Heart and blood vessels
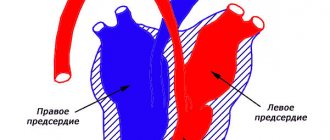
The basis of the circulatory system is the heart, which, like a pump, pumps blood through the arteries, ensuring the delivery of oxygen and nutrients to all organs and tissues. The heart is located in the chest along the projection of the sternum, slightly to the left, and is a hollow muscular organ the size of a fist. The heart has 4 chambers separated by septa. Between the left atrium and the left ventricle, as well as the right atrium and the right ventricle, there are openings with valves that regulate the direction of blood flow from the atria to the ventricles. Blood circulation occurs through the systemic and pulmonary circulation. Blood collects from all organs and tissues and enters the right atrium through the veins. From the right atrium, through the corresponding opening, venous blood flows into the right ventricle. Both of these right reservoirs (atrium and ventricle) are also called the right heart (“venous”). The pulmonary circulation begins in the right ventricle. From the right ventricle, due to the contraction of its muscular wall, dark, oxygen-poor and carbon dioxide-rich blood is pushed into the pulmonary artery and flows through it into the lungs. There it enters small arteries and capillaries, is cleared of carbon dioxide by diffusion and enriched with oxygen, acquires a bright red color and is already called arterial blood. Through four pulmonary veins, arterial blood enters the left atrium, and this completes the pulmonary circulation. Considering that the left cavities of the heart (atrium and ventricle) or the left heart are already filled with arterial blood, the left heart is called “arterial”. The systemic circulation begins in the left atrium. From the left atrium, arterial blood flows into the left ventricle, which is an even more powerful pump than the right ventricle. Contracting, the left ventricle pushes blood into the aorta and its branches, through which it enters all organs and tissues, down to the smallest capillaries. Having given oxygen to the tissues and taken away carbon dioxide from them, the blood again becomes venous. Venous capillaries gradually connect with each other into larger veins, which, in turn, form two wide ones: the superior and inferior vena cava. The superior vena cava collects blood from the head, neck, upper limbs and torso walls, and the inferior vena cava collects blood from the lower limbs, abdominal organs and pelvic region. Both vena cavae carry blood to the right atrium, where the systemic circulation ends.
In this way, 2 closed circles of blood circulation are obtained, which are connected by the motor of the human body - the heart. So, the systemic circulation begins in the left ventricle of the heart and ends in the right atrium. Its function is to supply all organs and tissues with nutrients and oxygen. The pulmonary circulation begins from the right ventricle and ends in the left atrium. Its function is to enrich the blood with oxygen in the lungs. The heart muscle, constantly performing enormous work, itself needs nutrition and oxygen. Blood flows to the heart through vessels that extend directly from the aorta and surround the heart like a crown or crown, which is why they are called coronary or coronary arteries.
Movement of blood through vessels.
The heart does a lot of work. So, in one minute it pumps 4.5–5 liters of blood in only one direction. Blood movement is ensured by valves located between the atria and ventricles, between the left ventricle and the aorta, pulmonary vessels and the right atrium. The speed of blood movement through the vessels depends on their diameter: if in the aorta the blood moves at high speed, then in the capillaries this speed is minimal. When the cardiovascular system is damaged by an atherosclerotic, inflammatory or degenerative process, both general and local circulatory disorders can be observed. An example of general circulatory disorders is heart failure with shortness of breath, palpitations, cough, bluish skin and swelling. An example of local circulatory disorders, when the blood supply to any organ is affected, is a heart attack (of the heart, lung or kidneys), or gangrene of a limb. But since the circulatory system functions as a single whole, even local circulatory disorders in any organ eventually affect the entire system. The activity of the heart is regulated by the central nervous system. In addition, the heart also has its own intracardiac regulatory mechanisms that promote rhythmic contraction (systole phase) and relaxation (diastole phase) of the heart. In an adult, the number of heartbeats per minute normally ranges from 60 to 80 beats; in athletes, the heart works more economically. Their heart rate is 40–50 beats per minute.
Arteries of our body
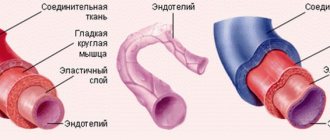
Before talking about atherosclerosis, let us recall the anatomical features of the arteries. Arteries are cylindrical elastic tubes of various diameters. The wall of arteries is much thicker than that of veins, the vessels that carry blood back to the heart. This difference in the thickness of the vessels is not accidental and is due to the fact that the blood pressure in the arteries is much greater than in the veins. The arterial wall consists of three layers: outer, middle and inner. The outer layer or serosa is a framework of connective tissue; the middle (muscle) layer consists of smooth muscle fibers; the inner layer (intima) is lined with a single layer of cells and is called endothelium. It is the endothelium, or rather its damage or dysfunction, that plays a major role in the development of atherosclerosis. However, we will talk about this later. The lumen of the arteries can change as a result of contraction or relaxation of the smooth muscle fibers of the middle layer. The dilation of blood vessels (for example, in hot conditions) helps to increase blood flow and more intense metabolism, and conversely, their narrowing (in low temperatures) slows down these processes in the body. If the vessels are constantly narrowed for some reason, then the organs and tissues receive little blood, and therefore oxygen. Over time, this leads to disruption of the functioning of those organs and tissues that are nourished by narrowed arteries.
Vascular changes in atherosclerosis
Atherosclerosis (from the Greek words “ather” - gruel and “sclerosis” - hardening), exactly as the name suggests, is the process of accumulation of soft deposits of lipids (fats, fat-like substances, primarily cholesterol) on the walls of arteries.
It has been established that atherosclerosis develops in response to damage to the endothelium (the inner lining of blood vessels).
Damage or dysfunction of the endothelium can be caused by a number of reasons, in particular, smoking, significant increases in blood lipid levels, high blood pressure, acute or chronic psycho-emotional stress, viral or bacterial infection. Following damage to the endothelium, fats, fat-like substances, and cholesterol begin to penetrate into the arterial wall. Leukocytes, or rather their special varieties, monocytes and macrophages, rush here from the blood. This is the beginning of the formation of an atherosclerotic plaque. The “mush” formed on the wall of the artery is covered with a thin connective tissue capsule consisting of fibrin threads. Such an atherosclerotic plaque is called young. Over time, as the atherosclerotic process progresses, calcium begins to accumulate in the plaques, and fibrous and connective tissue grows. The plaque becomes covered with a thick capsule (this is a formed plaque), increases in size and significantly narrows the lumen of the artery. Often several plaques form and merge with each other, further narrowing the lumen of the vessel. Due to the narrowing of the lumen of the vessel, the organ supplied with blood does not receive the required amount of oxygen and chronic ischemia occurs (from the Greek words “ishe” - I retain and “hemo” - blood). Thus, when one or more coronary arteries narrows, chronic myocardial ischemia occurs (chronic coronary heart disease).
Acute ischemia (acute vascular insufficiency) develops differently. The fact is that the body produces special enzymes that “eat away” the connective tissue membrane of the atherosclerotic plaque from the edges, reaching its soft, mushy core. When the plaque capsule is opened, this mass enters the blood. An open wound on the capsule of an ulcerated plaque becomes covered with sticky platelets. Gradually, a blood clot forms - a thrombus, which bulges into the lumen of the vessel, sharply narrowing it. A thrombus can break away from the vessel wall and, moving with the blood flow, clog a smaller vessel, creating acute local vascular insufficiency and stopping tissue nutrition, which leads to tissue necrosis (death). For example, when one of the coronary arteries of the heart is blocked, myocardial infarction occurs; when thrombosis of the femoral artery or leg artery occurs, foot necrosis (gangrene) occurs. Atherosclerosis can completely affect the aorta and its branches, but more often arteries of various sizes are affected, and not throughout, but in certain areas. Atherosclerotic plaques “love” to form in places where arteries bend and branch, which are especially numerous in vital organs. Thus, the coronary arteries of the heart, the vessels of the brain, the abdominal aorta and its branches that supply blood to the abdominal organs, kidneys, pelvic organs, and lower extremities are most susceptible to atherosclerosis. Often, atherosclerosis initially favors one organ. For example, with damage to the coronary arteries, coronary heart disease develops; with atherosclerosis of the cerebral arteries, coronary artery disease develops, including stroke. When the iliac or femoral vessels are narrowed by atherosclerotic plaques, obliterating atherosclerosis of the vessels of the lower extremities occurs. If the renal vessels are affected by atherosclerosis, then hypertension may develop with a predominant increase in the “lower” numbers of blood pressure. Depending on the location of the affected vessels, clinical manifestations of atherosclerosis of a particular vital organ are formed. Atherosclerosis in its development is not similar to any other disease, since its first signs appear in early childhood. Thus, at six months of age, some babies begin to develop fatty spots and stripes on the inner wall of blood vessels. During the growth process, a significant part of these spots resolves and only a few remain. If you do not engage in prevention, then by the age of 35-50 in men and somewhat later in women, clinical signs of atherosclerosis appear in the form of coronary heart disease, coronary disease of the brain and other organs. The resulting disease requires many years, and in fact lifelong treatment. Meanwhile, in medicine it has long been proven that serious diseases, including atherosclerosis, are better and easier to prevent than to treat later for many, many years. In order to prevent atherosclerosis, you need to know everything about the substrate of atherosclerotic plaques - cholesterol and its assistants - lipoproteins.
Publications in the media
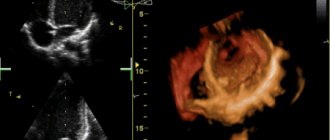
Single ventricle of the heart (SVC) is the absence of a septum between the ventricles of the heart. The main symptom is the communication of both atria through the mitral and tricuspid valves with a common ventricle. The structure of the heart is three-chambered. Frequency : 1.7% of all congenital heart defects (CHD).
Classification • Type A - single right ventricle (no inflow part of the right ventricle) • Type B - single left ventricle (no inflow part of the left ventricle) • Type C - undivided or common ventricle (no interventricular septum) • Type D - anatomy of the EVC is uncertain ( the inflow parts of both ventricles and the interventricular septum are absent).
Hemodynamics. In the single ventricular chamber, mixing of arterial and venous blood occurs. In the aorta and pulmonary artery (PA), which extend directly from the ventricle, the pressure is the same, which leads to the development of pulmonary hypertension.
Clinical picture • Complaints - shortness of breath, tachycardia, frequent respiratory diseases, more pronounced in the absence of PA stenosis • Examination •• Cyanosis, symptoms of “watch glasses” and “drumsticks”, more pronounced in PA stenosis •• “Heart hump” •• Systolic trembling along the left edge of the sternum •• Auscultation - II sound over the PA is accentuated in the absence of its stenosis; systolic murmur in the III–IV intercostal spaces; systolic murmur over the apex of the heart (relative mitral insufficiency); rough systolic murmur over the base of the heart according to the level of stenosis.
Research methods • ECG (deviation of the EOS to the right, hypertrophy of the EVC: the presence of ECG signs of hypertrophy of both the right and left ventricles) • X-ray examination of the chest organs (increase in the diameter of the heart shadow, increased pulmonary pattern) • Cardiac catheterization (high pressure in the EVC cavity, equal to the pressure in the aorta; increased oxygenation of blood in the ventricular cavity compared to the right atrium) • An angiocardiographic study allows you to determine the anatomical structure of the EVC, the location of the great vessels, and identify associated defects • EchoCG helps to identify the absence of an interventricular septum and the presence of two atrioventricular valves that open in EZhS.
Differential diagnosis • Tetralogy of Fallot • Open common AV canal • VSD • Transposition of the great vessels.
TREATMENT
Drug treatment - see Heart failure.
Surgery. Indications: all patients with EWS.
• Palliative operations are performed in young children and patients with the impossibility of radical correction due to many concomitant defects •• Surgical narrowing of the PA is performed with sharply increased pulmonary blood flow and high pulmonary hypertension •• Aortopulmonary anastomosis according to Blalock-Taussig is performed with severe PA stenosis and severe hypoxemia.
• Radical surgery is necessary when there is an increasing deterioration in the patient’s condition due to a progressive increase in the size of the heart and pulmonary vascular resistance. Radical correction is based on the principle of anatomical restoration of the structure of the heart - the creation of a septum dividing the EVC into arterial and venous chambers, and the elimination of associated heart defects. Necessary conditions for a successful operation are a sufficiently large size of the EVC cavity, correctly formed atrioventricular valves, normal location of the great vessels or synistrotransposition of the aorta in relation to the pulmonary trunk. Due to the fact that the implanted septum does not grow with the heart, the optimal age for surgery is 10–13 years. If radical correction is not possible (due to a seated tricuspid valve or due to insufficiency, hypoplasia or atresia of one of the atrioventricular valves) or is associated with a high risk, a hemodynamic Fontan correction is performed (see Tricuspid valve atresia).
Complications • Heart failure • Pulmonary hypertension • Cardiac rhythm disturbances • Postoperative complications (rhythm disturbances; renal failure; partial separation of the patch separating the UVC).
Course and prognosis. The prognosis is unfavorable. In the first year of life, 75% of patients die. The average life expectancy in the natural course of the defect is 6–7 years. Mortality after radical correction is up to 40%, after hemodynamic correction, subject to all Schuss criteria (see Tricuspid valve atresia) - up to 10%. Long-term mortality is 8–10%.
Synonyms • Common ventricle • Three-chamber heart with a single ventricle • Single-ventricle heart • Three-chamber heart with two atria
Abbreviations • EVC - the only ventricle of the heart • PA - pulmonary artery