Cardiac arrest: Pixabay The most common cause of death worldwide is cardiac arrest. The condition develops instantly, the outcome is determined in a matter of minutes. The vital activity of the body can prolong first aid in case of cardiac arrest. How to understand that a person needs help and what to do in case of cardiac arrest before medical personnel arrive, read on.
First aid for cardiac arrest
Regardless of the root causes of the failure of the heart muscle, the paramount question is: what to do in case of cardiac arrest?
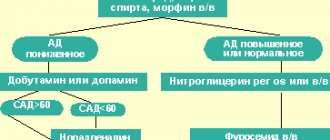
Figure 1. Resuscitation measures for cardiac arrest
The answer is as follows (Figure 1):
- Remain calm and act without delay, master the necessary techniques in advance;
- Remember that irreversibility of the consequences for the brain occurs after 5-6 minutes;
- Therefore, the salvation of the victim depends on the quality of resuscitation measures;
- They include massage of the main organ and artificial ventilation.
First aid for cardiac arrest consists of:
- Checking the victim for a conscious state - you should not shake him or hit him in the face, but gently touch him on the shoulder and ask loudly what’s wrong with him;
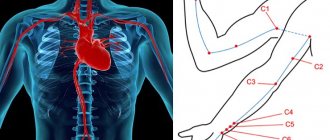
- If there is no reaction, check breathing - place your palm on his forehead and tilt his head back a little, see if his chest rises and falls, listen to sounds and try to feel the emanating air with your cheek for 10 seconds (Figure 2);
- If he is not breathing, immediately call an ambulance and begin cardiopulmonary resuscitation, for which you place the person with his back on a hard surface - the floor or asphalt;
- Kneel in front of him at the level of his forearms, place the heel of your palm on the middle of his chest between the nipples, after removing his outer clothing, and give him an indirect massage with artificial respiration.
Figure 2. First aid for cardiac arrest
First aid for cardiac arrest continues until:
- Medical staff will not appear;
- The victim will not become conscious;
- You will not get tired and will be able to continue resuscitation.
In the latter case, find yourself an assistant from among the people around you.
The first aid course for cardiac arrest includes:
- Not only gaining specialized knowledge about the causes and signs of cardiac arrest;
- Carrying out certain activities and mastering their techniques - special massage, ventilation or mouth-to-mouth breathing.
The risk group for fibrillation is men, with an average age of 45-75 years.
...A spectacular picture. "Discharge! Another discharge! The doctor's confident hands hold electrodes on the patient's bare chest. The patient is unconscious. And now on the monitor of the resuscitator, instead of a straight line, teeth began to run briskly. The doctor takes off his cap with relief, wiping sweat from his forehead. The return to life has happened, the doctors have defeated death!..
This is how most feature films show the defibrillation process. How does everything happen in life?
What is defibrillation and fibrillation
The prefix “de” (Latin) means cancellation, removal, liquidation. Defibrillation is the process of eliminating ventricular fibrillation of the heart.
Ventricular fibrillation (fibrillation) and flutter are pathological conditions in which effective heart contractions do not occur. It's practically cardiac arrest.
Fibrillation cannot stop spontaneously - only under the influence of electrical defibrillation.
See also: Flame motor.
Let's break it down into ventricles. The heart has its own conduction system, capable of generating and transmitting electrical impulses to all its cells. Due to this, a consistent contraction of the chambers of the heart occurs. The body receives oxygen and releases carbon dioxide and other toxic metabolic products that are excreted through the blood.
See also: BlackGate. You can't run away from yourself
With fibrillation, such coordinated work of cells disappears. Individual muscle fibers contract chaotically.
The heart begins to resemble “vibrating jelly.” It loses its ability to contract.
On the ECG, instead of classical waves, chaotic, irregularly shaped waves with a frequency of 200-500 vibrations per minute are recorded.
Every minute reduces the chance of returning to life by 10%
Essentially, fibrillation is cardiac arrest. It is responsible for up to 90% of sudden cardiac death cases.
Blood circulation stops.
Oxygen stops flowing to organs and tissues, hypoxia (oxygen starvation) develops. Cells switch to the economical anaerobic (oxygen-free) metabolic pathway. But at the same time, many toxic under-oxidized products are formed, and acidosis (acidification) develops. Without blood circulation, toxic waste cannot be removed. Cells die.
Brain cells are the most sensitive to hypoxia.
Emergency medical care must be provided within the first 4-10 minutes. (optimally 4-6 minutes - the time that the cerebral cortex can survive without oxygen without serious consequences). Every minute reduces the chance of returning to life by 10%.
If in the 1st minute 90% of patients can be saved, then by the 10th minute, as a rule, no one survives.
Causes of fibrillation
The first and most basic is myocardial infarction.
See also: Heart attack
Other heart diseases (hypertrophic cardiomyopathy, rhythm disturbances) can also lead to fibrillation; metabolic changes, toxins, drug overdose, electrical shock (accident, lightning strike).
Is it possible to start the “motor” after a “short circuit”. The essence of defibrillation
So, with fibrillation, the coordinated work of heart cells is disrupted, they get out of control and begin to contract chaotically.
However, the electrical activity of cells during fibrillation is preserved.
This distinguishes cardiac fibrillation from asystole (lack of systole, contraction) - complete cardiac arrest. With asystole, a straight line is recorded on the ECG. If timely assistance is not provided, fibrillation progresses to asystole. This is due to the fact that heart cells also suffer from oxygen starvation and toxic waste and die.
Asystole may also be the primary condition (it accounts for about 10% of sudden cardiac deaths).
With asystole, a sudden complete cessation of excitability occurs in the heart, a “short circuit.”
In this case, the prognosis is extremely unfavorable. Asystole, if possible, should be converted to fibrillation. The cells must be electrically active, otherwise it will not be possible to “start the engine”.
Defibrillation is the effect of a low-intensity, but high-voltage current on the heart.
This leads to the suppression of all electrical impulses, the direction of which does not coincide with the direction of the defibrillator current. All pathological foci of excitation are suppressed, leaving only those that provide the total vector of normal cardiac contraction. Effective heart function is restored.
How is defibrillation performed?
The defibrillator consists of two blocks: storage and electrode. In the first, electrical energy is accumulated and converted (the current decreases while the voltage increases). Electrodes are placed on the chest and send an electrical current to the heart. There are single- and multi-channel defibrillators. Single-channel has one electrode, and multi-channel has two.
It is desirable that the defibrillator model include an electrocardiomonitor. It allows you to record ECG outside the discharge.
The patient lies on a flat surface. A spacer is required between the electrodes and the body: for example, electrically conductive gel, wipes moistened with a hypertonic NaCl solution or water. The person providing assistance must not touch the patient’s body or other objects (even the surface on which the person is lying. Electrodes are installed on the right under the collarbone and on the left along the anterior axillary line outward from the apex of the heart (then the electrical strength of the impulse will coincide with the direction of the normal electrical axis of the heart) The discharge is applied sequentially with increasing power: 200 J > 300 J > 360 J.
Basic cardiopulmonary resuscitation. What to do if a person falls and loses consciousness before your eyes
There is no time to wait for an ambulance with a defibrillator to arrive. No more than 10 minutes left. What to do?
Cardiac arrest can be suspected if:
- lack of breathing and pulse (check on the carotid arteries),
- lack of pupil reaction to light,
- blue or gray complexion.
Sound the alarm: someone calls the resuscitation team, and someone starts basic cardiopulmonary resuscitation (CPR): chest compressions and mouth-to-mouth artificial respiration. If one person provides assistance, 2 breaths per 15 heart beats; if there are two, the ratio of blowing to pressing is 1:5.
The essence of CPR: artificial imitation of blood circulation occurs. The lungs “breathe” and the heart “contracts.”
The body suffers less from hypoxia.
The task is to hold out until resuscitators arrive with a defibrillator and a set of medications.
Government programs
The sooner specialized assistance is provided, the better the prognosis for life and its quality. In Europe and the United States, programs have been adopted and are being implemented to equip not only medical institutions and ambulances with automatic defibrillators (AEDs), but also public places: shopping centers, train stations, airports, hotels, concert halls, schools.
An airplane cannot land at US airports without a defibrillator on board.
A defibrillator is required in every public school in New York State. More than 50% of US government agencies are equipped with AEDs.
According to British experts, installing AEDs in public places and training staff to use them effectively will save thousands of lives in the next 10 years. In Hungary, all private doctors have an AED. In Germany, all large enterprises are equipped with AEDs
In 2015, the five-year state program “Cardiology” ended in our country. As part of this program, today almost all medical institutions and ambulances are equipped with the most modern biphasic defibrillators with a maximum power of 360 J, which is recommended by the European Association of Cardiac Arrhythmias.
The state program “People’s Health and Demographic Security of the Republic of Belarus” has been adopted (calculated until 2021), where a separate item includes equipping public places with defibrillators.
No less important than equipping public places with AEDs is the medical literacy of the population. Recognizing cardiac arrest in a timely manner and performing basic CPR is the key to saving more than one human life.
Consequences of defibrillation
Only 30% survive cardiac arrest.
Only 3.5% return to normal life, without serious health consequences!
This is usually due to late provision of assistance, when the brain, heart, kidneys, and liver have already been damaged by ischemia. It is important not just to save life. It is equally important to maintain its quality.
The most sensitive organ to ischemia is the brain. If it is possible to restore cardiac activity only after 7-10 minutes, the patient may experience mental and neurological disorders. Delayed help will lead to profound disability for the victim, who will remain a “vegetable” for the rest of his life.
How to prevent sudden death
See also: IHD. Oxygen was cut off to the heart
Remember, in first place - by a huge margin - among the causes of sudden cardiac death is myocardial infarction. Prevention of cardiac death is the prevention of coronary artery disease and myocardial infarction.
See also: Arterial hypertension
A healthy lifestyle, proper nutrition, cultivation of only healthy habits, drug correction of arterial hypertension.
Our life is in our hands!
Main photo of the article from healthversed.com
You can't hesitate!
If you find yourself near a person whose heart has stopped, the main thing you need to do is act quickly. There are only a few minutes to save the victim. If assistance for cardiac arrest is delayed, the patient will either die or remain incapacitated for life. Your main task is to restore breathing and heart rate, as well as start the circulatory system, since without this, vital organs (especially the brain) cannot function.
Emergency care for cardiac arrest is needed if the person is unconscious. First, stir him up, try calling out loudly. If no reaction is observed, proceed with resuscitation measures. They include several stages.
What is an ICD (implantable cardioverter defibrillator)
An implantable cardioverter defibrillator (ICD) is a device that automatically recognizes and provides antiarrhythmic treatment for most cardiac tachyarrhythmias, including ventricular tachycardia (VT) and ventricular fibrillation (VF).
ICD cardioverter-defibrillator device
An implantable defibrillator is small in size—no larger than a pager—and is implanted under the skin of the upper chest. An implantable defibrillator consists of a metal (titanium) box that contains a microcircuit and a battery. The ICD stimulates the heart when the heart stops or beats irregularly or too slowly. An ICD can also detect the electrical activity of the heart. If the pacemaker detects that the heart is beating on its own, it does not send an electrical impulse, i.e. does not stimulate the heart.
In addition to the usual functions of maintaining the heart rhythm at a certain frequency, the implantable defibrillator monitors the occurrence of abnormal, irregular rhythms. If tachyarrhythmias occur, the ICD, using special stimulation algorithms, will perform painless restoration of sinus rhythm, or defibrillation.
An implantable cardioverter defibrillator (ICD) consists of:
• A battery that supplies electrical energy to the implantable defibrillator so it can stimulate the heart (send an electrical impulse along the electrode to the heart). A small sealed lithium battery lasts for many years. When the battery is depleted, the implantable defibrillator is completely replaced.
• A microcircuit is like a small computer inside a pacemaker. The microcircuit transforms the battery energy into weak electrical impulses that the patient does not feel. The microcircuit controls the duration and power of electrical energy expended for the pulse.
• Connector block—a clear plastic block located on the top of the implantable defibrillator. The connector block is used to connect the electrodes and the pacemaker.
Electrodes
An implantable defibrillator is connected to the heart through veins using special electrodes. Electrodes are attached in the cavity of the right atrium and in the cavity of the right ventricle. Depending on the type of ICD (single-chamber, two-chamber, three-chamber), each electrode has its own design features and is designed to stimulate one of the chambers of the heart.
The electrode is a special coiled conductor that is flexible enough to withstand the torsion and bending caused by body movements and heart contractions. The electrode transmits an electrical impulse generated by a pulse generator to the heart and carries back information about the activity of the heart.
The electrode contacts the heart through a metal head at the end of the wire. With its help, the stimulator “monitors” the electrical activity of the heart and sends electrical impulses (stimulates) only when the heart requires them.
For better fixation of the electrode to the myocardium, special active fixation electrodes were developed. At the end of the electrode there is a screw-in spiral, with which the electrode is fixed to the area that needs to be stimulated. The spiral extends during the implantation of the electrode and, if there is a need to replace it, it is screwed in in the opposite direction and the electrode is easily removed.
In the event that cardiac activity is completely absent or the rhythm is very rare, the stimulator goes into constant stimulation mode and sends impulses to the heart at a given frequency. If the heart's own rhythm appears, the stimulator will go into standby mode, i.e. will operate in on demand mode.
Programmer
The programmer is a special computer that is used to control and change the settings of the pacemaker. The programmer is in the hospital. The doctor uses this special computer to see how the pacemaker is working and, if necessary, change the pacemaker settings.
During a follow-up visit or while you are in the hospital, your doctor may place the programming head (much like a computer mouse) over the implanted pacemaker. This allows:
• Obtain information from the pacemaker. Information obtained from the pacemaker shows how the pacemaker and the heart are working. Based on this information, the doctor can change the pacemaker settings.
• Change pacemaker settings. If necessary, the doctor can change the settings of the implanted pacemaker without any surgery.
What types of ICDs are there?
Single chamber ICD
A single-chamber ICD is used in cases of atrial fibrillation or when the patient does not have transient conduction blocks and the heart rate fully corresponds to the needs of the body. The stimulator has one ventricular electrode, which is placed in the cavity of the right ventricle. When VT or VF occurs, the pacemaker delivers a defibrillator shock. The stimulator has an algorithm for ultra-frequent and programmed stimulation to prevent an attack of VT with “painless stimulation”. In addition to the high efficiency of the painless stimulation algorithm in stopping VT, this mode practically does not consume the pacemaker battery charge. In this case, the defibrillator does not discharge. If the patient has bradycardia, the ICD works like a regular pacemaker.
Dual chamber ICD
A dual-chamber ICD contains two pacing chambers designed to stimulate the right atrium and the right ventricle. Electrodes are placed in the appropriate areas, thereby tracking the heart rhythm in the atria and ventricles. During AV blockade, the ICD paces the atrial and ventricular rhythms. Antitachycardia therapy is carried out at all levels, including the ability to stop a sudden increase in atrial rhythm during atrial flutter, atrial tachycardia, and supraventricular tachycardia with antitachycardia pacing (ATS). ATC is widely used to provide pain-free therapy for VT, thereby preserving ICD battery charge.
Three-chamber ICD (CRT/ICD)
Cardioverter-defibrillator with cardiac resynchronization therapy. CRT/ICD is used to treat heart failure (HF) by synchronizing the ventricles of the heart into a single heartbeat cycle. CRT/ICD can provide the full range of antiarrhythmic therapy, including defibrillator shock therapy to restore heart rhythm.
How does an ICD work?
Therapy of tachyarrhythmias
An ICD pacemaker constantly “monitors” the electrical activity of your heart. It can always tell what your rhythm is, including performing the function of a “Holter monitor” by recording fragments of the heart rhythm into memory, helping the doctor learn more about the patient’s rhythm than a regular electrocardiogram. If a tachyarrhythmia occurs in the heart, the stimulator algorithms will provide electrical therapy automatically. The type of treatment and program of stimulator functions depends on the settings that your doctor chooses. After ICD implantation, the doctor must communicate what therapy he has prescribed.
Ventricular fibrillation is a very life-threatening event. The ICD is specifically designed to restore sinus rhythm with a shock shock. This is called defibrillation. Your ICD has pain-free rhythm restoration (anti-tachycardia function) and anti-bradycardia function to treat all types of bradyarrhythmias.
Defibrillation
If the ICD detects VF, it delivers a high-energy shock. This is called defibrillation. During defibrillation, a shock is delivered directly to the heart. Restoring sinus rhythm requires much less energy (1/10th) compared to external defibrillation, which is performed by doctors in emergency situations.
The total time from the onset of a VF attack to the defibrillator shock is about 10 seconds. During this time, energy accumulates in the ICD, which is necessary to produce a high discharge during defibrillation.
Cardioversion is the restoration of heart rhythm by a defibrillator discharge (shock energy discharge). There are two types of electrical cardioversion: external, by applying special plates to the chest, and internal, through an electrode in the right ventricle with an electric current discharge.
Antitachycardia pacing (ATP)
Antitachycardia pacing has been widely used to suppress most cardiac tachyarrhythmias, including VT. The meaning of ATS is to determine heart rhythm disturbances and suppress an attack through ultra-frequent or programmed stimulation.
ATS is widely used to provide pain-free therapy for VT, thereby preserving battery charge. If the ATS is ineffective or in VF, it produces a defibrillator discharge.
If ventricular tachycardia occurs, the ICD will check for the abnormal rhythm and provide the necessary therapy to restore sinus rhythm. The type of antitachycardia function program is determined by your doctor when programming the ICD. If an antitachycardia function is established (painless relief of tachyarrhythmias), then during an attack of VT the stimulator will restore the correct heart rhythm with frequent electrical stimulation with a certain sequence. This stimulation is called antitachycardia therapy; when it occurs, the patient does not feel it.
Antibradycardia pacing
If the heart rhythm becomes very slow or skips (pauses) occur, the ICD can work like the simplest pacemaker used for bradycardia. The atrial and ventricular pacing chambers synchronize the upstream and downstream rhythms, thereby creating the optimal pacing pattern.
Alarm system
The ICD may have a built-in function to alert the patient to the need to see a doctor for evaluation. The ICD can be programmed to sound 30-second beeps when conditions require urgent medical attention. The two different beep tones correspond to different reasons. The signals are repeated every 24 hours until the doctor reads the information using the programmer. When the ICD beeps, you should immediately consult a doctor!
ICD implantation procedure
Pacemaker implantation is a surgical procedure in which a small incision is made in the right (if you are left-handed) or left (if you are right-handed) subclavian region. Depending on which pacemaker you are implanted with, one, two or three electrodes will be inserted through a vein and placed inside the heart under X-ray guidance.
As with most surgical procedures, a short course of prophylactic therapy with antibiotics and anti-inflammatory drugs will be prescribed after pacemaker implantation.
Before the operation, the attending physician will limit or stop taking certain medications, and the choice of anesthesia will be determined by the anesthesiologist. The operation of implanting (sewing in) a stimulator seems simple, since it causes little damage to the tissue, and is carried out in an operating room equipped with an X-ray machine. A vein is punctured (pierced) under the collarbone, a special plastic tube (introducer) is inserted into it, through which endocardial electrodes are inserted into the superior vena cava. Under X-ray control, the electrodes are directed into the right atrium and right ventricle, where they are fixed.
The most difficult procedure is to install and secure the tip of the electrode in the atrium and ventricle so as to obtain good contact. Usually the surgeon makes several tests, all the time measuring the threshold of excitability, i.e. the smallest impulse value (in volts) to which the heart responds with a contraction visible on the ECG. The challenge is to find the most sensitive spot and at the same time get a good ECG graphic recorded from the electrodes being installed. After fixing the electrodes, they are connected to a stimulator, which is placed in a formed bed under the fascia of the fatty tissue or under the muscles of the chest.
Of course, the operation requires strict sterility and careful control of bleeding to avoid accumulation of blood under the skin and suppuration. The stimulator itself and electrodes are supplied sterile. In total, all manipulations take from one to two hours.
Our clinic successfully performs ICD implantation operations and its subsequent programming in an optimal mode.
Possible causes of cardiac arrest
Poor general health and atmospheric pressure can play a bad joke on heart patients, but there are other factors that can stop the heart muscle from working.
- First aid for stroke: step-by-step algorithm of actions
Figure 3. What is Thrombosis
Cardiac arrest, causes:
- Coronary circulation disorders caused by excessive physical exertion or severe emotional shock;
- Poisoning and serious breathing problems;
- Acute allergic reactions, anaphylactic shock;
- Thrombosis (Figure 3), stroke and heart attack.
Sudden cardiac arrest can also be caused by other external influences on the human body:
- Mechanical injuries of the chest;
- Heavy blood loss of large volumes;
- Heat or sunstroke (Figure 4);
- Electric current discharge;
- By drowning or suffocation.
Figure 4. External factors that may cause cardiac arrest.
It is important to know and take into account which drugs cause cardiac arrest, these include:
- Beta blockers - bisoprolol, atenolol, bisoprolol and calcium antagonists - verapamil, diltiazem - they lower blood pressure, but they are strictly forbidden to be taken by those whose pulse is equal to or below 60 beats per minute; they are prescribed by doctors only for hypertension;
- Antibacterial agents - roxithromycin, azithromycin, related to macrolides - these antibiotics double the risk of tachycardia and can contribute to sudden death; they are not suitable for the elderly and those who suffer from heart disease.
All drugs that cause cardiac arrest can be divided into seven main groups:
- Antibiotics;
- Cardiac glycosides;
- Muscle relaxants;
- Potassium;
- Psychotropic drugs (Figure 5);
- Tablets and mixtures for heartburn;
- Vitamins. Figure 5. Drugs and antidepressants can cause cardiac arrest.
Why defibrillators stop the heart rather than start it
People who are far from medicine have little idea of how this or that device works. There is no point in a healthy person learning the tricks of X-ray equipment, since all his bones are intact. But everyone who sometimes watches movies has seen how doctors use a defibrillator.
Defibrillator. Source or Sources, can be used in the following meanings: Source (natural), spring, spring - the release of groundwater to the surface of the image:
wattpad.com
In short, it looks like this: a human being, a social being with reason and consciousness, as well as a subject of socio-historical activity and culture, has a cardiac arrest. Then the doctors, using a miracle device, try to restart the heartbeat, and only after a pause and loss of faith in success, the doctor manages to bring the person back from the dead with his last attempt. Dramatic, beautiful, but not at all true.
In fact, with such footage, experienced doctors simply hold back laughter, since they know very well how the defibrillator
.
To understand how this device works, you must first understand that there is fibrillation
and remember that the prefix
de
means something like negation.
What does fibrillation mean: Cardiac fibrillation is a painful condition of the heart in which individual groups of muscle fibers contract in a disjointed and uncoordinated manner?
So, cardiac fibrillation is a condition in which individual groups of fibers, a thin unspun thread of plant, animal or mineral origin, of the heart muscles contract uncoordinated with neighboring ones. Coordination of work can mean: Work - the functioning of any system - a mechanism, biocenosis, organism or community - as well as its part of these groups of fibers disappears, and the heart, a hollow fibromuscular organ that ensures blood flow through the blood vessels through repeated rhythmic contractions, ceases effectively pump blood.
The state of fibrillation itself is characterized on the cardiogram as a curve with a large number of peaks and valleys, which indicates an increased heart rate and arrhythmia of the heart as a whole. The heart rate in this state can reach 200-300 beats per minute, a non-systemic unit of time.
Ventricular fibrillation is a generalized name for some types of cavities in human and animal organs on a cardiogram. Image source: zabserdce.ru
Well, there is no trace of a straight line on the cardiogram, a method for recording and studying the electric fields generated during the work of the heart in this situation. Already from these data it becomes clear that the main task of a defibrillator is a device used in medicine for electrical pulse therapy of cardiac disorders and a stopped heart, and the removal of the condition from it is a concept denoting a set of stable values of variable parameters of the object of fibrillation (the disorderly work of various groups of muscle fibers of the heart muscle) . How does this happen?
How does the heart beat?
Until you begin to understand the human structure, it is difficult to even imagine how intricately designed our bodies are. It is difficult to explain the mechanism of the heart in accessible language, but there are some things you can try. To begin with, you should understand that all heart cells have internal automaticity, that is, the ability to contract independently of neighboring ones. This contraction occurs due to the accumulation of electrical charge on the membrane, a thin flexible film or plate usually attached around the perimeter of the cell, so electrical stimulation can cause the cell to contract under the influence of external sources.
Image source: giphy.com
Cells, the structural and functional elementary unit of the structure and vital activity of all organisms (except for viruses and viroids - life forms that do not have a cellular structure) of the atria, have an internal frequency of automatic contractions of approximately 60 times per minute. And in the cells located below, internal automatism Automatism (art) is the act of creating weaker, and in the ventricles it reaches up to 40 contractions, which can mean: An abbreviation, that is, an abbreviated designation, the name of someone, something per minute. With their contraction, the external cells transmit an electrical impulse deep into the heart, causing more and more new cells to contract. This is how the electrical impulse reaches the ventricles, and they push out blood. But if some of the cells are sick, then they simply do not have time to contract, and the impulse is transmitted further along the cell membrane. At the end The End is completeness. The End is the limit, boundary, edge of any object or event, as well as its part adjacent to this limit. The End (region) is an outdated unit of territorial division of the ends, it will reach the ventricles, but the blood is liquid and moving connective tissue of the internal environment of the body, heart into body is an ambiguous word, it can mean pushing out a little, because the ventricles simply did not have time to fill.
If there are a fair number of diseased areas of the heart, a category that expresses the external, formal relationship of objects or their parts, as well as properties, connections: their size, number, degree of manifestation of one or another property, then various areas of the heart muscle or muscles (from the Latin musculus - muscle ) - part of the musculoskeletal system in conjunction with the bones of the body, capable of contraction, begin to contract on their own. That is, the fibrillation phenomenon described above occurs. This condition is a direct threat to life, but it can be relieved by stimulating the heart cells with an external electrical impulse. The cells will work in a coordinated manner again, the threat of intimidation, the promise of harming someone, the evil of death will disappear.
How is defibrillation performed?
The basis of the defibrillator’s operation is the generation of short pulses of electricity, a set of phenomena caused by the existence, interaction and movement of electrical charges, which are then transmitted through the human body to his heart.
Basically, 2 types of defibrillators are used:
- Professional - manually controlled, having electrodes, an electrical conductor that has electronic conductivity (conductor of the 1st kind) and is in contact with an ionic conductor - an electrolyte (ionic liquid, ionized gas, solid in the form of VIEW: Literally: What is available the look of the irons.
Manually controlled defibrillator Control (philosophy) is an element, a function of such structured systems that arose naturally (evolutionary) or artificially (man-made). Image Source Multiple Term: Optical Image Monochrome Image Grayscale Image Full Color Image Digital Image Raster Image Binary Image Bitmap: cctpowertech.com
2. For non-professionals, automatic defibrillators with adhesive electrodes are available.
Defibrillator with sticky electrodes. Image source: internetmedicine.com
Schemes for installing irons (sticking electrodes) are different, but one of them is the most common. With this scheme, one iron is installed above the right nipple of the patient’s body, and the other in the area of the lower left rib.
One of the positions for installing defibrillator electrodes. Image source: istockphoto.com
The stimulation itself is carried out by a short-term electrical impulse (t=0.01 s) of high voltage. If the person's chest is not opened, then stimulation begins with 4,000 volts may mean (let the reader not be alarmed by such a high voltage, the current strength of the electrical impulse is actually work, occupation, action not for fun; a commercial enterprise, business; a question that requires resolution is relatively small, otherwise the patient is a person or other living being receiving medical care, undergoing medical supervision and/or treatment for any disease, pathological condition, or other, and would immediately die). If fibrillation does not stop, gradually the voltage Electrical voltage between points A and B - the ratio of the work of the electric field when transferring a test charge from point A to B to the value of this test charge of single pulses - a vector physical quantity that is a measure of the mechanical movement of a body - is brought to 7,000 volts. If the patient falls into a state of fibrillation during surgery with the chest open, then the defibrillator voltage should be within the range of 1,000-2,000 volts.
Thus, the defibrillator does not “start” the stopped heart, but, on the contrary, stops it with an electrical discharge. After this, the heart, in case of successful defibrillation, a device used in medicine for electrical pulse therapy of cardiac arrhythmias, should restore its normal electrical activity (rhythm).
Take care of yourself and your heart!
If you have anything to add on the topic, do not hesitate to write in the comments!
Subscribe to the Nauchpop channel. Science for everyone . Stay tuned, friends! There are a lot of interesting things ahead!
Source:Go
Causes and symptoms
Due to the fact that the heart suddenly stops beating, people of pre-retirement age most often die if they do not receive help. Risk factors for cessation of contractions are the following pathologies:
- pathologies of the circulatory system. Violations may be associated with stress, increased physical activity;
- respiratory problems;
- anaphylactic shock;
- stroke or heart attack;
- the appearance of blood clots.
Timely actions will help avoid complications, but the heart may stop beating due to external factors. These include mechanical damage to the chest area, electric shock, as well as thermal or solar damage, and large blood loss.
You can begin first aid for sudden cardiac arrest if you have the following symptoms of clinical death:
The person stops breathing.
- the person suddenly loses consciousness. At the same time, they note the lack of reaction to any stimuli;
- the pulse disappears. To check for its presence, you need to place two fingers on the carotid artery in the neck;
- the victim is not breathing. This can be understood by the fact that the chest does not move;
- the pupils become wide, and there is no reaction to light;
- the skin becomes pale and may acquire a bluish tint.
If these symptoms are present, then a stop has occurred. It is imperative to call emergency doctors, and before they arrive, try to start the heart on your own.
The Last Fireworks: What Happens to the Body When We Die
As a patient approaches death, changes occur in his body. They concern breathing, blood circulation, consciousness. We explain in detail what happens: if we understand death, perhaps we will be less afraid of it.
Author: Jacob Zimmank
The author of the article is a former employee of the palliative care service, which supervises dying people at home. He was amazed at how calmly many people faced their own death.
When does dying begin? At what point does a person begin his path to death?
Dying begins long before we are born. It is laid in the womb, in a cluster of cells from which the unborn child is formed. Some cells are redundant and need to make room for new ones. This is the only way the child’s organs can appear. It is due to this that there are only two kidneys, and only ten fingers on the hand. The genome of each cell already contains programs that act as a kind of “catapult”. It turns on at the moment when the cell becomes unnecessary or dangerous for the body. In this case, the cell voluntarily destroys itself.
Becoming a person is a process that involves both life and death. According to palliative medicine doctor Jean-Domenico Borasio, death is “a necessary condition so that we can, in principle, be born as viable organisms.”
“What we know for certain is that a person does not die suddenly, overnight” - Jean-Domenico Borasio, palliative care doctor
Death is omnipresent - but once we are born, we forget about it. And, if all is well, then death will appear in our lives again only after a few decades. Often this will be a condition that cannot be cured: cancer, heart disease, or kidney disease that means they can no longer cleanse the blood. And then the process of dying begins.
“What we know for certain is that a person does not die suddenly, overnight. The organs of the human body stop functioning gradually, not all at the same time, and then at some point their work stops,” says Dr. Borasio. As a result of the chain reaction, the liver, kidneys, lungs and heart stop working.
There are a variety of diseases, but at the end of life everything always follows the same pattern: the heart stops beating, breathing stops and, last of all, consciousness fades away. At the same time, it is very difficult to separate the work of the heart and brain. If the heart stops pumping oxygenated blood, brain cells begin to die within seconds. And after a few minutes, brain death occurs: at this moment the EEG will show a straight line instead of the usual curves and teeth. The reflexes that control the deep parts of the brain responsible for breathing, swallowing and consciousness also stop working. Thus, when the heart stops, the brain also stops working.
It also happens the other way around. The brain contains centers that regulate all vital functions: blood pressure, heart function, breathing. If these centers are damaged, breathing will stop and the heart rhythm will be disrupted. Often this damage occurs when intracranial pressure rises sharply as a result of a car accident or accident. The bones of the skull are hard, so with a strong blow, the soft tissue of the brain is squeezed into the only natural opening in the skull - the foramen magnum. Through it, the cranial cavity communicates with the spinal canal (the spinal cord passes into the brain stem). If the brain stem is pinched or damaged, the person dies.
There are no clear signs, but there are general patterns
Dying people live the last years, months and days of their lives in different ways. “The dying process is very individual,” says Lukas Radbruch, president of the German Society for Palliative Medicine and professor at the University Hospital Bonn. It often lasts for months or even years. Doctors divide dying into three stages: at the beginning comes the “terminal” stage, which lasts one to two years. At this time, the functioning of individual internal organs gradually decreases, and the dying person increasingly experiences fatigue. This is followed by the “pre-final” stage, which can last several weeks or months. At this time, symptoms such as shortness of breath and pain appear. And finally, the “final” stage - the last days. The patient stops eating and drinking and slowly fades away. “It is important to remember that this division of dying into stages is nothing more than a convention,” notes Radbruch. It is important for providing treatment and care, but does not provide an accurate picture and “does not help determine when the patient will die.”
“It used to be believed that the approach of death was indicated by pale skin in the nasolabial triangle,” says Radbruch. But this is also an unreliable sign. Currently, research that allows us to accurately determine the time of death is at an early stage. Some scientists are testing blood samples for markers that can be used to calculate remaining life expectancy. Radbruch says the best thing to do is ask the attending physician: Would she be surprised if she learned that the patient died that night or next weekend? If the doctor says that she is not surprised, then it is time to prepare for death.
Part 2. Death rattle
Although dying is a highly individual process, there are certain physical changes that are common to most patients (Palliative Care Review: Plonk & Arnold, 2005). As we approach death, there are more and more similar features, although the cause of death may be different. The dying are exhausted, have difficulty breathing and experience pain. Breathing changes: at first it becomes shallow, then intermittent, but after a while the dying person can again take a deep breath.
Doctors suggest that by this time the centers of the brain responsible for breathing have already been affected. They react late to the presence of carbon dioxide in the blood, allowing it to accumulate in large quantities. In some cases, breathing noises occur, one of which used to be called the “death rattle.” Due to the inability to expectorate and clear the throat, secretions accumulate in the pharynx and bronchi, which affects the passage of air flow during breathing.
The death rattle is often a terrible sound, but there is no evidence that the dying person is suffering at this moment. The same applies to an increase in the level of carbon dioxide in the blood - it is assumed that this has a rather calming and soporific effect. The death rattle (as the name suggests) indicates that death is imminent (American Journal of Hospice and Palliative Medicine: Morita et al, 1998). With very little time left, wheezing may become uncontrollable.
In addition, in the last days and hours before death, changes in blood circulation are observed. The body tries to deliver the small amount of oxygen that the heart is still able to pump through the blood to vital organs. “The pulse weakens and is often barely palpable, the hands become cold and the lips may turn blue,” explains Lukas Radbruch. “It’s a stress reaction.” In some cases, the heart begins to beat faster, the blood pressure drops, and a slight fever may even appear.
When consciousness fades
Radbruch says: “Someone remains conscious until his last breath. Another may experience anxiety and even hallucinations. And the third one just quietly fades away.”
There are enough reasons for such changes. On the one hand, due to uneven flow of blood and oxygen, brain metabolism is disrupted. On the other hand, some organs stop working, and because of this, toxic substances accumulate in the blood. For example, urea, which is excreted through the kidneys, can damage nerve cells in high concentrations. (But the dying person does not suffer from this either. Oblivion caused by a high concentration of urea in the blood is similar to anesthesia - it does not hurt the person, it is even pleasant.)
In addition to urea, ketone bodies accumulate in the blood of a dying person in large quantities, which also affect a person’s consciousness. They are produced from fat and, in conditions of energy deficiency, are used by the body as a substitute for glucose, which is necessary to nourish the brain and muscles. This is exactly what happens when dying: a person stops eating, but does not experience hunger (JAMA: McCann et al., 1994).
When dying, many patients quietly fade away or, on the contrary, become excited and whisper something excitedly. It may seem that they have already left this world, but despite this, “we must treat the dying as if they understood everything,” emphasizes Lukas Radbruch. “We don’t know exactly how much they can take in.”
Many patients continued to perceive what was happening even after cardiac arrest. This is evidenced by the results of a large study. Scientists interviewed 140 people from the UK, Austria and the US who had experienced cardiac arrest. Nine percent of those surveyed reported having had a near-death experience such as feeling fear, seeing a light or seeing family members.
Two of the respondents remembered the process of their own resuscitation. One of them talked about watching the doctors’ actions from above, from the corner of the room. He remembers that the doctors turned on the defibrillator and tried to “start” the heart, make it beat at the right rhythm again. And this coincided with what was happening in reality. It is interesting that the patient regained consciousness only a few minutes after cardiac arrest.
Last fireworks
When the heart stops and stops supplying the brain with oxygen, nerve cells do not die immediately. On the contrary, their activity increases sharply. This was reported by scientists who studied the electrical activity of the brain in laboratory rats (the rat’s brain is in many ways similar to the human brain). A few minutes after the rodents' hearts stopped beating, a burst of electrical activity could be observed—exceptionally strong. “This may explain why the memories of patients who have experienced clinical death are so real and accurate,” writes one of the study authors, anesthesiologist George Mashour of the University of Michigan Medical School.
When the heart stops, a real fireworks display occurs in the brain. Nerve cells release enormous amounts of norepinephrine, which affects the frontal lobes of the brain and sharpens attention. There is also a release of serotonin, so hallucinations and mystical insights are possible. And at the very last moment, dopamine arrives from the midbrain. It is responsible for the feeling of satisfaction, gives a feeling of warmth and joy. Perhaps even happiness.
The original interview is on ZEIT ONLINE.
We thank Vera Foundation volunteer Veniamin Sapozhnikov for translating this article.
How to support hospice patients?
It is very easy to support hospice patients. You can sign up for monthly donations (by checking the box next to “I want to donate monthly”) or make a one-time donation :
Thank you always.
Share
Tweet
Share
Share
SIMILAR
CPR Action Plan
- We pay attention to the safety of the approach to the victim.
- We check the victim's consciousness - no.
- We call an ambulance.
- We examine the oral cavity.
- We check for the presence of heartbeat and breathing - none.
- We perform indirect cardiac massage with artificial ventilation of the lungs until the ambulance arrives or the person regains consciousness (reacts to your actions, coughing, groaning, breathing and heartbeat appear).
security check
We check whether there is a threat from above, below and on the sides - heavy objects that can fall on you, wires, wild animals, slippery floors and many other factors that can not only prevent you from performing resuscitation, but also put your life at risk.
- Carrying out cardiopulmonary resuscitation: the correct algorithm of actions
Consciousness check
The first step is to make sure that the victim is unconscious. To do this, you don’t need to hit him in the face, just grab him by the shoulders and loudly ask him something. Immediately pay attention to the people around you and ask them to assist you in saving the person.
Attention! If the victim feels bad in front of you, then after you are convinced that he is unconscious, you should immediately check the pulse in the carotid artery (more details in the fifth paragraph). In the absence of a pulse (exclusively in the absence of a pulse), you should give the victim a precordial blow.
Calling an ambulance
From a landline number 03, from a cell phone 103 or 112. Read more about how to call an ambulance and talk to the dispatcher correctly.
Inspection of the oral cavity
We examine the oral cavity to determine whether there are foreign objects in it that impede breathing. If there are foreign objects (including vomit, mucus, pieces of food), we clean it with gentle movements of a finger wrapped in gauze or any other fabric. Pay attention to the position of the tongue so that it does not fall into the throat, thereby closing the path for air.
First aid for a child
A child is not a small adult. This is a completely original organism, the approaches to which are different. Cardiopulmonary resuscitation remains especially relevant for children in the first three years of life. At the same time, you should not give in to panic and act as quickly as possible (after all, you only have five minutes left).
- The child is placed on the table, unswaddled or undressed, and the mouth is freed from foreign objects or impurities.
- Then, with the pads of the second and third fingers of the hand, located on the lower third of the sternum, pressure is applied at a frequency of 120 pushes per minute.
- The thrusts should be gentle, but intense (the sternum moves to the depth of a finger).
- After 15 compressions, take two breaths into the mouth and nose, covered with a napkin.
- In parallel with resuscitation, an ambulance is called.