Home » Department of Cardiology and Cardiac Surgery » Diseases » Ebstein's anomaly
Ebstein's anomaly is a fairly rare congenital heart defect (CHD), which is characterized by displacement of the tricuspid (tricuspid) valve leaflets into the cavity of the right ventricle. That is, the leaflets of the pathologically altered valve are formed from the walls of the right ventricle (RV), and not from the atrioventricular (atrioventricular) ring, as is normal, and they do not close completely, so tricuspid valve insufficiency develops.
This defect accounts for about 1% of all congenital heart defects. In addition, 75% of people with this pathology also have an atrial septal defect. Also quite common are pathological pathways through which abnormal conduction of impulses occurs. This is the cause of the development of arrhythmias. Ventricular arrhythmias are the most common. They and congestive heart failure are the main causes of death in patients with this pathology. If the defect is allowed to develop naturally, 60% of patients die by the age of 20.
Types of Ebstein's anomaly
There are 4 types of Ebstein's anomaly:
- Type I - the posterior and septal leaflets are displaced or absent, the anterior valve leaflet is mobile and large.
- Type II - the anterior, septal and posterior leaflets are usually present, but they are shifted towards the apex of the heart and are relatively small.
- Type III - the anterior valve leaflet has shortened and fused chords, restrictions in movement and is often shortened. The posterior and septal valve leaflets are underdeveloped and displaced.
- Type IV - the anterior leaflet of the valve is severely deformed and also displaced in the direction of the outflow tract from the right ventricle. The posterior valve is usually underdeveloped or absent, and the septal valve is represented by fibrous tissue.
Ebstein's anomaly (echographic, clinical and pathomorphological comparisons)
Ultrasound scanner HS60
Professional diagnostic tools.
Assessment of tissue elasticity, advanced 3D/4D/5D scanning capabilities, BI-RADS classifier, options for expert cardiological studies.
Introduction
An unusual heart defect was first described by the German scientist Wilhelm Ebstein in 1866 in a 19-year-old boy with cyanosis, shortness of breath, and dilated jugular veins. In 1927 it was named Ebstein's disease (anomaly) [1]. Ebstein's anomaly is a rare congenital heart defect characterized by displacement of the atrioventricular ring of the tricuspid valve towards the apex of the heart. Part of the right ventricular cavity is atrialized, so that the ventricular cavity itself becomes smaller. Heart failure inevitably develops, the degree of which and the time of manifestation are completely determined by the magnitude of the displacement of the right atrioventricular ring. The rarity of the defect affects its diagnosis. But remembering the disease means diagnosing it by 50%.
results
The prevalence of Ebstein's anomaly is low. For more than 40 years of work of the pathology department of the regional hospital, this defect was diagnosed in only 2 cases (in more than 6000 sectional studies): one adult and one child [2, 3]. Over a 40-year period (1979–2019) of work in ultrasound diagnostic rooms of multidisciplinary children's hospitals, we identified Ebstein's anomaly in 2 cases.
The manifestation of heart disease in all the children we observed developed early, in the first 3 months of life. The adult patient was engaged in heavy physical labor (mason). He developed manifest heart failure at the age of 62 years. Clinical symptoms in all cases were reduced to tachycardia, expansion of the borders of the heart, shortness of breath, congestion in the lungs and an increase in liver size. Auscultation revealed a rough systolic murmur at the base of the heart and on the vessels.
Radiologically, cardiomegaly, pulmonary oligemia, enlargement of the right atrium and enlargement of the right heart silhouette were noteworthy. In the absence of cyanosis, the vascular pattern of the lungs did not change.
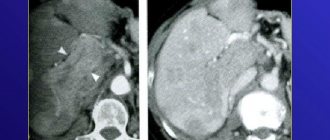
Ultrasound examination is decisive for the diagnosis. For Ebstein's anomaly, the typical finding was apical displacement of the septal and/or posterior leaflets of the tricuspid valve. Normally, the rings of the atrioventricular valves are located at the same level. In Ebstein's anomaly, the degree of displacement of the right atrioventricular ring directly correlates with the severity of the defect. The atypically large anterior leaflet prolapsed, causing a stream of regurgitation (Fig. 1).
Rice. 1.
Echogram - Ebstein's anomaly.
A sharply enlarged right atrium and a reduced right ventricle are clearly visible. Displacement of the right atrioventricular ring relative to the left.
RV - right ventricle, TV - tricuspid valve, RA - right atrium, LV - left ventricle, PM - papillary muscle, MV - mitral valve.
The ECG showed a high sharp P wave (dilatation of the right atrium), prolongation of the PR interval, deviation of the electrical axis of the heart to the right, and right bundle branch block.
During anatomical and histological studies (2 observations), the heart was sharply increased in size. The fibrous right atrioventricular ring is sharply displaced towards the apex of the heart. The right atrium was a large thin-walled cavity. The inner surface of the right atrium is devoid of trabecular muscles and is smooth. The papillary muscles are shifted towards the apex and are thin. The oval window is open. In an adult, the displacement of the right attroventricular ring relative to the left was less. Due to the long-term existence of the defect, the walls of the right ventricle were thickened up to 1.5 cm, in the apex area - up to 3.5 cm. Hypertrophy of the interventricular septum. The endocardium of the right ventricle is thickened and white. Fibrous cords from the endocardium penetrate the entire thickness of the wall of the right ventricle. Between the hypertrophied muscle bundles of the wall of the right ventricle there are wide layers of mature connective tissue. Fibroblasts are located among the collagen fibers.
Discussion
Ebstein's anomaly is a rare congenital heart defect occurring in approximately 1 in 200,000 live births, accounting for significantly less than 1% of all congenital heart defects. The causes of Ebstein's anomaly are heterogeneous. Based on the results of family and twin studies, genetic, reproductive and environmental factors (benzodiazepenes and lithium drugs in mothers) are indicated as possible causative factors. The vast majority of cases of this anomaly are sporadic; familial cases are rare. In rare cases, mutations of the cardiac transcription factor NKX2.5, deletions 10p13-p14 and 1p34.3-p36.11 are found in relatives [4, 5].
The morphogenesis of Ebstein's anomaly consists of incomplete detachment of the septal and posterior leaflets of the tricuspid valve during development from the myocardium, which leads to annular displacement and atrialization of the right ventricle. This entails overload of the remaining part of the right ventricle and its dysfunction. The anterior leaflet of the tricuspid valve is often redundant and is usually described as "sail-like". An unbalanced deformity results in rotational displacement of the tricuspid valve into the right ventricular outflow tract, causing varying degrees of obstruction. The severity of the disease varies and depends on the degree of valve displacement, the degree of atrialization of the right ventricle, outflow tract obstruction, and ventricular dysfunction.
The clinical picture is nonspecific. The degree of heart failure and its severity vary depending on the severity of atrialization of the right ventricle. In some patients, the defect, as in one of our observations, can manifest itself in adulthood. According to foreign data, the age of patients ranges from 1 day to the elderly. The earlier the symptoms develop, the more severe the defect. Newborns with Ebstein's anomaly in the presence of cardiomegaly, heart failure, increased pulmonary artery pressure, cyanosis and acidosis should be immediately referred to a specialized cardiac surgery department [5, 6].
Depending on the anatomical disorders of the valve apparatus, the following options are distinguished (as the prognosis worsens):
- The volume of the preserved part of the right ventricle is sufficient for full hemodynamics.
- The atrialized portion of the right ventricle is large, but the anterior leaflet of the tricuspid valve moves freely.
- The anterior leaflet is significantly limited in movement and creates obstruction of the outflow tract.
- Almost complete atrialization of the right ventricle [4, 7].
Conclusion
Echocardiography is the non-invasive method of choice in diagnosing Ebstein's anomaly. An ultrasound examination can reveal the degree of displacement of the valves, the function of the ventricles of the heart, and the presence of additional defects. Identifying the morphological details of Ebstein's anomaly is the main condition for determining patient management tactics. Echocardiography makes it possible to diagnose heart defects in utero.
Literature
- Balaguru D. Pediatric Ebstein Anomaly. Updated: Aug 14, 2018.
- Delyagin V.M. Congenital heart defects in children of the Aktobe region according to sectional data for 22 years // Pediatrics. 1977; 9:87.
- Delyagin V.M. Congenital heart defects in twins // Medical practice. 1978; 12:42–44.
- Attenhofer Ch., Connolly H., Dearani J., Edwards W. et al. Ebstein's Anomaly. Circulation. 2007; 115:277–285.
- Cherry C., DeBord S., Moustapha-Nadler N. Ebstein's Anomaly: A Complex Congenital Heart Defect. AORN J. The official voice of perioperative nursing. 2009; 89(6):1098–1114.
- Nihoyannopoulos P., McKenna W., Smith G., Foale R. Echocardiographic Assessment of the Right Ventricle in Ebstein's Anomaly: Relation to Clinical Outcome. JACC 1986; 8(3):627–635.
- Munoz-Castellanos L., Espinola-Zavaleta N., Kuri-Nivon M., Candace Keirns C. Ebstein's Anomaly: Anatomoechocardiographic correlation. Bio Med Central. Cardiovascular Ultrasound; 2007; 5: 43. doi: 10.1186/1476-7120-5-43.
Ultrasound scanner HS60
Professional diagnostic tools.
Assessment of tissue elasticity, advanced 3D/4D/5D scanning capabilities, BI-RADS classifier, options for expert cardiological studies.
Causes of development of Ebstein's anomaly
As is known, in the prenatal period, the human heart is formed in the first 9 weeks of pregnancy. It is at this time that all congenital heart defects develop.
It is during this period that Ebstein's anomaly is determined. This happens under the influence of a number of factors:
- viral infections;
- scarlet fever;
- measles;
- rubella;
- use of certain medications (sedatives, hypnotics, lithium preparations);
- drugs;
- alcohol.
Family history also plays an important role. It should be noted that the above reasons cause not only Ebstein's anomaly, but also almost all other congenital heart defects.
Diagnostics
The key examination method in diagnosing an abnormality is an echocardiogram (ultrasound of the heart), usually transesophageal echocardiography gives the most accurate results. An echocardiogram can accurately assess the presence and extent of tricuspid valve abnormality and also identify most other congenital heart defects that may be present.
Adults and older children who receive initial evaluation for Ebstein's anomaly usually undergo an exercise test to assess their physical performance, blood oxygenation during exercise, and the response of heart rate and blood pressure to exercise. These measurements are useful in assessing the overall severity of a heart condition and the need and urgency of surgical treatment.
It is also important to evaluate people who have the abnormality for the presence of cardiac arrhythmia. In addition to annual electrocardiogram (ECG) and ambulatory ECG monitoring, most of these people should be evaluated by an electrophysiologist after they are diagnosed to assess the likelihood of developing potentially dangerous arrhythmias.
Pathophysiology of Ebstein's anomaly
Due to the fact that the valve leaflets are formed from the tissues of the ventricle and are localized in it, a significant reduction in its cavity occurs. According to the decrease in the atrium cavity, the volume of blood ejected by the heart into the pulmonary trunk also decreases.
We should also not forget that the valve leaflets have an abnormal shape and are not able to completely isolate the ventricular cavity from the atrium cavity. There is a reflux of blood into the atrium, which causes stagnation of blood in the atrium and its hypertrophy. And since this is often accompanied by a septal defect, blood is dumped into the left atrium, which leads to mixing of arterial and venous blood and a decrease in blood oxygen saturation.
Symptoms of Ebstein's anomaly
The clinical symptoms of Ebstein's anomaly directly depend on the degree of tricuspid valve insufficiency, the type of heart rhythm disturbance, the amount of blood discharged through the atrial septal defect, as well as the degree of narrowing of the outflow tract of the RV (right ventricle).
Newborns with types III and IV Ebstein's anomaly develop severe hypoxemia after closure of the ductus arteriosus (patent ductus arteriosus).
- Patients begin to complain of shortness of breath, increased fatigue, pain in the heart, palpitations (feeling of heart contractions).
- The skin is bluish (cyanotic).
- Swelling appears in the lower extremities (a consequence of venous stagnation).
- In patients, the terminal phalanges of the arms and legs change (the appearance of “watch glasses” and “drumsticks”).
All these symptoms indicate that the body tissues are experiencing a lack of oxygen.
Forecast
The prognosis of Ebstein's anomaly depends on the severity of the tricuspid valve problem and the presence or absence of other congenital heart problems. Babies with the disease who are born critically have a high risk of mortality—more than 30 percent die before they are discharged from the hospital.
The risk of premature death when the abnormality is diagnosed in later childhood or adulthood also depends on the severity of the condition. However, in recent decades, aggressive surgical treatment and prophylactic treatment of potential cardiac arrhythmias have significantly improved the prognosis of people with Ebstein's anomaly.
Diagnosis of Ebstein's anomaly in Israel
- Auscultation reveals dull first and second sounds.
- X-ray : an increase in the size of the right atrium, depletion of pulmonary blood flow, the cardiothoracic index often approaches one.
- ECG (electrocardiography) : signs of right atrium hypertrophy are noted.
- EchoCG (echocardiography).
- Fetal echocardiography (EchoCG) : the defect is diagnosed prenatally (during pregnancy) in 60% of cases. The main symptom is a pronounced increase in heart size, mainly due to the right atrium. On the tricuspid valve, regurgitation (backflow of blood) of varying degrees is recorded.
- Cardiac catheterization and right contrast atriography.