When should you pay attention to your health?
Any healthy person should undergo a minimum preventive examination once a year, which includes a general blood test.
If the hemoglobin level is below 120 g/l, you should consult a physician.
Anemia with a hemoglobin level above 100 g/l is considered mild and does not pose a serious danger to the body at the time of detection, but still requires correction. If the hemoglobin level is 70-80 g/l and below, it is necessary to take urgent measures, because This condition poses serious threats to health, and sometimes life!
For the reasons for the development of anemia, the leading position is occupied by iron deficiency anemia - every 12th person in the world suffers from iron deficiency anemia, and among all anemias, iron deficiency anemia reaches 80% in frequency.
What is associated with the development of iron deficiency anemia? The reasons may be an elementary deficiency of iron in food, impaired absorption of iron in the gastrointestinal tract (for example, with gastritis with low acidity) and chronic bleeding.
Cardiovascular disease and anemia
The number of deaths from cardiovascular diseases (CVD) continues to rise worldwide. The conclusion that coronary heart disease (CHD) “... is the leading cause of death worldwide, its level is constantly growing and has now reached the proportions of a pandemic that knows no borders,” appeared on the website of the World Health Organization (WHO) in 2009 ., is perceived as increasingly relevant. In 2011, IHD caused the death of 7.3 million people [1, 2].
According to WHO estimates, 1.62 billion people suffer from anemia in the world [3]. The incidence of anemia, as well as coronary artery disease, increases significantly with age. More than 10% of people over 65 years of age and up to 50% of elderly patients with chronic diseases living in nursing homes have signs of anemia [4].
In the practice of general practitioners and cardiologists, a combination of cardiovascular pathology and anemia is often encountered. Anemia is detected in 25–40% of patients with chronic heart failure (CHF) and 10–20% of patients with coronary artery disease [5–7].
European and American recommendations for the management of patients with stable angina, issued in the last two years, require mandatory determination of hemoglobin levels in all patients and consider anemia as a factor provoking coronary insufficiency [8, 9]. In the latest recommendations for the diagnosis and treatment of patients with CHF, American and European experts note that anemia not only increases the symptoms of CHF, worsens the quality of life of patients, reduces exercise tolerance, and can cause the development of acute decompensation of CHF and an increase in the frequency of hospitalizations, but also an independent negative predictor of prognosis [10, 11]. The risk of death in CHF in patients with anemia is twice as high as without it, even when taking into account additional variables (renal dysfunction, severity of CHF, and others) [13]. Already latent iron deficiency can have a negative impact on the prognosis of CHF [14], which makes it advisable to determine its markers in all patients with CHF.
In acute coronary syndrome, the presence of anemia can quadruple the likelihood of death in patients and is considered an independent predictor of the risk of adverse clinical outcomes [15, 16]. Even chest pain syndrome in women, when combined with anemia, turns out to have a more unfavorable prognosis (the risk of death doubles) [17].
Preoperative anemia during cardiac surgery determines a high risk of subsequent blood transfusion and worse treatment results, which makes the task of early detection of anemia and high-quality, timely treatment urgent [18].
The role of anemia as an independent risk factor for poor prognosis in atrial fibrillation in elderly and senile people has been proven [19].
As shown by the analysis of the effect of the combination of anemia and impaired renal function on coronary artery disease in the population-based ARIC study (The Atherosclerosis Risk in Communities Study), anemia occurs in individuals with a slight and moderate decrease in renal function much more often than expected. And the combination of anemia and renal dysfunction significantly increases the risk of developing coronary artery disease, even after taking into account known risk factors such as diabetes mellitus, blood lipid levels, blood pressure and the use of antihypertensive therapy. The findings highlight the need for timely identification and treatment of anemia to improve patient prognosis [20].
The unfavorable mutual influence of CHF, anemia and renal dysfunction gave rise to the identification of new syndromes: “cardiorenal anemia syndrome”, “cardiorenal iron deficiency syndrome” and even “cardiorenal anemia and iron deficiency syndrome”. The latter terms emphasize the importance of iron deficiency as an independent risk factor for poor prognosis in CHF. The possibility of a direct effect of iron deficiency on diastolic function, hypertrophy, fibrosis and dilatation of the myocardium, the level of circulating erythropoietin, molecular signaling pathways and activation of inflammation has been proven in animal experiments [21]. This wide range of negative effects of iron deficiency is likely related to the role of iron in the body. It is not only part of hemoglobin and myoglobin, but is also found in enzymes involved in the conversion of adenosine triphosphate into adenosine diphosphate, promotes electron transport in mitochondrial chains, determines tissue metabolism and the absorption of free radicals [19]. Iron is involved in immune reactions and is necessary for the myelination of nerve fibers and DNA synthesis [22, 23].
Anemia in people with cardiovascular disease may have the same etiological factors as in the general population. An additional role in the development of anemia in cardiovascular pathology may be played by the older age of patients, which is itself associated with a lower hemoglobin value, the increasing incidence of chronic kidney disease, and the high prevalence of diabetes mellitus. It is assumed that the development of anemia in pathology of the cardiovascular system is contributed by: a chronic inflammatory process (increased synthesis of pro-inflammatory cytokines - tumor necrosis factor alpha, interleukin-6), ischemic depression of bone marrow hematopoiesis, decreased synthesis of endogenous erythropoietin due to renal dysfunction. In CHF, hemodilution with sodium and water retention and impaired absorption of iron and vitamins in the intestine may play a role in the formation of anemia. An additional factor for the development of anemia may be ongoing drug therapy that causes blood loss (when taking Aspirin, anticoagulants), a decrease in the production of erythropoietin and the sensitivity of the bone marrow to it (when using blockers of the renin-angiotensin-aldosterone system), etc.
The relevance of the issue of early diagnosis of anemia in patients with cardiovascular pathology is determined by the fact that its late detection leads to a delay or absence of the necessary intervention in relation to a potentially correctable condition.
A significant proportion of patients with cardiovascular pathology have latent iron deficiency, or iron deficiency anemia (IDA) or a combination of these conditions with other types of anemia.
Clinical signs of IDA consist of anemic and sideropenic syndromes, the latter is also determined by iron deficiency. Anemic syndrome may include the following manifestations: weakness, dizziness, syncope and orthostatic conditions, memory loss, epileptic seizures, symptoms of coronary insufficiency (anginal pain, repolarization disturbances on the ECG, arrhythmias), symptoms of myocardial insufficiency, systolic murmur on auscultation of the heart. Sideropenic syndrome leads to multiple disorders of various organs and systems. Lesions due to iron deficiency in the skin, skin appendages and mucous membranes (dryness, damage to hair and nails, etc.) are well known. No less common manifestations are symptoms from the gastrointestinal tract (decreased and perverted appetite, dysphagia, constipation or diarrhea, glossitis, burning tongue, esophagitis, dystrophic changes in the cells of the gastric mucosa); nervous system (increased fatigue, tinnitus, dizziness, headaches, decreased intellectual capabilities); cardiovascular system (tachycardia, diastolic dysfunction); urinary system (dysuria and urinary incontinence when coughing, laughing, nocturnal enuresis).
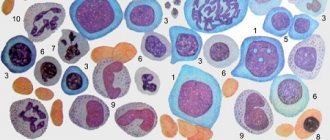
In the laboratory diagnosis of chronic IDA, microscopy of a peripheral blood smear reveals microcytic hypochromic anemia with hypoproliferation of reticulocytes. To confirm iron deficiency, reduced serum iron and ferritin levels are required.
Treatment of IDA is aimed at treating the disease underlying iron deficiency and actually compensating for iron deficiency.
Although patients with IDA need dietary advice, it is important to clearly explain that diet is not the basis of therapy. The largest amount of iron is found in meat (heme iron). All other foods contain less iron, and, most importantly, much less of them is absorbed (1–5% from apples, 10–15% from eggs and fish, and 25–30% from meat).
In drug therapy for IDA, the main focus has been and remains the use of iron supplements. The choice of iron drug is determined by its effectiveness (the amount and bioavailability of the iron it contains) and tolerability. An intake of 100 to 300 mg of elemental iron per day is required. The use of higher doses does not make sense, since iron absorption does not increase. Iron preparations on the domestic market are represented by hydroxypolymaltose complex, iron sorbitol complex, protein iron succinylate, iron sucrose complex. For patients with cardiac pathology, it is extremely important when carrying out additional drug therapy for IDA, in addition to high efficiency, the absence of negative drug interactions and good tolerability of the drug. The drug Maltofer, a polymaltose complex of iron sulfate (III), meets these requirements. Maltofer is a non-ionic iron preparation. Its absorption is ensured by active transport, without preliminary dissociation in the intestine, which eliminates the irritating effect on the mucous membrane and avoids most of the undesirable reactions from the gastrointestinal tract typical of ionized iron preparations [25, 26]. Maltofer does not interact with food or other medications, and the release form in the form of chewable tablets allows it to be used at any time and in any setting [27–30]. At the same time, the absorption of iron from other iron supplements may be reduced under the influence of substances contained in some foods - phytins (rice, soy), phosphates (fish, seafood), tannin (tea, coffee), while taking a number of medications (tetracyclines, antacids, calcium and magnesium salts), which requires taking these medications taking into account the time of consumption of food and these medications. Iron salt preparations contain divalent iron, which, after entering the blood, is converted into trivalent iron for its subsequent inclusion in the hemoglobin molecule, which can be accompanied by the formation of free radicals and have a negative effect on physiological processes in various organs and tissues [31]. Maltofer contains ferric iron, which is directly used to build the hemoglobin molecule, and therefore does not have a pro-oxidant effect [32]. When using iron supplements in adequate doses, a subjective improvement in well-being may be noted within a few days. The first objective criterion - reticulocyte crisis (an increase in the number of reticulocytes by 2-10 times compared to the initial one) is observed by the end of the first week of therapy. The absence of reticulocyte crisis indicates either an inadequate dose of the drug or an erroneous prescription of the drug. An increase in hemoglobin levels and the number of red blood cells is observed in the third week of therapy. After normalization of hemoglobin levels, a half dose of iron supplement is recommended for another 4–8 weeks to saturate the iron depot.
In 2013, the first recommendations for the treatment of anemia in patients with cardiovascular pathology were issued by the American College of Physicians [20]. They generally determine the tactics of managing a patient with cardiac pathology and anemia, regardless of its etiology. Three treatment strategies are considered: the use of erythropoietin-stimulating agents, red blood cell transfusion, and replenishment of iron deficiency. It is emphasized that red blood cell transfusion does not provide benefit and can cause harm to patients, so it is only possible in hospitalized severe patients with coronary artery disease with severe anemia. The use of erythropoietin-stimulating drugs for mild and moderate anemia in patients with CHF and coronary artery disease is not recommended due to the potential risk of thromboembolic complications and the lack of effect of therapy on the prognosis and frequency of hospitalizations. Positive data are currently available for the strategy of replenishing iron deficiency with intravenous administration of iron carboxymaltose; this tactic improves exercise tolerance, quality of life, reduces mortality and the frequency of hospitalizations [33].
Thus, anemia is a common comorbidity in cardiovascular diseases. Today in cardiology it is assessed as an independent predictor of the risk of adverse clinical outcomes, therefore patients with cardiovascular pathology need timely diagnosis of anemia in order to carry out adequate therapy.
Literature
- World Health Organization Cardiovascular diseases // Information bulletin No. 317. March 2013 [Electronic resource] - Access mode: https://www.who.int/mediacentre/factsheets/fs317/ru/ [Date of access: 10.04. 2014].
- World Health Organization 10 leading causes of death in the world // Information bulletin No. 310. July 2013 [Electronic resource] - Access mode: https://www.who.int/mediacentre/factsheets/fs310/ru/ [Access date: 04/10/2014].
- Worldwide prevalence of anemia 1993–2005. WHO Global Database on Anaemia. [Electronic resource] - Access mode: https://whqlibdoc.who.int/publications/2008/9789241596657_eng.pdf [Access date: 04/10/2014].
- Bross M.H., Soch K., Smith-Knuppel T. Anemia in older persons // Am Fam Physician. 2010. Sep 1; 82(5). P. 480–487.
- Boyd CM, Leff B, Wolff JL et al. Informing clinical practice guideline development and implementation: prevalence of coexisting conditions among adults with coronary heart disease // J Am Geriatr Soc. 2011. 59. P. 797–805.
- Felker GM, Adams KF Jr., Gattis WA et al. Anemia as a risk factor and therapeutic target in heart failure // J Am Coll Cardiol. 2004. 44. P. 959–966.
- Malyszko J., Bachorzewska-Gajewska H., Malyszko J. et al. Prevalence of chronic kidney disease and anemia in patients with coronary artery disease with normal serum creatinine undergoing percutaneous coronary interventions: relation to New York Heart Association class // Isr Med Assoc J. 2010. 12. P. 489–493.
- Stable Coronary Artery Disease (Management of). ESC Clinical Practice Guidelines. [Electronic resource] - Access mode: https://www.escardio.org/GUIDELINES-SURVEYS/ESC-GUIDELINES/Pages/GuidelinesList.aspx [Access date: 04/10/2014].
- Fihn SD, Cardin JM, Abrams J. et al. 2012 ACCF/AHA/ACP/FCP/AATS/PCNA/SCAI/ SNS Guideline for the Diagnosis and Management of Patients With Stable Ischemic Heart Disease // J. Am. Coll. Cardiol. 2012. Vol. 60. No. 24. P. e44-e164.
- 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. [Electronic resource] - Access mode: https://circ.ahajournals.org/content/128/16/e240.extract [Access date: 04/10/2014].
- Acute and Chronic Heart Failure. ESC Clinical Practice Guidelines. [Electronic resource] - Access mode: https://www.escardio.org/GUIDELINES-SURVEYS/ESC-GUIDELINES/Pages/GuidelinesList.aspx [Access date: 04/10/2014].
- Groenveld HF, Januzzi JL, Damman K. et al. Anemia and mortality in heartfailure patients a systematic review and metaanalysis // J Am Coll Cardiol. 2008. 52 (10). P. 818–827.
- Jankowska E.A., Rozentryt P., Witkowska A. et al. Iron deficiency: an ominous sign in patients with systolic chronic heart failure // Eur Heart J. 2010. 31 (15). P. 1872–1880.
- Meneveau N., Schiele F., Seronde MF et al. Anemia for Risk Assessment of Patients With Acute Coronary Syndromes // Am J Cardiol. 2009. Feb 15; 103(4). P. 442–447.
- Hasin T., Sorkin A., Markiewicz W. et al. Prevalence and Prognostic Significance of Transient, Persistent, and New-Onset Anemia After Acute Myocardial Infarction // Am J Cardiol. 2009. Aug 15; 104(4). P. 486–491.
- Arant C., Wessel T., Olson M. et al. Hemoglobin Level Is an Independent Predictor for Adverse Cardiovascular Outcomes in Women Undergoing Evaluation for Chest Pain. Results From the National Heart, Lung, and Blood Institute Women's Ischemia Syndrome Evaluation Study // J Am Coll Cardiol. 2004. 2, Jun 2; 43 (11). P. 2009–2014.
- Muñoz M, Ariza D, Gómez-RamÍrez S et al. Preoperative Anemia in Elective Cardiac Surgery: Prevalence, Risk Factors, and Influence on Postoperative Outcome // Transfusion Alternatives in Transfusion Medicine. 2010. 11 (2). P. 47–56.
- Sharma S., Gage B.F., Deych E. et al. Anemia: an independent predictor of death and hospitalizations among elderly patients with atrial fibrillation // Am Heart J. 2009. Jun; 157(6). P. 1057–1063.
- Astor B.C., Coresh J., Heiss G. et al. Kidney function and anemia as risk factors for coronary heart disease and mortality: the Atherosclerosis Risk in Communities (ARIC) Study // Am Heart J. 2006. Feb; 151(2). P. 492–500.
- Naito Y., Tsujino T., Matsumoto M. et al. Adaptive response of the heart to long-term anemia induced by iron deficiency // Am J Physiol Heart Circ Physiol. 2009. 296. P. 585–593.
- Ordway AG, Garry DJ Myoglobin: an essential hemoprotein in striated muscle // J Exp Biol. 2004. 20; 7. P. 3441–3446.
- Arredondo M., NbСеz MT Iron and copper metabolism // Mol Aspects Med. 2005. 26. P. 313–327.
- Ortiz E., Pasquini JM, Thompson K., Felt B. et al. Effect of manipulation of iron storage, transport, or availability on myelin composition and brain iron content in three different animal models // J Neurosci Res. 2004. 77. P. 681–689.
- Treatment of anemia in patients with heart disease: A clinical practice guideline from the American college of physicians // Annals of Internal Medicine. [Electronic resource] - Access mode: https://annals.org/article.aspx?articleid=1784292 [Access date: 04/10/2014].
- Geisser P., Muller A. Pharmacokinetics of iron salts and ferric hydroxide carbohydrate complexes // Drug Research 1987. 37. P. 100–104.
- Pestaner JP, Ishak KG, Mullick FG, Centeno JA Ferrous Sulfate toxicity. A review of autopsy findings // Biol Trace Elem Res. 1999. 69 (3). P. 191–198.
- Andrade JVD, Rodrigues PPB, Fontoura IB et al. Tratamento da anemia ferropriva com hidroxido de ferro polimaltosado - Estudo multicêntrico comparativo entre tratamento ministrado com e sem alimentação concomitante // Arq bras Med (Suppl). 1992. 66. P. 253–258.
- Funk F., Canclini C., Geisser P. Interactions between iron (III)-hydroxide polymaltose complex and commonly used medications. Laboratory studies in rats // Arzneimittel-Forschung (Drug Research). 2007. 57 (6 a). P. 370–375.
- Potgieter MA, Potgieter JH, Venter C., Venter JL, Geisser P. Effect of oral tetracycline on iron absorption from iron (III)-hydroxide polymaltose complex in patients with iron deficiency anemia. A single-centre randomized controlled isotope study // Arzneimittel-Forschung (Drug Research). 2007. 57 (6 a). P. 376–384.
- Burckhardt-Herold S., Klotz J., Funk F. et al. Interactions between iron (III)-hydroxide polymaltose complex and commonly used drugs. Simulations and in-vitro studies // Arzneimittel-Forschung (Drug Research). 2007. 57 (6a). P. 360–369
- Hutchinson C., Al-Ashgar W., Liu DY et al. Oral ferrous sulphate leads to a marked increase in pro-oxidant nontransferrin-bound iron // Eur. J. Clin. Invest. 2004. 34. P. 782–784.
- Geisser P. Safety and Efficacy of Iron (III) hydroxide Polymaltose Complex. A review of 25 years experience. Arzneimittel-Forschung (Drug Research) 2007. 57 (6 a). P. 439–452.
- Anker SD, Comin-Colet J., Filippatos G. et al. Ferric Carboxymaltose in Patients with Heart Failure and Iron Deficiency // N. Engl. J. Med. 2009. 361. P. 2436–2448.
E. S. Temnikova, Doctor of Medical Sciences, Professor
State Budgetary Educational Institution of Higher Professional Education Omsk State Medical Academy of the Ministry of Health of the Russian Federation, Omsk
Contact Information
What is the danger of long-term anemia?
Even mild anemia, if persisted for a long time, can cause serious damage to health! Prolonged oxygen starvation of tissues (hypoxia) leads to metabolic disorders, accumulation of toxic metabolic products, and excessive load on life-support organs - the heart, lungs, as well as excretory organs - liver, kidneys.
As a result of chronic hypoxia, sclerotic processes develop in tissues and organs - normal, working tissue is replaced by sclerotic (conditionally “scar”), as a result of which organs begin to gradually lose their function - cardiosclerosis develops with manifestations of heart failure (shortness of breath, edema, decreased exercise tolerance ), heart rhythm disturbances, respiratory failure, the function of the liver, kidneys, blood vessels, endocrine organs, and brain suffers. A person, without noticing it, acquires chronic diseases, loses his ability to work, becomes emotionally labile, depressed, and his immunity decreases. In addition, against the background of chronic anemia, any acute disease, be it a viral infection, tonsillitis, or more serious illnesses, is much more severe, dangerous complications develop much more often due to the fact that there are simply no compensatory capabilities in the body, they are depleted by a long-term hypoxic state.
In order to avoid the development of chronic diseases against the background of anemia, long-term, debilitating, and sometimes expensive treatments, you must follow simple rules:
- undergo an annual preventive examination - for a healthy person it will be enough to take a general blood and urine test, undergo fluorography and visit a therapist, gynecologist (urologist) and dentist.
- When identifying symptoms of chronic diseases that can lead to the development of anemia, promptly correct them.
- If there are signs of chronic bleeding, promptly diagnose and treat the diseases that cause them.
This is especially true for women with gynecological problems . Often, women are accustomed to enduring all hardships and long, heavy menstruation is considered almost a variant of the norm! This is fundamentally wrong - on the one hand, very often after treatment it is possible to restore the normal menstrual cycle quite easily and there is simply no reason for anemia; on the other hand, long, heavy periods, especially in women after 40 years of age, can be the first symptoms of oncological diseases of the female sphere !
- anemia must be treated! Even if you have mild anemia, it is necessary to promptly correct your hemoglobin level - sometimes just a diet and a monthly course of taking iron supplements are enough to restore normal blood counts and prevent the development of adverse long-term consequences!
At the ACMD-MEDOX clinic, almost all the necessary research methods for diagnosing anemia are available. Comfortable conditions, professional specialists, and modern equipment will allow you to undergo the necessary examinations painlessly and in the shortest possible time.
Experienced doctors at our center will help you identify the first signs of anemia in the early stages, understand the causes of its occurrence and prescribe adequate therapy for the identified pathologies! Be healthy!
What is hemoglobin and how does it affect blood pressure?
Hemoglobin is a complex protein that contains iron and circulates in the human blood inside red blood cells.
Its main function is the formation of a bond with oxygen and its transfer to the tissues and cells of the body. Normal hemoglobin level in an adult:
- men—130—160g/l;
- women—120—150g/l.
If we talk about the connection between hemoglobin and blood pressure, it is very significant: with an increase in the level of protein in the blood, pressure increases, and with its decrease, it decreases.
Does anemia occur in hypertensive patients and how to deal with it?
If we talk about whether high blood pressure is possible with low hemoglobin, we need to talk about the existence of such a combination, since anemia and high blood pressure can be in one person, like two diseases unrelated to each other. Each of these pathologies occurs for its own separate reason in most cases.
The presence of hypertension does not mean that a person is immune from low hemoglobin levels. In this case, it is imperative to look for the cause of anemia and eliminate it, not forgetting about blood pressure control.
Causes of high blood pressure in primary hypertension
It is difficult to name the exact cause of the development of chronic hypertension. The development of the disease occurs due to disruptions in the mechanisms of blood pressure regulation, which arise for various reasons. Functional defects include poor kidney function, which causes sodium to be retained in the body. More fluid accumulates in the body, and the kidneys do not respond to random increases in pressure during exercise and stress.
Increased activity of the nervous system can lead to blood pressure disorders. Changes in its sensitivity can be caused genetically or by environmental factors - stress, chronic fatigue or pain. When the activity of the central nervous system increases, the load on the heart increases.
The cause of high blood pressure can be circulatory disorders in tissues - edema due to metabolic problems, epithelial dysfunction.
In older people, blood pressure increases with age. In adolescents and young adults, the disease can be caused by environmental factors, lifestyle or heredity. The hereditary factor for essential hypertension is not disputed by doctors. So the probability of its inheritance is 30%.
Risk factors for primary arterial hypertension include:
- An excess of saturated fatty acids in the menu, in particular cholesterol.
- High salt content in foods, such as pickles and processed foods.
- Sedentary lifestyle and excess body weight.
- Smoking and alcohol.
- Tension, stress, nervous breakdowns.
Excess cholesterol is deposited on the walls of blood vessels, which narrows their lumen and interferes with blood flow. The structure of the arteries also changes due to excess salt. Excessive use makes blood vessels fragile and impairs their elasticity.
Weight, as one of the causes of hypertension, is considered in the context of BMI - overweight. If this indicator is significantly exceeded, measures must be taken to reduce the risk of complications. The risk of developing arterial hypertension with excess weight increases 2-6 times, especially with the upper type of obesity, when waist circumference increases.
Symptoms of iron deficiency
IDA is highly prevalent in children and adults worldwide. Almost every second preschool child and half of pregnant women suffer from iron deficiency. About 9% of children under two years of age are treated for anemia. According to WHO, the number of people with iron deficiency in the world is at least 600 million people.
Iron deficiency anemia can be mild, moderate, or severe. In mild cases, there are no clinical manifestations or they are practically not bothersome. Moderate symptoms that you should pay attention to include:
- fast fatiguability;
- weakness;
- decreased concentration;
- pallor of the mucous membranes and nail beds;
- peeling of the skin.
In severe forms, more pronounced symptoms are added:
- shortness of breath with minor exertion;
- dizziness, tinnitus;
- arrhythmia, rapid pulse;
- sleep disturbance;
- chilliness;
- brittle nails;
- frequent colds.
With the development of anemic precoma, the skin and mucous membranes become pale, tachycardia appears, hallucinations and depressive syndrome are possible. Urgent medical attention is needed. If the level of iron in the body is not normalized, an anemic coma may occur with loss of consciousness and lack of reflexes.
Is an increase in hemoglobin accompanied by an increase in blood pressure?
Causes of high hemoglobin:
smoking;- alcohol consumption;
- congenital heart defects;
- pulmonary failure;
- chronic heart failure;
- intestinal problems;
- excess vitamin B12;
- polycystic kidney disease;
- stay in high mountain areas;
- long-term physical activity;
- dehydration;
- diabetes;
- erythremia;
- oncology;
- intestinal problems.
Symptoms of high hemoglobin:
- drowsiness;
- fatigue;
- decreased appetite;
- visual and urinary disturbances;
- pale skin or redness;
- aching in bones and joints.
An increase in hemoglobin levels leads to thickening of the blood, and this in turn leads to an increase in blood pressure, since it is much harder for the heart to pump “thick” blood. But not only pressure instability is a problem in such a case: thickening also increases the risk of blockage of blood vessels, that is, it promotes thrombus formation. This impairs oxygen transport and also leads to thromboembolism, heart attacks, and strokes.
How to restore normal blood composition?
It is not recommended to carry out correction on your own. A doctor's consultation is required. If hemoglobin is increased or decreased by no more than 10 units, most likely this is not a consequence of any disease - these deviations indicate a functional state, which can be corrected by changing lifestyle, in particular nutrition.
Patients suffering from hypertension and increased hemoglobin are prescribed blood thinners: chimes, cardiomagnyl, aspirin.