavity that it occupies before its systole is the end-diastolic volume (120–130 ml).
End-systolic volume (ESV) is the amount of blood remaining in the ventricle immediately after systole. At rest, it is less than 50% of the EDV, or 50-60 ml. Part of this blood volume is reserve volume.
The reserve volume is realized when CO increases under load. Normally, it is 15–20% of the end-diastolic value.
The volume of blood in the cavities of the heart remaining when the reserve volume is fully realized at maximum systole constitutes the residual volume. CO and IOC values are not constant. During muscular activity, IOC increases to 30–38 l due to increased heart rate and increased CO2.
A number of indicators are used to assess the contractility of the heart muscle. These include: ejection fraction, rate of blood expulsion during the rapid filling phase, rate of increase in pressure in the ventricle during the period of stress (measured by probing the ventricle)/
The rate of blood expulsion is changed using Doppler ultrasound of the heart.
The rate of increase in pressure in the cavities of the ventricles is considered one of the most reliable indicators of myocardial contractility. For the left ventricle, the normal value of this indicator is 2000-2500 mmHg/s.
A decrease in the ejection fraction below 50%, a decrease in the rate of blood expulsion, and the rate of pressure increase indicate a decrease in myocardial contractility and the possibility of developing insufficiency of the pumping function of the heart.
The value of the IOC divided by the body surface area in m2 is determined as the cardiac index (l/min/m2).
SI = MOK/S (l/min×m2)
It is an indicator of the pumping function of the heart. Normally, the cardiac index is 3–4 l/min×m2.
IOC, SV and CI are united by the common concept of cardiac output.
If the IOC and blood pressure in the aorta (or pulmonary artery) are known, the external work of the heart can be determined
P = IOC × BP
P is the work of the heart in minutes in kilograms (kg/m).
MOC—minute blood volume (l).
Blood pressure is pressure in meters of water column.
At physical rest, the external work of the heart is 70–110 J; during work it increases to 800 J, for each ventricle separately.
Thus, the work of the heart is determined by 2 factors:
1. The amount of blood flowing to it.
2. Vascular resistance during the expulsion of blood into the arteries (aorta and pulmonary artery). When the heart cannot pump all the blood into the arteries at a given vascular resistance, heart failure occurs.
There are 3 types of heart failure:
1. Insufficiency from overload, when excessive demands are placed on the heart with normal contractility due to defects, hypertension.
2. Heart failure due to myocardial damage: infections, intoxications, vitamin deficiencies, impaired coronary circulation. At the same time, the contractile function of the heart decreases.
3. Mixed form of failure - with rheumatism, dystrophic changes in the myocardium, etc.
The entire complex of manifestations of heart activity is recorded using various physiological techniques - cardiography: ECG, electrokymography, ballistocardiography, dynamocardiography, apical cardiography, ultrasound cardiography, etc.
The diagnostic method for the clinic is the electrical recording of the movement of the contour of the heart shadow on the screen of the X-ray machine. A photocell connected to an oscilloscope is applied to the screen at the edges of the heart contour. As the heart moves, the illumination of the photocell changes. This is recorded by an oscilloscope in the form of a curve of contraction and relaxation of the heart. This technique is called electrokymography.
The apical cardiogram is recorded by any system that detects small local movements. The sensor is fixed in the 5th intercostal space above the site of the cardiac impulse. Characterizes all phases of the cardiac cycle. But it is not always possible to register all phases: the cardiac impulse is projected differently, and part of the force is applied to the ribs. The recording may differ from person to person and from one person to another, depending on the degree of development of the fat layer, etc.
The clinic also uses research methods based on the use of ultrasound - ultrasound cardiography.
Ultrasonic vibrations at a frequency of 500 kHz and higher penetrate deeply through tissues being generated by ultrasound emitters applied to the surface of the chest. Ultrasound is reflected from tissues of various densities - from the outer and inner surface of the heart, from blood vessels, from valves. The time it takes for the reflected ultrasound to reach the capturing device is determined.
If the reflective surface moves, the return time of the ultrasonic vibrations changes. This method can be used to record changes in the configuration of heart structures during its activity in the form of curves recorded from the screen of a cathode ray tube. These techniques are called non-invasive.
Invasive techniques include:
Catheterization of the heart cavities. An elastic catheter probe is inserted into the central end of the opened brachial vein and pushed towards the heart (into its right half). A probe is inserted into the aorta or left ventricle through the brachial artery.
Ultrasound scanning - an ultrasound source is inserted into the heart using a catheter.
Angiography is the study of heart movements in a field of X-rays, etc.
Mechanical and sound manifestations of cardiac activity. Heart sounds, their genesis. Polycardiography. Comparison in time of periods and phases of the cardiac cycle of ECG and FCG and mechanical manifestations of cardiac activity.
Heart beat. During diastole, the heart takes the shape of an ellipsoid. During systole, it takes on the shape of a ball, its longitudinal diameter decreases, and its transverse diameter increases. During systole, the apex rises and presses against the anterior chest wall. A cardiac impulse occurs in the 5th intercostal space, which can be recorded (apical cardiography). The expulsion of blood from the ventricles and its movement through the vessels, due to reactive recoil, causes vibrations of the entire body. The recording of these oscillations is called ballistocardiography. The work of the heart is also accompanied by sound phenomena.
Heart sounds. When listening to the heart, two sounds are detected: the first is systolic, the second is diastolic.
- The systolic tone is low, prolonged (0.12 s). Several overlapping components are involved in its genesis:
1. Mitral valve closure component.
2. Closure of the tricuspid valve.
3. Pulmonary tone of blood expulsion.
4. Aortic tone of blood expulsion.
The characteristic of the first tone is determined by the tension of the leaflet valves, the tension of the tendon threads, papillary muscles, and the walls of the ventricular myocardium.
Components of blood expulsion occur when the walls of the great vessels are tense. The first sound is clearly audible in the 5th left intercostal space. In pathology, the genesis of the first tone involves:
1. Aortic valve opening component.
2. Opening of the pulmonary valve.
3. Tone of pulmonary artery distension.
4. Aortic stretch tone.
Strengthening of the first tone can occur with:
1. Hyperdynamics: physical activity, emotions.
- When there is a violation of the time relationship between the systole of the atria and ventricles.
- With poor filling of the left ventricle (especially with mitral stenosis, when the valves do not open completely). The third option of amplifying the first tone has significant diagnostic value.
Weakening of the first sound is possible with mitral valve insufficiency, when the valves do not close tightly, with myocardial damage, etc.
- II tone - diastolic (high, short 0.08 s). Occurs when the closed semilunar valves are tense. On the sphygmogram its equivalent is incisura. The higher the pressure in the aorta and pulmonary artery, the higher the tone. It can be heard well in the 2nd intercostal space on the right and left of the sternum. It intensifies with sclerosis of the ascending aorta and pulmonary artery. The sound of the 1st and 2nd heart sounds most closely conveys the combination of sounds when pronouncing the phrase “LAB-DAB”.
studfiles.net
Norms of cardiac echocardiography in children
In pediatrics, standard indicators are directly related to the patient’s body area. It can be determined using a formula using the child’s height and weight data. During diagnostics, review and note information on:
Competent interpretation of cardiac echocardiography in children requires care and responsibility in all situations.
| Parameters for diagnosing myocardium in newborns | Male | Female |
| Left ventricular EDR | From 19 to 25 mm | From 18 to 24 mm |
| Left atrium diameter | From 13 to 18 mm | From 12 to 17 mm |
| Left ventricle diameter | From 6 to 14 mm | From 5 to 13 mm |
| Left ventricular ESR | From 12 to 17 mm | |
| MZhP (thickness) | From 3 to 6 mm | |
| Right ventricular wall thickness | From 2 to 3 mm | |
| Blood flow speed | About 1.3 m per second | |
| Ejection fraction varies in infants | From 65 to 75% | |
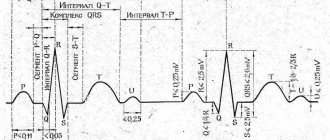
Determination of heart rate (HR) and direction of the electrical axis of the heart
Using the cardiogram data, you can determine the number of heart contractions. To do this, you need to measure the distance between the two highest R waves on the ECG, estimate the speed at which the cardiogram was taken and make calculations.
Horizontal position of the electrical axis of the heart
If the ECG was taken at a speed of 25 mm/s, a coefficient of 0.04 a will be used for calculation; if the speed was 50 m/s, the coefficient will be 0.08.
The number of contractions is calculated using the formula:
Heart rate = 60/distance between teeth R* coefficient
For example, the distance between the teeth on the cardiogram was 15 mm, and the cardiogram was taken at a speed of 25 mm/s.
In this case, the calculation will be like this:
In this case, the number of heart contractions will be 100 beats/min. Since 50–90 beats/min is considered normal, such a patient has slight tachycardia.
To determine the direction of the electrical axis of the heart, it is necessary to evaluate the size of the R wave in standard leads. Normally, it should be largest in lead II. This indicates that the heart is positioned correctly with a slight deviation to the left.
The largest R wave in lead III indicates a deviation of the heart to the right, and in lead I - to the left. In these cases, it is necessary to analyze the cardiogram for hypertrophy of the left or right side of the heart, which most often leads to such processes.
Heart rhythm and arrhythmias
Normally, the heart beats rhythmically, so the cardiogram looks like a repeating pattern. Small deviations are possible - up to 10% from the norm. To understand whether the difference between the intervals fits into 10%, you need to evaluate the ECG fragments by measuring the distances between the RR teeth in cells or using a ruler.
If a significant difference is detected between these intervals, the patient is diagnosed with arrhythmia.
The heart rate should normally be sinus. This is evidenced by the sinus nature of the P wave, which is positive in leads I-II and negative in leads AVR. This wave is also usually positive in lead I, AVF and in precordial leads V3-V6.
In leads V1 and V2 it can be either positive or biphasic (consisting of two small teeth). All these cases are considered a variant of the norm. In other cases, a rhythm disorder is diagnosed.
Arrhythmias can be of varying severity - from mild, recorded only on an ECG, to severe, leading to death. Many of these conditions are corrected with medications.
Heart rhythm disturbances can be observed with weakness of the sinus node, inflammatory changes in the myocardium, malnutrition of the heart muscle, coronary artery disease (IHD), and heart attacks.
Contraindications and recommendations for the procedure
Analysis of heart rate variability using a pulse oximetry sensor or ECG leads is a harmless and painless method. There are no contraindications, but you should not put a pulse oximeter sensor or ECG clip on areas with damaged skin.
During the day before the examination, it is not recommended to take medications, and you should also refrain from physiotherapeutic procedures (except for cases of monitoring ongoing activities). The room temperature should be maintained at 19-23°C.
Before the diagnostic procedure, it is advisable to sit or lie down for a few minutes in a comfortable position. During the test, avoid exposing the pulse oximeter sensor to direct sunlight or bright artificial lighting.
Conducting a study using the Wellness Medscanner is covered in detail in the video instructions, and examples of program reports can be viewed at the following link.
Let's look at the different types of arrhythmias
Sinus arrhythmias occur due to disturbances in the sinoatrial node, located in the right atrium. In this case, all teeth maintain size, shape and sequence.
Types of sinus arrhythmias:
Respiratory sinus arrhythmia
Non-respiratory sinus arrhythmia
Sometimes extrasystoles alternate with normal heart contractions. In this case, the following occurs:
After such an attack (paroxysm) there is a long pause. There are complaints of dizziness, nausea, and speech may be impaired. This condition is most often associated with myocardial damage in the area of conducting fibers left after a heart attack or with inflammatory processes. Sometimes this disorder can occur due to problems with the nervous system and accompany severe neuroses.
There is a type of paroxysmal tachycardia, in which the impulses come not from the sinus node, but from the AV node. The picture in this case will be similar, however, on the cardiogram in frequently repeated contractions there will be a P wave, which falls out during paroxysmal tachycardia coming from the atria. This type of arrhythmia is called A-B junction tachycardia.
Diagnostics
It is carried out on an outpatient basis. Hospitalization is required only in critical cases. Specialist - cardiologist.
Approximate list of events:
- Oral questioning of the patient regarding complaints. Objectification of symptoms allows you to build a clear clinical picture and put forward approximate hypotheses regarding the possible disruption of the heart.
- Anamnesis collection. Previous illnesses, habits and lifestyle, family history, other points.
- Measuring blood pressure using routine methods. Using a regular tonometer. Used for immediate assessment of vital signs.
- The basis of diagnosis is daily Holter monitoring. Only it can provide accurate information on the circadian rhythm. The measurement is carried out every half hour or hour and is entered into the memory of an automatic programmable device. Then the device independently calculates the indicator and remembers it.
- Then doctors have more opportunities for diagnosis, the vector becomes clear. Because the numbers usually depend on the probable pathological process.
- The following shows electrocardiography. It is necessary to detect rhythm disturbances. For example, extrasystoles and other similar deviations.
- Echocardiography. Ultrasound research technique. It is used for early detection of anatomical defects or determining the stage of the disorder.
- MRI if necessary.
- Load tests. If there is no reason to suspect anatomical defects, heart failure or other dangerous conditions. It is carried out under the supervision of doctors in order to provide first aid if necessary.
Other specialists may be involved. They are not able to eliminate the cause of the disorders, but identifying abnormalities in the nervous system and respiratory activity is their prerogative.
Low cardiac index associated with increased risk of dementia
Systems in the human body are interconnected, and problems in one of them affect the functioning of others. One example is the influence of cardiovascular factors on the risk of developing dementia. This issue has been studied in some detail in recent years. Here are the results of one of the latest observations by scientists.
One of the indicators of the functioning of the cardiovascular system is the so-called cardiac index - the ratio of minute volume of blood circulation to body surface area. The cardiac index is an important indicator of the functional state of the body, so specialists from the Vanderbilt University Medical Center (USA) traced the relationship between the cardiac index and the risk of developing dementia. Participants, with a mean age of approximately 70 years, had no clinically diagnosed strokes, mini-strokes, or neurodegenerative disorders at baseline. Observation of them lasted about 7 years. The assessment included data such as the subjects' gender, age, high blood pressure, use of blood pressure medications, presence of diabetes, medical history of cardiovascular diseases, atrial fibrillation, smoking and education. At the end of the observation period, 32 patients were diagnosed with dementia, all of whom were in the low cardiac index group.
According to study leader Angela Jefferson, poor heart function may ultimately be a major factor increasing the risk of dementia because the brain does not receive enough oxygen and nutrients. However, unlike a genetic factor that cannot be corrected, the heart can be strengthened through proper nutrition and physical activity, and at any stage of a person’s life.
Source
Features of age-related changes
With age, the minute volume of blood changes, on which the cardiac index depends. Due to the slowing of heart contractions, stroke volume increases (per contraction). So in a newborn baby it is at the level of 2.5 ml, at one year of age - 10.2 ml, and by the age of 16 it increases to 60 ml.
In an adult, this figure ranges from 60 to 80 ml.
The indicator is the same for boys and girls. But from the age of 11 it grows faster in boys, and by the age of 16 a slight difference is determined: in boys it is higher than in girls. But since weight and height (and therefore the total surface area of the body) simultaneously increase, the cardiac index does not increase, but even decreases by 40%.
Modern equipment does not require manual calculations, but produces a comprehensive analysis result. The specialist compares it with standard standards, compares it with other analytical data and judges the amount of compensatory possibilities or pathological changes.