Relevance of the problem
Cardiac arrhythmia is one of the most common manifestations of heart disease and other pathological conditions outside the cardiovascular system.
Extrasystole (ES) is the most common rhythm disorder in children. According to the literature and our own observations, in the structure of arrhythmias it reaches 75% (Shkolnikova M.A., 2006; Pshenichnaya E.V., 2008), while its growth has been noted over the past decades (Makarov L.M., 1998; Kupriyanova O.O., Oskolkova M.K., 2004; Nagornaya N.V. et al., 2012). Extrasystoles are found in children of all ages, including newborns; they are even detected prenatally. In some cases, ES is detected in healthy individuals, including those involved in sports. The pathogenesis of extrasystolic arrhythmia often involves various electrophysiological phenomena, which are combined in a complex way, with the mutual influence of the central and autonomic nervous systems, indirectly involving other factors. The type of extrasystole in most cases does not allow us to judge its clinical significance and prognosis for a particular patient. In this regard, the choice of treatment and preventive measures often turns out to be the most difficult problem facing a doctor when managing a patient with extrasystole. General goal : to be able to diagnose and determine tactics for managing a child with extrasystole.
Specific goals : to identify the main clinical and electrocardiographic signs of extrasystole, to draw up a plan for examining a patient with extrasystole, to make the most likely clinical diagnosis, to determine a plan of treatment and preventive measures.
Symptoms of the disease
In most cases, extrasystoles do not cause any discomfort. They can happen day and night, but the child will not pay any attention to them.
However, there are disturbances in cardiac activity that are accompanied by:
- weather dependence;
- weakness;
- sleep disorders;
- decreased appetite;
- rapid fatigue;
- weakness;
- a feeling of a strong blow followed by a sinking heart.
Definition of extrasystole. Classification of heart rhythm disorders in children
Extrasystole (Latin extra outside + Greek systolē contraction, compression) is a heart rhythm disturbance characterized by single or paired premature contractions (extrasystoles) of the entire heart or any of its parts (atria or ventricles) as a result of excitation of the myocardium arising from an impulse, emanating not from the physiological source of the heart rhythm (sinus node), but from another part of the myocardium or the conduction system of the heart (heterotopic source of arrhythmia).
ICD X contains the following codes:
— I 49 — other heart rhythm disturbances;
— I 49.1 — premature depolarization of the atria;
— I 49.2 — premature depolarization emanating from the connection;
— I 49.3 — premature depolarization of the ventricles;
- I 49.4 - other and unspecified depolarization.
Etiopathogenesis of extrasystole in children
Extrasystoles can be congenital or acquired; etiologically caused by cardiac, extracardiac and combined factors.
Cardiac causes of arrhythmia include congenital and acquired heart defects, primary and secondary cardiomyopathy, rheumatic carditis, infective endocarditis, non-rheumatic carditis and other intracardiac pathology.
It has been proven that extrasystole is more common in children with mitral valve prolapse and other minor structural abnormalities of the heart compared to children without them.
A special etiological group consists of genetically determined diseases, in which arrhythmias (ventricular ES, ventricular tachycardia) are the main clinical manifestation. This is arrhythmogenic right ventricular dysplasia (ARVD) - a pathology of the heart muscle, predominantly genetically determined, characterized by fibro-fatty replacement of the right ventricular myocardium, which can be either minimal, detected only by histological examination, or pronounced, with varying degrees of involvement of the interventricular septum in the process. and myocardium of the left ventricle (Basso C., Corrado D., Marcus F., 2009; Bockeria L.A., Revishvili A.Sh., Neminushchiy N.M., 2011). In half of the cases, the disease is familial and is a common cause of sudden cardiac death.
ARVD must be excluded in every patient with mono- or polytopic ventricular ES. Currently, for the diagnosis of ARVD, the criteria of Marcus F. (2010) are used, based on data from electrocardiography, echocardiography, MRI, ventriculography, and histological examination. An important ECG criterion for ARVD is the presence of an epsilon wave (e-wave) in patients with ventricular arrhythmias. The epsilon wave is a reproducible low-amplitude signal between the end of the QRS and the beginning of T wave in the right precordial leads (Fig. 1).
Extrasystoles can be observed in diseases of the nervous and endocrine systems (diabetes mellitus, thyrotoxicosis, hypothyroidism), acute and chronic infectious processes, intoxication, overdose or inadequate reaction to medications, deficiency of certain microelements, in particular magnesium, potassium, selenium. To date, there are indications of the role of foci of chronic infection, in particular chronic tonsillitis, in the genesis of extrasystole, but it has not been fully proven.
It has been established that ES can be a manifestation of viscero-visceral reflexes in cholecystitis, diseases of the gastroduodenal zone, gastroesophageal reflux, diaphragmatic hernia, etc.
The appearance of ES after severe emotional and physical overload is explained by an increase in the concentration of catecholamines in the blood. The genesis of extrasystole is also influenced by autonomic dysfunction and psychogenic changes.
In the etiology of ES, the significant role of perinatal pathology (unfavorable course of pregnancy and childbirth, prematurity, intrauterine malnutrition, fetal infections) has been proven, leading to disruption of morphogenesis and functional immaturity of the cardiac conduction system. Perinatal damage to the central nervous system can disrupt the neurovegetative regulation of rhythm with a change in the relationship between the sympathetic and parasympathetic influences of the autonomic nervous system, resulting in electrical instability of the myocardium and the conduction system of the heart, as well as a decrease in the functional reserves of adaptation of the sympathoadrenal link of heart rate regulation.
In cases where the cause of SE cannot be identified, it is classified as idiopathic.
How is extrasystole diagnosed?
Experienced cardiologists help diagnose extrasystole in children. These are highly specialized specialists who are attentive to problems related to cardiac activity.
Most often, ventricular extrasystole in children is discovered accidentally during a general examination. When listening with a phonendoscope, two beats are heard following each other. The first blow is loud and clear, the second is quieter. After such contractions, there is a slight disruption in the rhythm, some pause before the next beat.
As additional diagnostics, the following are prescribed:
- ECG;
- Ultrasound of the heart with Doppler;
- donating TSH and T3-T4 hormones to check the functioning of the endocrine system;
- Holter monitoring;
- general blood analysis;
- general urine analysis;
- blood chemistry.
It is necessary that in addition to the cardiologist, the child is also examined by a neurologist and an endocrinologist.
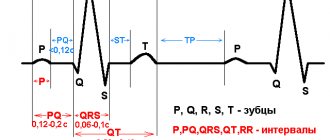
An ECG plays a particularly important role in diagnosing extrasystole (rhythm disturbance) in a child. An electrocardiogram allows you to record the frequency of repetitions of “interruptions”, the location and type of the disease. When printing the results, a shortening of the intervals of the cardiac cycle and a change in the P tooth are observed. With ventricular extrasystole in children, a pause is observed after recording “interruptions” and the absence of the P wave.
Our clinic employs experienced staff who know everything about the functioning of the heart, methods for diagnosing its diseases and effective treatment.
Clinical and electrocardiographic characteristics of extrasystole in children
Extrasystole in children is often asymptomatic, which makes it impossible to accurately determine the time of its occurrence. According to our data, about 70% of cases of arrhythmia are discovered by chance by parents or medical personnel during preventive examinations or in connection with a current or past respiratory infection. Indeed, the connection between NRS and respiratory infections has been proven, which is due to the possible presence of carditis, autonomic dysfunction with hyperactivity of the trophotropic apparatus in the early period of convalescence, when vagal tone predominates against the background of decreased activity of the sympathoadrenal department.
According to our observations, many patients do not complain and do not know about the existence of ES until the doctor informs them about it. If a child with ES has complaints, the most common ones are a feeling of interruptions in the heart’s function, a feeling of sinking in the heart, reminiscent of the sensation when a plane descends quickly or at the beginning of the downward movement of a high-speed elevator; a feeling of short-term (1.0–1.5 s) cardiac arrest followed by a feeling of a strong heartbeat into the chest wall (post-extrasystolic potentiation). Sometimes the described sensations are accompanied by short-term (1–2 s) acute pain in the area of the apex of the heart. In the prepubertal and pubertal period, cardiac arrhythmias, including extrasystole, can have a strong emotional coloring, caused by psycho-vegetative changes, and be accompanied by other cardiac and extracardiac complaints: pain in the heart, increased excitability, sleep disturbances, and meteosensitivity. Manifestations such as dizziness and weakness are observed only with extrasystolic arrhythmia against the background of severe heart damage with hemodynamic disorder.
On auscultation, the extrasystole is perceived as a loud tone or as two tones closely spaced from each other, the intensity of the first of which is increased, and the second is sharply weakened. These sounds arise prematurely in diastole and are accompanied by a compensatory pause. Noises heard above the heart during extrasystoles sometimes disappear (due to insufficient filling of the ventricles with blood); in some cases, on the contrary, the noise is heard only during extrasystolic contraction, which indicates the occurrence of turbulent blood flow in the aorta at the time of extrasystole. Intercalated extrasystoles are recognized by auscultation as premature contractions that are not accompanied by a compensatory pause. With frequent polytopic extrasystoles, physical examination does not always allow us to ascertain this rhythm disturbance.
Sometimes, at the moment of extrasystole, a jerky swelling of the neck veins is noted; after an extrasystole, you can often see or palpate a single increased cardiac impulse (a consequence of post-extrasystolic potentiation). Loss of pulse beats are detected, corresponding to hemodynamically ineffective early extrasystoles, or premature weakened pulse beats (with relatively hemodynamically effective late extrasystoles), accompanied by an extended (compensatory) pause, followed by a slightly increased pulse beat. Bigeminy often manifests itself as bradysphygmia, when only pulse beats caused by normal contractions of the heart reach the palpated artery.
ES verification is carried out based on ECG indicators.
Extrasystoles are classified by location, degree of prematureness, frequency, sequence, compensatory pause, as well as by the characteristics of their lability during functional tests.
Depending on the location of the focus of ectopic activity, extrasystoles are divided into atrial, atrioventricular (atrioventricular, nodal) and ventricular. In rare cases, sinus extrasystole is observed, in which premature excitation occurs in the physiological pacemaker of the heart - the sinus-atrial node.
One of the main electrocardiographic criteria for ES is a shortened diastole before ES and a compensatory pause after it. The shape of the ectopic complex depends on the site of origin of the ES.
With extrasystoles occurring in the ventricles of the heart, the interval between pre- and post-extrasystolic contractions of the heart is usually equal to the time of two normal cardiac cycles; such a compensatory pause is called complete. The compensatory pause after atrial and atrioventricular (atrioventricular) extrasystoles is shorter than after ventricular ones - an incomplete compensatory pause (Fig. 2).
Atrial extrasystole is characterized by the following electrocardiographic signs:
— premature appearance and deformation of the atrial P wave;
- presence of a P wave before the QRS complex;
- the morphology and/or polarity of the P wave in the ES differs from the sinus: for the left atrial localization of the extrasystole, negative P waves are characteristic in all standard and left chest leads; with ES from the middle and lower parts of the right atrium, a negative P wave appears in leads II, III, aVF and a positive P wave in standard lead I;
— PR in atrial ES can be shortened, lengthened and normal;
- the ventricular complex of the extrasystole does not differ in configuration and duration from the ventricular complexes of the main rhythm;
- the compensatory pause is incomplete, but with aberrant QRS it can be complete.
Sometimes the extrasystolic QRST complex is deformed due to aberrant conduction through the ventricles (if intraventricular conduction has not been fully restored by the time the extrasystole occurs), resembling a ventricular extrasystole. In such cases, the extrasystolic P wave often overlaps the T wave of the preceding normal complex (T + P), causing its deformation (Fig. 3).
Atrioventricular extrasystole in terms of QRS changes corresponds to the atrial one (therefore they are combined under the general name of supraventricular, or supraventricular, extrasystoles), but differs from the latter in changes in the P wave, which is always inverted and occupies a different position in relation to the ventricular complex depending on which part it is from. extrasystoles originate from the atrioventricular junction (superior or inferior). With an extrasystole emanating from the upper part of the atrioventricular junction, an inverted P wave precedes the QRS, and the PQ interval is less than 0.12 s. With an extrasystole from the lower part of the atrioventricular junction adjacent to the node, the P wave can overlap its ventricular complex, somewhat deforming the latter, or be recorded immediately after the extrasystolic ventricular complex (Fig. 4).
Ventricular extrasystole is characterized by the following electrocardiographic signs (Fig. 5):
— the P wave preceding the extrasystole is absent (the impulse does not reach the atria retrogradely) or is inverted and recorded after the ventricular complex;
- a significant difference in the shape of the ventricular complex of the extrasystole and the ventricular complexes of the main rhythm - pronounced deformation and expansion of the ventricular QRS complex. The duration of the QRS complex exceeds age parameters (more than 60 ms in children under 1 year old, more than 90 ms in children from 1 to 3 years old, more than 100 ms in children 3–10 years old, more than 120 ms in children over 10 years old);
— the location of the RS-T segment and the T wave is discordant with the direction of the main waves of the QRS complex;
- the presence in most cases of a complete compensatory pause.
The extrasystolic ventricular QRST complex usually resembles the QRST complex in shape when one of the legs of the atrioventricular bundle is blocked. Ventricular extrasystoles can be monotopic (excitation occurs in one ectopic focus); in this case, all extrasystolic complexes are identical in shape and all coupling intervals are of equal size. Ventricular extrasystoles are divided depending on location into right ventricular (most often in children from the outflow tract) and left ventricular. Right ventricular extrasystoles are characterized by the morphology of the ventricular complex according to the type of left bundle branch block, left ventricular extrasystoles - according to the type of right bundle branch block. The inconstancy of the coupling interval and the shape of the extrasystolic complex indicates that the extrasystoles come from different ectopic foci (polytopic extrasystole, Fig. 6).
According to density, ES can be single (separately located), paired and group. A group of 3 or more ES is called paroxysm of ectopic tachycardia.
There is an allorhythmic ES, that is, alternating with the next complexes in the correct sequence. The ES following each successive sinus complex is bigeminy, a group of three complexes separated by a compensatory pause is trigeminy (Fig. 7), of four complexes is quadrigeminy, etc.
According to the frequency during auscultation, ES is divided into rare (up to 5–9 per minute), medium frequency (from 10 to 15 per minute), and frequent (more than 15 per minute). According to Holter monitoring, extrasystoles with an occurrence rate of more than 600 per hour or more than 15,000 per 24 hours are considered frequent.
The circadian rhythm (type) of ES is diagnosed depending on the period of the day. There are three circadian types of ES: daytime, nighttime and mixed (Fig. 8). In the daytime type, ES are recorded during wakefulness, and disappear at night during sleep; at night - appear after falling asleep.
All ES of vegetative origin can be divided into three pathogenetic variants:
1. Labile resting ES (vago-dependent).
2. Stable resting ES (combination-dependent).
3. ES tension (sympathetic-dependent).
Labile resting ES are most common (47.5%), usually in children of the older age group; they are associated with increased activity of the vagus nerve. In this case, ES can be frequent, allorhythmic, group, and detected in clino- and orthoposition during the day.
Stable resting ES are most typical for children of the younger age group, as well as for schoolchildren with a mixed type of VSD and with a vagotonic initial autonomic tone. Such ES are heard and recorded on the ECG regardless of body position and physical activity, that is, there is a stable persistence of frequent ES (usually allorhythmic) in the sphenoid and orthoposition, as well as during the day (sleep and active wakefulness).
ES tensions are more often recorded in children during puberty and are characterized by an increase in orthoposition, their predominance during active wakefulness, including physical activity, and a decrease or complete disappearance during night sleep. A peculiarity of these ES is their appearance or persistence against the background of sinus tachycardia.
Modern methods of examining children with extrasystole
In terms of their physical development, children with extrasystole do not differ from their peers. Therefore, the clinical assessment of extrasystole must be carried out comprehensively, with an analysis of complaints, anamnesis, the state of the cardiovascular, central and autonomic nervous systems, which is important for classification, identification of genesis, assessment of prognosis, drawing up an individual treatment and rehabilitation program, and evaluation of its effectiveness. Mandatory are:
— assessment of clinical, anamnestic and genealogical data;
— assessment of vegetative status;
- standard electrocardiography;
— Holter monitoring with psychological, physical and medicinal stress tests;
— tests with dosed physical activity (treadmill test, bicycle ergometry);
— Doppler echocardiographic examination;
- study of the level of blood electrolytes, thyroid hormones; according to indications - MB-fraction of creatine kinase, troponin T, brain natriuretic peptide;
— examination for intracellular infections;
— neurophysiological study and assessment of neurotrophic function;
— transesophageal electrocardiography;
The main method of instrumental diagnosis of cardiac arrhythmias is electrocardiography, which does not lose its significance over time. The relationship and dynamics of the main components of the electrocardiogram provides the clinician with significant diagnostic information about the bioelectrical activity of the myocardium, the presence and characteristics of arrhythmia.
Holter monitoring - long-term recording of an ECG using portable cardiac monitors in conditions of free activity of the subject, followed by interpretation of the recording using special automatic analyzing systems - is the leading method of examining children with ES.
Indications for Holter monitoring in children with ES are:
— detection of cardiac arrhythmias in patients with other pathologies in which there is a high risk of developing arrhythmia (cardiomyopathy, MVP with regurgitation, primary pulmonary hypertension, congenital heart defects);
— assessment of the frequency and complexity of ES in the daily cycle;
— determination of the circadian rhythm of arrhythmia, the connection of ES with loads, subjective sensations;
— assessment of the effectiveness of antiarrhythmic therapy.
An important characteristic of extrasystoles caused by autonomic dysfunction is a decrease in the frequency of extrasystoles in the ortho position, during physical activity (treadmill test, bicycle ergometry), during a test with atropine, which confirms the dependence of arrhythmia on the state of the parasympathetic department of the ANS (labile resting extrasystoles). When using 24-hour heart rate monitoring, there is a clear connection between the frequency of extrasystoles and the functional states of the child’s body - a decrease in extrasystoles during the period of maximum activity and play; increased frequency - during a period of relative rest, in the deep stages of sleep.
When assessing the vegetative status in children with extrasystole, as a rule, there is a predominance of the parasympathetic department - vagotonia - or there is dystonia with a predominance of vagotonic signs (marbling of the skin, increased sweating, diffuse, red, raised dermographism, etc.). These children often suffer from vestibulopathy, increased weather dependence and meteotropism. They have other viscerovegetative manifestations - nocturnal enuresis, dyskinesia of the gastrointestinal tract and/or biliary tract, gastroesophageal reflux, etc.
Carrying out Doppler echocardiography in patients with ES is necessary to monitor the state of central hemodynamics, changes in which in the form of a decrease in ejection fraction, the appearance and progression of dilatation of the heart cavities are considered a sign of the development of arrhythmogenic cardiopathy and an indication for interventional treatment.
A study of the central nervous system of children with extrasystole, as a rule, reveals mild residual symptoms in the form of individual microorganic signs. Their combination with hypertensive-hydrocephalic syndrome, diagnosed by craniograms and echoencephaloscopy, indicates the residual nature of organic cerebral insufficiency, in most cases the result of an unfavorable course of pregnancy and/or childbirth. There is no local epileptic activity on the electroencephalogram in patients with extrasystole.
According to our observations, the psychological status of this category of patients was characterized by moderately severe anxiety and depressive disorders, and a hypochondriacal fixation on their own health. Despite emotional lability and a high level of neuroticism, children with extrasystole did well in school, and the number of interpersonal conflicts they had was less than with other types of arrhythmias.
According to indications, in a specialized hospital, patients with ES are treated with special research methods: surface ECG mapping (for topical diagnosis of rhythm disturbances), transesophageal electrocardiography. In a non-invasive electrophysiological study, due to the maximum proximity of the electrodes to the left atrium, high-amplitude atrial potentials are recorded. This makes it possible, without resorting to the complex and dangerous method of intracavitary ECG, to study the electrical potential of the atrial complex for diagnostic purposes.
Principles of treatment of extrasystole in children
The issues of treating extrasystole have not been sufficiently developed to date; there is a lot of controversy in them, probably due to different assessments of the degree of organic “interest” of the heart during extrasystole. It is necessary to use all opportunities to make an etiological diagnosis.
The presence of structural changes in the heart, somatic pathology, which could cause arrhythmia, require treatment of the underlying disease.
Children with rare ventricular extrasystoles usually do not require treatment. It is important to dynamically monitor patients at least once a year, and in the presence of clinical symptoms of ES, Holter monitoring is recommended once a year due to evidence of the persistence or transformation of ES into another cardiovascular pathology in subsequent age periods according to the Framingham study.
It is important to explain to the patient that extrasystole is safe, especially when potentially significant arrhythmogenic factors are eliminated: psycho-emotional stress, disruption of the daily routine, bad habits (smoking, alcohol, substance abuse), and taking sympathomimetic drugs. A healthy lifestyle is of great importance: getting enough sleep, walking in the fresh air, creating a favorable psychological climate in the family and school. Food should contain foods rich in potassium, magnesium (apricots, prunes, baked potatoes, dried fruits), selenium (olive oil, seafood, herring, olives, legumes, nuts, buckwheat and oatmeal, lard) and vitamins.
In children in the neonatal period, in the absence of organic heart pathology, extrasystoles more often occur in the presence of pre- or postnatal hypoxia. Of particular importance is feeding the baby with breast milk containing sufficient amounts of vitamins, minerals, polyunsaturated fatty acids, including omega-3, omega-6. In the absence of breastfeeding, it is necessary from birth to use highly adapted nutritional mixtures containing vital vitamins, minerals, and micronutrients.
Children with labile resting ES and infrequent stable resting ES do not need to be exempted from physical education lessons. The decision on physical activity for children with frequent stable ES at rest and ES of tension is decided individually depending on the results of stress tests.
With vegetative-dependent ES in pediatric arrhythmology, basic therapy is traditionally used, the purpose of which is to correct and normalize cardiocerebral interactions, neurovegetative disorders and restore the regulatory function of the sympathoadrenal system (Belokon N.A., Shkolnikova M.A. 1986). These regimens include nootropic drugs, membrane stabilizing and metabolic agents. When prescribing basic therapy, the course of treatment should be 3 months at least 2 times a year. No more than three drugs from different groups are prescribed at the same time.
Nootropic and nootropic-like drugs have a trophic effect on autonomic regulation centers, enhance the metabolic activity of cells, mobilize energy reserves of cells, regulate cortical-subcortical relationships, have a mild and persistent stimulating effect on the sympathetic regulation of the heart (peripheral sympathomimetic effect), participate in the activation of the serotonergic system .
Noofen: 100 mg 2 times a day (up to 3–4 years); 100 mg 2–3 times a day (up to 6 years); 100 mg 3–4 times a day (up to 10 years); 200 mg 2–3 times a day (up to 14 years); 250–500 mg 3 times a day (over 14 years).
Aminalon: 50 mg - 1/2 t. 2 times a day (up to 7 years); 1 t. 2–3 times per day (over 7 years).
Glutamic acid: 50 mg 2 times a day (up to 3 years); 125 mg 2–3 times a day (up to 7 years); 250 mg 3 times a day (up to 12 years); 500 mg 2 times a day (over 12 years).
Encephabol: 25 mg 2 times a day (up to 3 years); 50 mg 2 times a day (up to 7 years); 100 mg 2–3 times a day (over 7 years).
Semax 0.1% solution (nasal drops): 1 drop. 2 times per day in each nasal passage (up to 3 years); 2 drops 2 times a day (up to 7 years); 3 drops 2 times a day (up to 10 years); 5 drops 2 times a day (over 10 years old).
Pantogam: 50 mg 2 times a day (up to 3 years); 125 mg 2 times a day (up to 7 years); 250 mg 2 times a day (up to 10 years); 500 mg 2 times a day (over 10 years).
They have a sedative, anxiolytic effect:
Neurovitan: 1/4–1/2 tablet. 1 payday (from 1 to 3 years); 1 table 1 day (from 3 to 7 years); 1 table 1–3 times per day (from 8 to 14 years); 1 table 1–4 days a day (over 14 years old).
Phenibut: 50 mg twice a day (up to 3 years); 125 mg 2 times a day (up to 7 years); 250 mg 2 times a day (up to 10 years); 250 mg 3 times a day (over 10 years).
Picamilon: 10 mg 2 times a day (up to 3 years); 20 mg 2 times a day (up to 7 years); 50 mg 2 times a day (up to 10 years); 50 mg 3 times a day (over 10 years).
Metabolic drugs participate in all types of metabolism and restore normal electrical activity of the myocardium:
Cardonate: 1 caps. 1 payday (from 1 to 5 years); 1 caps. 2 times a day (from 5 to 15 years); 1–2 caps. 3 times a day (over 15 years old).
Carnitine chloride 20% solution: 4-10 drops 3 times a day (up to 1 year); 14 drops 2–3 times a day (from 1 to 6 years); 28–42 drops 2–3 times a day (from 6 to 12 years); 0.5–2.0 teaspoon 2 times a day (over 12 years).
Kudesan (coenzyme Q10): 4–10 drops 1 time per day (from 1 to 3 years); 10–16 drops 1 time per day (from 3 to 7 years); 16–20 drops 1 time per day (from 7 to 12 years); 20–60 drops 1 time per day (over 12 years).
Mildronate: 250 mg 2 times a day (up to 12 years); 250–500 mg 2 times a day (over 12 years).
Potassium and magnesium preparations affect metabolic processes, have their own antiarrhythmic effect and potentiate the effect of other antiarrhythmic drugs:
Magne B6: 10–30 mg/kg/day in 3 divided doses (from 1 to 6 years); 2–6 tables (1–3 amp.) 3 times a day (from 6 to 12 years); 6–8 tables (3–4 amps.) 3 times a day (over 12 years old).
Panangin: 1–2 tables. 3 times a day
Asparkam: 1–2 tablets. 3 times a day
Rhythmocore: 1 caps. 3 times a day (from 6 to 12 years); 1–2 caps. 3–4 days a day (over 12 years old).
If a child has feelings of disturbed rhythm and a decrease in quality of life, rational psychotherapy, sedatives, tranquilizers or antidepressants are indicated.
With frequent idiopathic ventricular extrasystole, it is necessary to monitor the well-being and state of central hemodynamics, changes in which are an indication for interventional treatment.
During radiofrequency catheter ablation (RFA), a special electrode is inserted into the heart cavity through large vessels, the distal pole of which is installed in the area of localization of the electrophysiological substrate of arrhythmia, which is responsible for its occurrence and/or maintenance. Applications of radiofrequency current are applied to the “zone of interest”. As a result of myocardial damage, the key zone of extrasystole is destroyed, which makes it impossible for it to occur. RFA of an ectopic focus is indicated for children with frequent ventricular extrasystoles (more than 15,000 ventricular extrasystoles per day), accompanied by the development of arrhythmogenic myocardial dysfunction: the appearance and increase of dilatation of the heart cavities, a decrease in the ejection fraction. In children, it is important to use the most gentle radiofrequency protocol possible.
In the immediate postoperative period, a control echocardiographic study and Holter monitoring are recommended. The effectiveness of RFA of ventricular ES is, according to various authors, from 83 to 100% and depends on the type of arrhythmia, technical capabilities and experience of the clinic.
Antiarrhythmic therapy in children has significant limitations and is justified only in order to prevent the development of arrhythmogenic myocardial dysfunction and when clinical manifestations appear due to the hemodynamic ineffectiveness of ES. Antiarrhythmic therapy with a course duration of 3–6 months. should be prescribed to children only if there are existing restrictions (most often age-related) or the impossibility of radical treatment - catheter ablation of the electrophysiological substrate of ES.
The choice of antiarrhythmic drugs remains empirical. For ventricular ES, the following drugs are most effective:
- amiodarone 5-7-10 mg/kg/day (in children under 1 year of age - up to 15 mg/kg/day);
— rhythmonorm (propafenone, propanorm) 10–15 mg/kg/day;
— atenolol 0.5–1.0 mg/kg/day;
— concor 0.1–0.2 mg/kg/day.
In children with frequent extrasystole, the effectiveness of the anticonvulsant drug carbamazepine (finlepsin), which has anti-affective and membrane-stabilizing properties, as well as antiarrhythmic activity due to inactivation of the incoming sodium current, has been described. The drug is prescribed at a dose of 7–10 mg/kg/day (up to 15 mg/kg/day in children under 1 year), divided into 2–3 doses, for a long time (up to 12 months).
It has been established that for the supraventricular form of extrasystole, class IV antiarrhythmic drugs—calcium ion transport inhibitors—are effective. The most commonly used in arrhythmology is isoptin (verapamil, finoptin). The drug is prescribed to children at a dose of 0.002 g/kg body weight per day in 4 divided doses.
In the simultaneous presence of supraventricular and ventricular ES, a more rational drug is sotalol (Sotalex) 1–2 mg/kg/day.
The selection of antiarrhythmic drugs is carried out under the control of ECG data and Holter monitoring, taking into account saturation doses and the circadian nature of the arrhythmia. It is advisable to calculate the maximum therapeutic effect of a medicinal substance taking into account what periods of the day the ventricular extrasystole is most pronounced. The exception is long-acting drugs and amiodarone.
Antiarrhythmic therapy is considered effective if the number of ventricular extrasystoles per day decreases by more than 50%, and the number of paired extrasystoles by at least 90%. The effectiveness of treatment is also assessed by parameters of intracardiac hemodynamics according to echocardiography in sinus rhythm and in extrasystolic complexes.
Treatment of the disease
If the results of the diagnostics revealed only single heart contractions that do not bring any pain or discomfort to the child, then treatment of extrasystole in children is not carried out.
If a lot of extraordinary contractions are recorded, then there is a need for therapy prescribed by a cardiologist and neurologist.
In this case, doctors can prescribe:
- modern nootropic drugs to calm the nervous system;
- metabolic agents to eliminate tissue hypoxia and normalize metabolism;
- drugs to improve the functioning of the heart muscle.
The dosage and method of taking medications is determined individually for each case. The course of treatment is 3 months at least twice a year.
In the presence of pathological extrasystole in children, the cardiologist prescribes:
- antiarrhythmic therapy;
- taking complex vitamins;
- psychotherapy.
The patient is temporarily suspended from physical education and sports in general if a direct relationship between loads or extraordinary heart contractions is revealed.