© Author: A. Olesya Valerievna, candidate of medical sciences, practicing physician, teacher at a medical university, especially for SosudInfo.ru (about the authors)
The frequency of anomalies of the vein of Galen does not exceed one percent among people of all ages, but up to a third of cases of cerebral vascular defects in newborns and young children are due to this pathology. In male children it is detected twice as often as in girls.
According to statistics, up to 90% of cases of congenital malformations of the vein of Galen end in the death of children at an early age, which is associated both with the severity of the pathology and with the insufficient readiness of specialists to treat the disease, and the lack of equipped neurosurgical and vascular operating rooms. The prognosis is significantly worse in patients who were born with signs of heart failure, hydrocephalus and impaired blood flow in the cerebral hemispheres.
In recent years, mortality has been reduced to 70-80%, and the literature even describes isolated cases of successful control of pathology, which is largely due to progress in the field of ultrasound research methods and the improvement of microsurgical and endovascular techniques in neurosurgery. At the same time, unfortunately, doctors still cannot give parents of babies with anomalies of the vein of Galen any reassuring recommendations.
Anatomy and types of pathology of the great cerebral vein
The vein of Galen is called the great vein of the brain, since it is one of the largest venous trunks, carrying blood saturated with carbon dioxide and metabolic products from the internal parts of the brain - the subcortical nuclei, visual thalamus, transparent septum, plexus of the lateral ventricles.
The great cerebral vein belongs to the deep venous system and runs in the subarachnoid space (it is also called the cistern of the vein of the same name in this area), connecting with the inferior sagittal venous sinus to form the straight sinus. The large vein of Galen flows into the straight sinus.
The anatomy of the vein of Galen depends on the shape of the head. Its length is about 12-14 mm, while in people with a dolichocephalic type of skull (with a long and narrow head) it can reach 2 centimeters, and in brachycephalics with a short and wide head - a little more than a centimeter.
The diameter of the vessel is not related to the shape of the skull and averages 5-7 mm, however, it has been noted that brachycephals have a relatively short but wider trunk than dolichocephals with a long and narrower vein.
The normal speed of blood flow in the vein of Galen in children under one year of age is 4-18 cm/sec.
Among the changes that are most often detected in the vessel in question are:
- Aneurysm of the vein of Galen;
- Arteriovenous malformation of the great cerebral vein.
How to do an MRI of cerebral veins
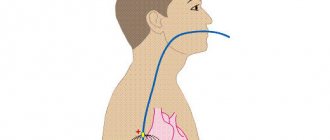
The classic MR venography protocol is a cycle of several sequential actions:
- the patient is placed on a horizontal platform in the “supine” position, a special RF coil is installed in the head area, which amplifies the tomograph signal;
- the moving part with the person is directed into a round magnet;
- Doctors go into the next room to monitor the operation of the devices on the computer.
You need to be prepared that during operation, medical equipment may make sounds in the form of pops, clicks or knocks. To make the process more comfortable, medical patients are offered to wear headphones and undergo the screening accompanied by pleasant musical accompaniment.
Aneurysm of the vein of Galen
Aneurysm of the vein of Galen is one of the most severe and quite difficult forms of vascular pathology of the brain for early diagnosis and treatment. Unfortunately, it is usually discovered no earlier than the third trimester of gestation, which comes as a real shock to expectant parents, because previous screening ultrasounds showed normal results.
At the same time, a defect identified during pregnancy, albeit quite late, makes it possible to decide on the tactics of treating the baby before birth, choose a clinic and specialist, and psychologically prepare for the fight for the well-being of the child.
An aneurysm of the vein of Galen forms in utero. Initially, the brain structures of a growing embryo are nourished by embryonic vessels, which mature into full-fledged arteries and veins during the first two months of gestation. If this process is disrupted, then in the fetal brain the embryonic vessels remain undeveloped, giving rise to aneurysms and other malformations.
Among the reasons that may contribute to abnormalities in the formation of the vascular bed are:
- Exposure to viruses and bacteria (herpes, rubella, respiratory infections, etc.);
- Taking certain medications;
- Effect of ionizing radiation.
It is important to note that the defect begins in the first third of gestation, but becomes noticeable for diagnosis much later.
From an anatomical point of view, an aneurysm can represent a local increase in the lumen of a vein, but much more often it looks like multiple communications between vessels in the form of a tangle consisting of embryonic-type vessels.
Blood from the arteries of the brain (the internal carotid and vertebrobasilar systems) is discharged into an abnormally formed vein, without sufficiently reaching the nervous tissue of the hemispheres and subcortical formations, which is why the latter experience anemia, and the venous section is overloaded.
Embryonic vessels lack a smooth muscle layer, so they can easily rupture with blood spilling into the nervous tissue, and can also be stretched by excess fluid. Stretching and increasing the diameter of the venous part of the bloodstream contributes to compression of the cerebrospinal fluid pathways and the development of hydrocephalus.
An aneurysm of the vein of Galen is found in the anterior part of the skull, behind and above the visual tuberosities in the cistern of the same name. There are several forms of aneurysm:
- Intramural, when the artery flows directly into the vein.
- Choroidal - represented by choroid plexuses in the choroidal fissure.
- Parenchymal - multiple vascular communications are located in the brain parenchyma.
Video: Vein of Galen aneurysms on ultrasound
Anatomy of cerebral veins, what is visible on MRI?
Veins are blood vessels that are designed to drain blood from the brain. Oxygenated blood enters the nerve center through the arteries, and after giving nutrients and oxygen to the cells, the blood returns to the heart through the veins.
Disturbances in the functioning of the cerebral veins can contribute to poor health, fatigue and the gradual development of cerebral edema. This is why timely and accurate diagnosis is so important.
Examination of the condition of the venous bed using a magnetic resonance imaging scanner is called MR venography.
In terms of information content, MRI of the arteries and veins of the brain is one step ahead of traditional diagnostic methods using X-rays or ultrasound. Using MR images, diagnosticians receive visual information about the functioning of the veins of the brain.
MR venography allows you to accurately determine:
- anatomical pattern of the venous system;
- congenital and acquired abnormalities in the structure and functioning of blood vessels;
- disturbances in trophism and blood flow from parts of the brain;
- possible damage to blood vessels and their consequences;
- the presence of tumor formations blocking the vascular bed.
A tomography examination is a completely safe procedure that allows not only detailed and high-quality visualization of the structural features of the venous network of the brain, but also scanning for preventive and diagnostic purposes with any frequency without negative impact on health.
Malformation of the great cerebral vein
Malformation of the vein of Galen is a change in the vascular system in which a plexus is found in the form of a tangle, consisting of embryonic-type vessels and, necessarily, an enlarged great vein (aneurysm). That is, malformation always includes an aneurysmal change in the vein.
Malformations are characterized by underdevelopment of the elastic and muscle fibers of the middle tunic of the vein, so even a slight increase in pressure is accompanied by an expansion of the lumen of the vessels, which only worsens over time. An aneurysm may have the appearance of a sac or a diffuse increase in the lumen of the vessel.
Arteriovenous malformation of the vein of Galen can be mural, when the brain arteries approach the aneurysmally dilated vein and flow into it directly, and choroidal - pathologically altered tangles of vessels feeding the malformation, flowing into the dilated vein of Galen.
The malformation together with the aneurysmally dilated vein of Galen puts pressure on the surrounding tissues, promoting their atrophic changes, displacement, blockade of liquor and venous outflow, which causes hydrocephalus to increase.
Video: Vein of Galen malformation
Tributaries
Vein of Galen is one of the most important elements of the circulatory system.
It has tributaries:
- medial tributaries located in the occipital region;
- the anterior superior vessel, which passes through the cerebellum;
- pineal gland;
- internal venous plexuses of the brain;
- Rosenthal vessels;
- posterior venous duct of the corpus callosum.
Manifestations of venous vessel anomalies
Symptoms of abnormalities of the venous bed of the brain appear at birth in half of the babies. The main symptom of an aneurysmal change in the vein of Galen is heart failure associated with increased venous pressure in the cerebral and vena cava, creating excess stress on the child’s heart. Since the aneurysm functions during the prenatal period, by the time of birth the baby has a high probability of cardiac decompensation.
child diagnosed with vein of Galen malformation
Clinical signs of an aneurysm are:
- Rapid fatigue of the child during feeding;
- Swelling of soft tissues;
- Shortness of breath with risk of pulmonary edema;
- Delayed physical development from the first months of life.
An unfavorable sign of impaired venous outflow is hydrocephalic syndrome, which indicates compression from outside by dilated vessels of the brain aqueduct carrying cerebrospinal fluid from the lateral ventricles and subarachnoid spaces, or a strong discharge of large amounts of blood into the veins of the skull.
Hydrocephalus is manifested by an increase in the size of the child’s head, expansion of its superficial veins, which is noticeable to the naked eye. Against the background of hydrocephalic-hypertensive syndrome, vomiting, convulsions, bulging eyes, strabismus, and focal neurological disorders are possible.
As a result of blood shunting, the hemispheres do not receive enough arterial nutrition, therefore the development of intelligence is disrupted and mental retardation is formed. In rare cases, hemorrhages into the brain with convulsions, coma, and paralysis are possible.
Malformation of the vein of Galen manifests itself in early childhood and is extremely rare in adults. Most often it occurs with hydrocephalus and intracranial hypertension due to compression of the cerebral aqueduct, as well as intracerebral hematomas, convulsive syndrome, mental and motor development disorders, and focal neurological disorders.
Due to the increased load on the myocardium, as well as due to concomitant malformations of the cardiovascular system, heart failure with shortness of breath, edema, and cyanosis appears quite early.
Depending on the severity of the course, several clinical types of malformation are distinguished:
- Type I - severe course with high mortality, cardiac and respiratory failure, enlarged liver, dropsy of the brain;
- Type II - severe neurological focal disorders, hypoplasia of parts of the brain, signs of arterial blood flow disturbance due to blood shunting;
- Type III - disorders of venous outflow with increased pressure, pathology of liquorodynamics, communicating hydrocephalus.
Alena and Artem: were in the smallest percentage!
On that day, the icon of the Mother of God “The Sign” was brought to the Church on the Blood in Yekaterinburg. Alena Babaeva really wanted to kiss. Her pregnancy was going well. 32 weeks already. It’s just that lately I’ve been having trouble sleeping at night.
It was not difficult to get to the icon: with its belly, people willingly gave way to it. But getting away from it is almost impossible. Tears flowed freely from the unsentimental Alena. Why? She couldn't understand it herself. She only remembers that she left the temple with a firm intention: she urgently needs to do an ultrasound!
At home, her “whim” was not supported. “What kind of nonsense? You just did it today! An excellent doctor looked at me, on recommendation. He said: everything is fine." But Alena stood her ground: it needs to be done urgently!
We signed up for the only medical center that had a “window” left. There was no time to choose, just to be accepted today! Late in the evening, the tired ultrasound technician was probably hoping to finish his work day quickly. But could not. A professional eye could not help but pay attention to this baby. There was clearly a mess in his head. “Most likely, hydrocephalus,” he brought the conclusion down on Alena’s head.
In the morning she was already standing on the threshold of the medical genetic center. Four uzists looked at her with pitiful eyes, not daring to pronounce a verdict. Finally, the council decided: “Malformation of the vein of Galen.” 90% of children with this diagnosis die in utero, of those who survive, 90% die on the first day.
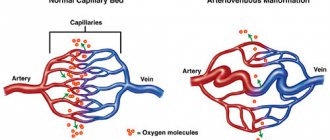
Arteriovenous malformation is a pathological connection between veins and arteries, in which there is no capillary network and arterial blood is directly discharged into the venous blood, depriving the corresponding organ of nutrition. The vein of Galen is one of the main venous collectors of the brain (collects blood from its internal structures). Arteriovenous malformation of the vein of Galen is a rare congenital disease of this vein.
But Alena did not agree. She didn't want to be one of those statistics. Three weeks later she had a caesarean section - and Artem was born. Alive. And he continued to survive. “Then we often ended up in the smallest percentage according to statistics. That is, statistically all this was very unlikely.”
On the third day, Artem had his first stroke - hemorrhage. Alena sent his documents to the three most famous neurosurgical clinics in the country, including in Novosibirsk to the National Medical Research Center named after Academician E.N. Meshalkin.
And then it turned out that Dr. Orlov from this center should come to Yekaterinburg. Having learned about Artyom’s case, he immediately said: “We must save him!” This probably really saved him. Because in all the official responses that came a month later, Artem was refused help: “inappropriate.”
After that life-saving operation (it was the first operation in the Sverdlovsk region to correct a malformation of the vein of Galen, which was successful), Artem underwent nine more neurosurgical operations. Each time, giving her son for surgery, Alena realized that she might be kissing him for the last time.
Aneurysm of the vein of Galen can cause complications in the form of cerebral palsy, hydrocephalus, and epilepsy. Artem suffered all the complications that one can imagine. The most severe of them is West syndrome, a complex form of epilepsy. It was this syndrome that provoked 30 respiratory arrests per day. Artyom lay motionless for days on end, his gaze seemed clouded and absent.
“It was as if he was not with us,” says Alena. “But we managed to defeat West syndrome. The son went into long-term remission, he returned to us, his freed brain began to perform a wide variety of tasks - from picking his nose to crawling.”
By the age of two, Artem was assigned level V according to the GMFCS gross motor function classification system. This meant he would never go. Typically, Level V children remain like this for their entire lives. But after two years, when drugs for epilepsy were selected, his body began to actively respond to rehabilitation. Today he can roll over on his own, get on all fours, stand and walk with support. And its capabilities are assessed as corresponding to level III according to the GMFCS system.
“Even with a walker, he’s already walking! It's incredible, but it's possible! And to all the women who come to me when faced with the same diagnosis, I say: “I always repeat the prayer “Lord! Give me the strength to change the things I can change, the courage to accept the things I cannot change, and the wisdom to know the difference.”
Alena, together with other parents whose children were diagnosed with AVM of the vein of Galen, is creating a support base for “newcomers.” Together they created a website where you can get the necessary information and contact experienced mothers who have already achieved good results.
Even if no pathologies were identified during pregnancy, be careful if you notice the following symptoms in your baby: gets tired quickly during feeding; swelling of the soft tissues of the head; an increase in head circumference beyond the norm; pronounced venous pattern on the head; possible: vomiting, strabismus, convulsions. Be sure to consult a neurosurgeon!
Nuances of diagnosing venous malformations
Diagnosis of pathology of intracranial veins is carried out through:
- X-ray contrast angiography - after the birth of a baby, this is the main research method that plays a decisive role in determining surgical tactics;
- Ultrasound analysis with Doppler measurements - before birth in the third trimester and after the birth of the baby (neurosonography) is the safest and most accessible diagnostic method;
- CT, MRI - in the early neonatal period.
Detection of an aneurysm of the vein of Galen becomes possible no earlier than the third trimester of gestation using ultrasound. The anomaly appears as an anechoic formation in the center of the skull. Ultrasound scanning is complemented by Doppler measurements to determine the nature of blood flow in pathologically altered vessels.
If a woman was not examined before childbirth, then it is extremely difficult to suspect a pathology both because of its rare occurrence and due to the absence in some cases of clinical signs at the time of birth of the child. Pediatricians make the diagnosis by excluding other causes of cerebral edema and heart failure.
In addition to ultrasound diagnostics, computed tomography and MRI are used, which show tangles of abnormally developed intracranial vessels. X-ray contrast angiography makes it possible to clarify the nature of the branching of embryonic vessels, their relationship with normal ones, the presence or absence of thrombosis, based on the results of which a surgical treatment plan is also developed.
Indications and contraindications for MRI of cerebral veins
Indications for magnetic resonance imaging of cerebral veins may include the following symptoms and conditions:
- frequent headaches;
- sudden dull headache;
- traumatic brain injuries;
- tinnitus, dizziness, fainting;
- a feeling of pressure and fullness in a certain area of the head;
- feeling of pressure on the eyeballs;
- coordination problems;
- problems with memory, speech;
- a sharp decline in cognitive abilities and the ability to concentrate in young patients;
- cognitive impairment in older people;
- single or repeated epileptic seizures.
If one or more of the above symptoms occur, patients should consult a doctor who will give a referral for an MRI of the veins of the brain.
Diagnostician prepares patient for examination
MR venography can be indicated not only in the presence of any ailment, but also for preventive purposes for the early detection of vascular diseases.
Contraindications to the procedure
MRI is considered a safer method of visual diagnosis of internal body structures than CT. However, MR scanning also has a number of contraindications, which can be divided into absolute and relative.
Absolute contraindications include:
- the presence of metal objects in the body (fragments from wounds, shot);
- a pacemaker or neurostimulator installed in the patient;
- cochlear implants, vascular clips;
- the patient’s weight category is over 130 kilograms and body girth from 150 centimeters;
- first trimester of pregnancy;
- age up to 5 years.
Before prescribing a referral for an MRI of the cerebral veins, the doctor must check the patient for the presence of risk factors.
Relative contraindications do not negate the diagnosis, but require careful preliminary preparation. The procedure is not indicated in the case of:
- severe damage to the cardiovascular system in the acute stage;
- presence of tattoos on the body containing paint with metal particles;
- mental disorders in the acute stage;
- fear of being in a confined space;
- inability to maintain long-term immobility.
Prostheses made of non-ferromagnetic materials do not prohibit MRI screening if the following requirements are met:
- availability of documents for the prosthesis;
- the prosthesis was installed no later than 3 months before the diagnosis;
In addition, if the prosthesis is located outside the scanning area, its presence will not interfere with the screening.