Photo: courtesy of the CELT clinic.
Our heart is constantly working: in an adult, it pumps about 10,000 liters of blood per day. In addition, our “fiery engine” is constantly under pressure: overload at work, family problems, stress, abuse... Doctors tritely call it: “heart muscle,” which we ourselves put at risk, leading to a heart attack. For many years and even decades, cardiovascular diseases have consistently led the way.
Why does our heart hurt so often and what are the ways to save it? The answer to these and other questions from our readers and his advice during the direct telephone line “MK” is given by the chief cardiologist of the Center for Endosurgery and Lithotripsy (CELT), MD. Inna Arkadyevna BESPALKO.
Causes:
- hemodynamic disturbances due to atherosclerosis of the coronary vessels;
- lack of oxygen due to a sudden and intense start to exercise;
- deficiency of magnesium and other beneficial substances;
- pathologies of the heart, stomach, intestines;
- neuralgia;
- oncological diseases.
During training, compression and the appearance of diffuse, aching, stabbing, paroxysmal pain without increasing are possible. The sensation occurs behind the sternum or in the center of the back, often radiating to the left side of the body under the shoulder blade, in the shoulder, arm or up to the neck and chin. Accompanied by deterioration of health, arrhythmia, lack of air.
Often, chest pain after training occurs late - after 1-72 hours.
With true pain in the myocardium, panic suddenly arises, fear for life, perspiration, weakness, and the person stops moving. The absence of these signs indicates physiological causes and manifestations of non-cardiac pathology.
If heart pain or discomfort occurs, you should immediately stop the load, switch to smooth movements and restore breathing.
Why is pain during exercise dangerous?
Correctly selected physical exercises are one of the methods for preventing diseases of the cardiovascular system. However, there are conditions when even a slight load causes pain in the heart when playing sports:
- Coronary heart disease (angina pectoris) is caused by a violation of blood transport to the myocardium through the narrowed lumen of the coronary vessels. This disease develops in people with atherosclerosis. An attack of pain is characterized by retrosternal localization, radiation to the left arm and shortness of breath.
The problem of symptoms in athletes is associated with increased myocardial mass, which leads to increased nutrient requirements. During intense exercise, the need for an adequate supply of oxygen increases, causing a vicious cycle.
- Hypertrophic cardiomyopathy is a non-inflammatory lesion of the myocardial muscle mass, which is characterized by an increase in the number of fibers with a decrease in the volume of the heart chambers, resulting in a decrease in the amount of ejected blood.
- Uncontrolled use of hormonal and anabolic drugs . Heart pain after bodybuilding is often associated with the intake of proteins and testosterone, which help build skeletal muscle. However, the use of uncertified products in unregulated doses is accompanied by a delay in the development of internal organs, especially the heart, which does not have time to adapt to ensure sufficient blood supply.
In addition, a significant increase in the volume of the heart cavities develops arrhythmia and congestion in the chambers with the formation of a blood clot. Such processes lead to thromboembolism - blockage of the lumen of a vessel with a blood clot, which requires urgent treatment.
Preventing chest pain
Before starting training, it is recommended to find out your level of physical fitness.
Suitable for this purpose:
- endurance test using squats;
- Ruffier index;
- shoulder muscle strength and endurance test;
- Robinson index;
- reactions of the autonomic nervous system to increased physical activity.
Based on the test results, a training program is selected. If chest pain appears during or after exercise, you need to identify the trigger. This provocateur is excluded (for example, the degree of stress is reduced).
Angina pectoris
Angina pectoris is one of the most common forms of coronary heart disease (CHD). The disease manifests itself as pain in the chest (in the middle of the chest) when walking (especially in cold or windy weather), climbing stairs, as well as other physical and emotional stress, against a background of increased blood pressure. The pain is compressive in nature (that’s why angina pectoris was previously called “angina pectoris”), pressing or burning, radiating to the left arm or both arms, or to the lower jaw. The pain is often accompanied by shortness of breath, sweating, and weakness. When you stop or stop exercising, the pain behind the sternum quickly (in 3-5 minutes) goes away.
For stable angina pectoris, the repetition of pain in the chest during the same physical activity is typical; the pain is of the same nature and quickly disappears when the exercise is stopped or nitroglycerin is taken under the tongue. Often, patients know that an attack occurs precisely when going outside in cold weather, accelerating their pace, climbing a mountain, and they can even say exactly when walking what distance (for example, after 100-200 meters) the pain appears.
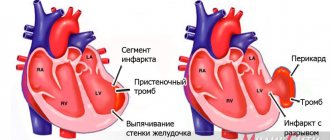
If pain behind the sternum occurs more often, becomes more intense, prolonged (lasting more than 10-15 minutes), provoked by less stress and occurs even at rest (including at night), their character changes (especially if the pain becomes burning or tearing, sensation “cola behind the sternum”) and are no longer quickly relieved by nitroglycerin, then these are symptoms of unstable angina. When an attack of angina pectoris lasts more than 20-30 minutes, the death of myocardial cells begins, that is, myocardial infarction is likely. In the acute period of myocardial infarction, there is a high risk of life-threatening complications (ventricular fibrillation, i.e. cardiac arrest, heart block, heart rupture). Therefore, if the chest pain cannot be relieved within 15-20 minutes, then you should immediately call an ambulance, which will take you to a specially equipped cardiac intensive care unit, where observation and treatment will reduce the likelihood of myocardial infarction and its complications.
Why does chest pain occur?
To understand what coronary heart disease is and angina pectoris as the most common form of this disease, you need to remember your school biology textbook. In a simplified form, the development of this disease can be represented as follows.
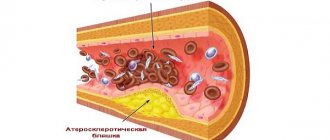
If you remember, all living organisms, unlike inanimate nature, move. The organisms themselves, their body parts, stomach and intestines move, blood moves through the vessels. Movement requires energy. Energy in cells is produced through oxidation (this complex process can be very loosely called “internal combustion”). Oxidation requires oxygen. The simplest organisms (amoebas, bacteria, etc.) receive oxygen directly through the cell membrane. In complex organisms, there is a delivery system: in the lungs, oxygen is absorbed into the blood and distributed through the vessels to all organs and tissues. The vessels through which oxygenated blood flows are called arteries. Accordingly, there are arteries in all organs. The arteries that supply blood to the heart are called coronary or coronary arteries (by the way, this is why coronary heart disease is also called coronary heart disease (CHD) in English transcription). Normally, the lumen of the artery is sufficient to ensure the flow of the required amount of blood through it to the part of the heart to which it supplies blood. In addition, when the demand for oxygen increases (for example, when running), due to the elasticity of the wall, a healthy coronary artery can expand (this is called coronary reserve). With atherosclerosis (and ischemic heart disease is a type of this process) under The lining of the coronary arteries deposits cholesterol in the form of plaques. As a result, the lumen of the arteries in these areas narrows (just as the lumen of water pipes narrows in areas where rust and scale are deposited). In addition, calcium penetrates into the plaques and these areas are “cemented” and lose elasticity.As a result, the lumen of the coronary arteries narrows and the coronary reserve decreases. This process can last for years and not manifest itself in any way, because the physiological coronary reserve is quite high. But when the lumen of the artery narrows by more than 70-75%, then the oxygen supplied by the blood may not be enough (in medical terms, myocardial ischemia occurs). Naturally, this occurs primarily when the need for oxygen is greater, that is, during physical activity. In typical cases, when you speed up your pace, walk uphill, or go outside in cold weather, pain occurs behind the sternum, which quickly stops when you stop (at rest, there is still enough blood supply through the narrowed section of the artery). Pain behind the sternum is an alarm signal, a “cry of the heart” - “stop, I don’t have enough oxygen,” and therefore “enduring it courageously” is wrong and very dangerous.
How to detect angina pectoris?
If you experience chest pain described above, you should consult a cardiologist, or first, a general practitioner or family doctor. If you are a man over 40 years of age, smoke, suffer from hypertension or diabetes, and your parents had heart attacks or strokes, then it is very likely that chest pain is a symptom of angina pectoris. The disease is serious, so you need to be examined as soon as possible, temporarily postponing daily activities. Remember that if you leave this problem “for later”, hoping for “maybe”, then a myocardial infarction may occur, which often leads to death.
The diagnosis of angina is made based on an analysis of the patient's complaints and examination data. Blood lipid tests and blood coagulation parameters (coagulogram) are performed. An electrocardiogram (ECG) is recorded at rest, which may be normal if there has not been a myocardial infarction. But if you provoke an attack of angina with physical activity (stress test) on a treadmill (treadmill) or bicycle ergometer, then the ECG can reveal signs of transient myocardial ischemia. If the stress test results are positive, coronary angiography (x-ray contrast study of the coronary arteries) is indicated, which can reveal the nature of the damage to the coronary arteries (multiple or single atherosclerotic plaques, stable or not, the severity of stenoses (narrowings), their location and extent. Depending on the symptoms , the cardiologist makes a decision on the possibility of drug treatment of angina or the need for myocardial revascularization surgery - coronary angioplasty (PTCA) or coronary artery bypass grafting (CABG).
What to do if you have an angina attack?
The first thing to do when pain occurs in the chest is to stop exercising. If pain appears while walking, then you need to stop. Stopping the load itself can relieve (stop) the pain. But it is safer to take nitroglycerin under the tongue. I note that modern forms of nitroglycerin in the form of nitrospray in cans (nitromint, nitro-pol, nitrocor-spray, etc.) are more convenient in comparison with also effective tablets. There is no need to open the tube and pour the pills into the palm of your hand, take one of them, pour the rest back (and at this time there is pain in the chest, and if, in addition, the attack occurred on the street, you also need to take off and put on gloves, etc.). Nitrospray, unlike tablets, does not crumble into powder, which means that the dosage of nitroglycerin remains exactly necessary, it is protected from light and remains valid for 3 years. In short, if possible, it is more convenient and reliable to use nitro spray.
So, if there is pain in the chest, you need to:
- Stop and take one dose of nitroglycerin under the tongue (1 spray or one tablet).
- If possible, sit down. Nitroglycerin lowers blood pressure, and if the pressure drops suddenly, you may feel dizzy or even faint. That is why you should not immediately take more than 1 dose of nitroglycerin. But attention! The danger of myocardial infarction when an attack of angina is prolonged is much more serious than these possible side effects of taking nitroglycerin, which, by the way, do not always occur, just like a headache. If you previously had severe headaches while taking nitroglycerin, then to reduce them, also take 1 tablet of Validol or any other tablet containing menthol (Halls, Rondo, Chill, etc.). Attention! Taking validol alone is not reliable compared to taking nitroglycerin and you may lose valuable time to quickly relieve an attack. The same applies to taking nitrosorbide under the tongue; it begins to act only after 7-10 minutes. Nitroglycerin remains the “gold standard” for relieving angina attacks. If, when taking nitroglycerin, severe headaches or dizziness still occur, then you can reduce the single dose to relieve attacks by switching to using “Kremlin drops” or Votchal drops or using an alcohol solution of nitroglycerin (drop 1-2 drops of it onto a validol tablet and during an attack, do not take the entire tablet, but break it into 2-4 parts; however, such a “blank” cannot be stored for more than a few hours due to the rapid destruction of nitroglycerin). As a rule, chest pain is quickly relieved by taking 1 dose of nitroglycerin under the tongue.
- If the pain behind the sternum is not relieved after 3-5 minutes and there is no severe weakness or dizziness, then you need to take another dose of nitrospray or 1 tablet of nitroglycerin under the tongue. If after another 3-5 minutes the pain behind the sternum is still not relieved, then 1 dose (3rd) of nitroglycerin is taken under the tongue again.
- If after 15 minutes the chest pain is not relieved by taking nitroglycerin, then you need to call an ambulance. While waiting for the ambulance, if there is no severe weakness and dizziness, you can take 1 dose of nitroglycerin under the tongue again every 5-10 minutes and put a mustard plaster on the heart area. Considering that in such a situation myocardial infarction is likely, it is also necessary to take? aspirin tablets (250-325 mg).
Treatment of angina
If the diagnosis of angina is confirmed during examination, then treatment of this disease is necessary. The type of treatment depends primarily on whether the situation is stable or unstable. If a diagnosis of unstable angina is made, then hospitalization in a hospital is indicated; treatment of stable angina is usually possible on an outpatient basis. In case of unstable angina or severe stable angina, coronary angiography is indicated and a decision on the need for surgical treatment - myocardial revascularization operations - coronary angioplasty (PTCA) or coronary artery bypass grafting (CABG) is indicated. If possible, they limit themselves to drug treatment.
Objectives of drug treatment
- slowing the progression of atherosclerosis,
- prevention of myocardial infarction,
- reduction in the frequency of chest pain.
Unfortunately, it is impossible to completely cure atherosclerosis and ischemic heart disease (do not believe charlatans who advertise all sorts of remedies that have not been scientifically tested!), but the prognosis and quality of life can be significantly improved.
In principle, treatment of angina pectoris includes:
- Correction of risk factors for coronary artery disease. A direct connection between smoking, arterial hypertension, hyperlipidemia, and diabetes mellitus and morbidity and mortality from ischemic heart disease has been proven. It is necessary to eliminate or reduce the impact of these factors.
- Treatment of atherosclerosis. IHD is one of the forms of atherosclerosis, so strict adherence to the diet and constant lifelong use of statins (Zocor, Simgal, Liprimar, Lipostat, etc.) are necessary.
- Prevention of blood clot formation on atherosclerotic plaques. If the atherosclerotic plaque is “soft”, with a thin cover, then it can burst and a blood clot forms on it. A thrombus can block blood flow through the coronary artery and then myocardial infarction occurs (see section “Myocardial infarction”). To prevent the formation of a blood clot on an unstable plaque, all patients suffering from angina pectoris are prescribed antiplatelet drugs - aspirin (its enteric form is called thromboASS) or Plavix.
- Optimizing the working conditions of the heart. If we compare our body to a cart that rides along the road, and our heart to a horse that pulls it, then it will become clear why certain drugs are prescribed. Beta blockers (atenolol, metoprolol, concor, etc.) slow down the heart and lower blood pressure. As a result, we spare the horse (heart) so as not to drive it, and the cart travels longer. Antihypertensive drugs (calcium antagonists (nifedipine-retard, norvasc, plendil, diltiazem), ACE inhibitors (enalapril, prestarium, monopril, etc.), diuretics (indapamide (arifon), hypothiazide), etc.) reduce blood pressure if it is elevated , reducing the obstacle to the ejection of blood from the heart (improving the road along which the cart travels). Cytoprotectors (preductal) improve metabolism in the myocardium (comparable to lubrication of the axles of cart wheels). As a result, the use of drugs reduces the load on the heart, which reduces its need for oxygen and reduces the likelihood of angina attacks.
- Prevention of angina attacks. For this purpose, the beta-blockers already mentioned above are used, as well as calcium antagonists (they also dilate the coronary arteries) and long-acting nitrates (cardiquet-retard, monocinque, monomac, nitrosorbide, etc.). Nitrates are used in the minimum required doses, as needed, depending on what time of day angina attacks occur and what provokes them. So, if chest pain occurs only in the first half of the day when going outside, then Cardiquet-Retard is taken only once a day in the morning 20-30 minutes before the expected exercise. If, against the background of a selected adequate dose of beta-blockers and calcium antagonists, there is no chest pain, then taking nitrates is not indicated.
How to prevent heart pain in athletes:
- be examined by a cardiologist;
- to refuse from bad habits;
- eat well, get enough sleep;
- maintain a drinking regime (35–50 ml of water/1 kg of body weight);
- warm up before training;
- After exercise, do a cool-down appropriate for the sport;
- start with minimal loads at low intensity;
- gradually gradually increase the complexity of the program.
If the examination reveals a disease that forces you to limit sports activity, we recommend classes with a physical therapy specialist who will select an individual set of exercises and determine the intensity and degree of physical activity.
conclusions
Regular sports and bodybuilding with the correct use of dietary supplements and medications do not pose a danger to the functional state of the heart. However, due to the individual characteristics of a person, the presence of concomitant diseases and non-compliance with exercise techniques, there is a risk of aching, stabbing and burning pain in the chest.
Athletes who experience heart pain after exercise are advised to stop exercising and consult a doctor for help. Doctors, in turn, use a comprehensive approach to diagnosing the underlying cause of pain so that treatment advice is most appropriate.
Pathological athlete's heart
In the United States, they keep a special register where the death of an athlete is celebrated every third day, and mostly football players die - a kind of American football is “densely implicated” in rugby. We do not have such records, but all death cases are widely covered by the press; Russian athletes clearly die much less often. The cause of their death is, as a rule, a pathological sports heart, which is formed by unsystematic extreme loads, doping, training against the background of banal infections and, of course, genetic characteristics.
The mass and thickness of the walls of the heart in this situation are also greater than normal, but due to the lag in the growth of coronary capillaries from the increase in the myocardium itself, its nutrition is disrupted. The muscle is less elastic, so contractility suffers and, therefore, maximum relaxation at rest is impossible. The volume of not only the ventricles that eject blood increases, but also the volume of the atria that receive blood. The volume of the heart is increased, but much more than it should be - more than 1200 cubic centimeters.
Also, the heart rarely contracts, bradycardia occurs. It can be more pronounced, that is, less than 40 contractions per minute, especially at night, which leads to severe oxygen starvation of the brain. With a normal athletic heart, the athlete does not feel a slow heartbeat in any way; when bradycardia is accompanied by clinical symptoms, then this is no longer a normal adaptation of the heart to high loads, but a pathological condition. Decrease in blood pressure below 100/60 mmHg. in such a situation, it is also not an adaptation of the body, but a reaction to painful changes.
How the heart reacts to sports stress
At maximum athletic activity, the heart contracts more than two hundred times, pumping more than 30 liters of blood per minute. Trying to ease the colossal cardiac work, the body distributes blood more efficiently, reducing the resistance of the vascular walls, dilating the vessels of skeletal muscles and opening additional collateral vessels, which were previously in a collapsed state. However, even with such a significant compensatory decrease in blood flow, the heart works on the verge of beyond its capabilities.
Under the influence of loads, the heart changes its configuration - it is remodeled to ensure the viability of all organs under intense load. Morphological - biological changes correct the electrophysiology of the myocardium, that is, the emergence of an electrical potential for contraction of the heart chambers and their relaxation. In four out of ten professional athletes, the ECG recording, reflecting the electrophysiological characteristics of the heart, differs from the normal electrocardiogram in the height and depth of the waves.
Over time, but before that, at least two or three years of regular sports activities will pass, the heart will adapt to constant loads that are excessive for the normal body, so that the skeletal muscles are able to develop strength that is inaccessible to an untrained person.
Treatment of myocarditis
How to treat myocarditis after coronavirus? Nonspecific therapy aimed at treating the underlying cause is required. Antiviral and immunosuppressive drugs are used.
The use of symptomatic medications of the following drug groups is recommended:
- beta blockers
- angiotensin-converting enzyme inhibitors to lower blood pressure
- decongestants
Depending on the severity of the lesions and the patient’s condition, cardiac glycosides and antiarrhythmic drugs are also prescribed.
Medicines and dietary supplements for cardiac stress
To reduce the load on the heart and prevent its overstrain, sports pharmacology has a number of medications and dietary supplements, which can be conditionally divided into 4 main groups according to the vector of application of cardioprotection. Some of these drugs may have complex effects and be included in several groups.
1. Drugs that optimize ENERGY PROCESSES IN THE CELL.
These effects are inherent
1A. macroergic phosphates (creatine, riboxin, phosphadene, ATP-long)
1B. inhibitors of lipolytic processes (nicotinic acid, natural antioxidants ceruloplasmin and superoxide dismutase prototypes (panaxod, orgotein, peroxinorm),
1C. enzymes and electron-acceptor substances (D-ribose, cytochrome C, coenzyme Q10, L-carnitine, trimetazidine, meldonium, succinic acid (succinate)).
2. Drugs that increase the RESISTANCE OF CELL MEMBRANES. This is, in particular,
2A. phospholipids (essential), α-tocopherol (Vit.E), probucol, PUFAs (Omega-3-6), β-carotene (Vit.A))
2B. inhibitors of free radical processes (mexidol, flavin, quercetin, rutin, methionine, unithiol, epargriseovit),
2C. phospholipase blockers (cefaransine, chlorpromazine, calcium antagonists, etc.)
3. ANTIHYPOXANTS. These are the means
3A. Improving coronary blood flow and blood transport function. In particular, Arginine, Meldonium, Actovegin, Aerox Oxygen Drops
3B. Improving the processes of energy supply to the cell are the products of the mentioned group No. 1, Meldonium, Creatine, ATP-long, L-carnitine, succinic acid, etc.
4. Means for CORRECTING IONIC FLOWS. Primarily Potassium K+ and Magnesium Mg2+ ions, and the most famous drug here is Panangin (Asparkam)