Indications, contraindications and adverse reactions during treatment with Actovegin
The medication in tablets is recommended for use in patients with certain diseases:
- in complex therapy of metabolic and vascular disorders associated with dementia, ischemic stroke, circulatory failure, and head injury;
- diabetic polyneuropathy, trophic ulcers, angiopathy.
Injection solutions and droppers with Actovegin are prescribed for similar diseases and conditions as for tablets.
Direct contraindications for therapeutic procedures are:
- pulmonary edema;
- fluid retention in tissues;
- decreased daily urine production, anuria;
- individual allergic reactions to the component composition;
- heart failure in the decompensation phase.
Actovegin rarely causes adverse reactions and is well tolerated by most patients. Sometimes during treatment the following is recorded:
- swelling, urticaria, fever, sweating, hot flashes and other allergy symptoms;
- nausea with vomiting, dyspepsia, epigastric pain, stool disorders;
- state of weakness, cephalalgia, attacks of dizziness, short-term fainting, involuntary trembling of the body, decreased blood pressure or hypertensive symptoms;
- painful sensations in the chest area, paleness of the skin, shortness of breath, rapid heartbeat;
- rapid breathing, problems with swallowing, discomfort in the throat and chest, feeling of suffocation;
- pain in the lumbar area, joints and bones.
If adverse reactions to treatment occur, it is necessary to consult your doctor and replace Actovegin with an analogue.
results
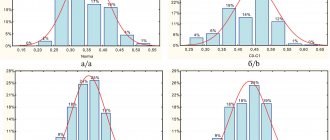
Changes in the level of skin perfusion that arose as a result of the study in patients are indicated in Table. 1.
Table 1. Oxygen regime of tissues before and after treatment with Actovegin
| Observation days | Before treatment | 15 days | 30 days | 60 days |
| Control group | 0,41±0,03 | 0,46±0,02 | 0,46±0,09 | 0,42±0,08 |
| Actovegin group | 0,43±0,04 | 0,51±0,03 | 0,52±0,02 | 0,54±0,09 |
Before treatment, both groups were comparable in terms of the initial level of microcirculation. In the control cohort of patients, despite standard therapy, no statistically significant improvement in transcutaneous oxygen tension was obtained, which may indirectly indicate that these medications do not affect the microcirculation.
In the Actovegin group, skin perfusion improved by 35% by day 15 of observation, at the end of the parenteral course. This result was maintained at the achieved level by days 30 and 60 with the help of an extended course of taking the drug in tablet form (Table 2)
Table 2. Effect of atovegin on microcirculation of the skin of the foot
| Time | First group (n-30) (APU) | Second group (n-30) (APU) |
| Before treatment | 42±3.1 | 43±2.4 |
| 15 days | 45±2.8 | 62±1.7 |
| 30 days | 48±1.7 | 75±2.1 |
| 60 days | 53±1.4 | 89±2.6 |
After morphological studies in the control group, a tendency towards intensification and growth of inflammation in the demarcation zone was revealed, followed by the development of necrobiotic and then necrotic changes in this area. Which was macroscopically expressed in the proximal spread of the area of dry necrosis (gangrene).
By day 15, compared with the initial data according to histological examination, activation of reparative processes was observed in the form of increased activity and an increase in the number of macrophages and fibroblasts (Fig. 4, Fig. 5).
During the same time period, cytological data indicate a significant decrease in the activity of the inflammatory process in the form of a 3-4-fold decrease in leukocyte infiltration by neutrophils (Fig. 6, Fig. 7).
In the Actovegin group, significant changes were noted during the period of parenteral administration of the drug, which was a manifestation of the activation of the corresponding metabolic links that are affected by the drug at the initial stage of treatment. In subsequent periods, consolidation of the result at the achieved level was observed.
Dosages in the instructions and methods of use of Actovegin
The injection solution is used for intravenous and intramuscular administration:
- Depending on the complexity of the pathological process, Actovegin is used in dosages from 10 to 20 ml IV, then the volume changes to 5 ml. The drug is prescribed daily or several times a week.
- For metabolic and blood circulation disorders in the GM - two weeks, 10 ml every day, the next month - from 5 to 10 ml several times a week.
- Ischemic stroke, arterial angiopathy - from 20 to 50 ml mixed with infusion solution (300 ml). Therapy is carried out for 2-3 weeks.
- Trophic ulcers, burns - 5 ml IM or 10 ml IV. This dosage is prescribed 1-2 times a day, with additional local therapy with another form of Actovegin.
Prevention and treatment of skin pathologies requires daily administration of 5 ml of the product intravenously, in between radiation exposures.
The solution for infusion is prescribed according to a different scheme:
- the medicine is injected into the veins or arteries, the final doses depend on the condition of the body;
- the daily norm is 250 ml, later it is increased to 500 ml;
- The therapeutic course includes 10-20 manipulations.
The dropper speed should not exceed 2 ml per minute. The solution should not penetrate into tissues adjacent to blood vessels.
The instructions for the tablets indicate that they should not be chewed, but should be taken before meals and washed down with a small amount of liquid. From 1 to 2 pieces are prescribed three times a day, the duration of treatment is 1-1.5 months.
For diabetic polyneuropathy, the medication is administered intravenously, 2 g per day (3 weeks), then switched to tablets - up to 3 pieces per day, for 4 months.
The incidence of chronic cerebrovascular accident is determined to be 70-100 cases per 1000 population [8], and impaired cognitive function is recognized as one of the most common manifestations of cerebrovascular disease. According to population studies, the initial manifestations of this disorder are detected in 24.4% of the urban population of elderly and senile age (60 years and older), and among elderly patients observed in a psychoneurological clinic - in 18.7% [1]. During a comprehensive examination of elderly patients at a territorial clinic, these disorders were found in 30.8% [6]. Mild cognitive impairment (MCI) as part of vascular psychoorganic syndrome in 24.5% of cases is the reason for contacting a gerontopsychiatrist at a general somatic clinic, and in another 36.2% of cases it is diagnosed as a comorbid disorder in patients of a gerontopsychiatric office [6 ].
MCI[] syndrome is characterized by a borderline disorder of memory and cognitive functions, the degree of manifestation of which does not allow a diagnosis of dementia of cerebrovascular or other origins, including Alzheimer's disease (AD) [2].
The prevalence of MCI syndrome in old age is extremely high. Among the Moscow population over 60 years of age, this figure is about 18% [4]. Similar figures (19%) are given by O. Lopez et al. [15]. As has been shown by domestic researchers [9], 40% of people with an established diagnosis of MCI are diagnosed with AD or dementia of another origin within 4 years.
In recent years, evidence has been obtained of the heterogeneity of the MCI syndrome, and therefore various clinical variants of the syndrome have been identified (amnestic, non-amnestic and variant with multiple cognitive impairment), which have a different prognosis in terms of the likelihood of transition to different nosological types of dementia (AD, vascular or frontal dementia). temporal dementia, dementia with Lewy bodies, etc.).
A high risk of worsening cerebral vascular disease, including an increased risk of cerebrovascular accidents, as well as the risk of developing dementia even without stroke, is most often associated with MCI syndrome with multiple cognitive impairment [5, 15].
In this regard, the tasks of treating MCI of vascular origin in elderly and senile patients have become the most pressing in geriatric practice and constitute the daily content of the activities of both neurologists and psychiatrists, as well as general practitioners [12, 14]. Treatment of the initial manifestations of cognitive decline is one of the most important tasks of complex therapy, including the prevention of dementia in the elderly.
Current treatments for initial cognitive decline of vascular origin include improving blood rheology, improving the delivery and use of oxygen and glucose in cerebral structures; reduction of neurotransmitter deficiency.
Actovegin, used for the treatment and prevention of hypoxic and ischemic disorders of organs and tissues, belongs to the group of drugs without direct vasodilating effects. The drug acts as a neurometabolic stimulant, increasing the energy supply of nerve cells by increasing the consumption and utilization of oxygen and glucose, which leads to improved brain function.
Actovegin is a highly purified hemodialysate obtained by ultrafiltration from the blood of young bulls under the age of 6 months. The drug contains exclusively physiological components with high biological activity - organic low-molecular compounds: amino acids, oligopeptides, nucleosides; intermediate products of carbohydrate and fat metabolism: oligosaccharides and glycolipids. The molecular weights of the organic compounds that make up Actovegin do not exceed 5000 daltons. The technology for obtaining hemodialysate excludes the presence of protein and other components with antigenic and pyrogenic properties. Experimental and clinical studies have proven that Actovegin does not contain additional impurities of blood components.
The therapeutic effectiveness of Actovegin is due to a wide range of substances included in its composition: amino acids, oligopeptides (insulin-like action), nucleosides, electrolytes (potassium, sodium, phosphorus, magnesium, calcium, copper) and microelements, as well as intermediate metabolic products (oligosaccharides, glycolipids).
Numerous studies have shown that Actovegin, by improving the absorption of oxygen and glucose by nerve cells, has an activating effect on metabolic processes in the brain. When glucose consumption increases, oxygen consumption increases accordingly. These processes lead to the acceleration of ATP synthesis in the brain, stimulation of cellular metabolism, and improvement of blood supply to ischemic brain tissue, which provides a clear therapeutic effect for cerebrovascular accidents.
The supply of large amounts of oxygen causes activation of aerobic oxidation, which in turn increases the energy potential of the cell. Actovegin improves energy exchange in the vascular endothelium, which leads to the release of endogenous substances with vasodilating properties - prostacyclin and nitric oxide - and improved perfusion of all tissues and a decrease in peripheral resistance. In conditions of tissue hypoxia caused by impaired microcirculation, Actovegin promotes the restoration of the capillary network due to newly formed vessels. By improving oxygen delivery and reducing the severity of ischemic tissue damage, Actovegin promotes the protein-synthesizing function of cells.
The effect of Actovegin is most pronounced under conditions of intracellular oxygen deficiency, in particular due to hypoxia or hypoperfusion, and the antihypoxic effect of Actovegin extends not only to neuronal, but also to glial structures. The effect of Actovegin begins to manifest itself no later than 30 minutes (10-30 minutes) after parenteral administration and reaches a maximum after an average of 3 hours (2-6 hours).
Due to the fact that Actovegin improves microcirculation and has an activating effect on metabolic processes in the brain, it seems reasonable to study its effectiveness in elderly patients with cognitive impairment of vascular origin. Although Actovegin has been known for about 40 years as a classic neurometabolic drug, its attitude towards nootropic properties has fluctuated from doubts to evidence-based statements. A number of controlled studies [6, 7, 9, 12, 15, 17, 19] have shown the effectiveness of Actovegin in cognitive disorders of varying severity, including dementia of vascular and Alzheimer's origin [7, 9, 12]. Most studies show the benefits of parenteral administration of Actovegin by intravenous infusion of 250 ml (2000 mg) in a course of at least 10 infusions; however, a faster onset of effects on cognitive impairment is indicated. Reduction or leveling of memory and attention disorders, an increase in the pace of mental processes are recorded in more than half of the patients. There are no data on the results of another method of parenteral administration of Actovegin - intramuscular, which is much more convenient for widespread use in outpatient practice.
The purpose of this work is to study the effectiveness and safety of intramuscular use of Actovegin in elderly patients with mild cognitive decline syndrome of cerebrovascular origin.
Material and methods
The study was conducted as an open, uncontrolled study in a group of patients with MCI syndrome of vascular origin, under the supervision of employees of the Department of Alzheimer's Disease and Associated Disorders of the Department of Geriatric Psychiatry of the Scientific Center for Mental Health of the Russian Academy of Medical Sciences.
Inclusion criteria
patients in the study: women (postmenopausal) and men aged 50 to 85 years;
MMSE score ≥26 points; compliance with the operational criteria for the diagnosis of mild cognitive decline syndrome (MCI) (patient complaints of memory loss, confirmed by an informant - usually a family member, and objectively detected signs of mild cognitive dysfunction; score 0.5 on the CDR scale; no basis for a diagnosis of dementia; preservation of daily activities , although slight deterioration in complex and instrumental types of daily and/or professional activities is possible); Hacinski scale score >4 points; obtaining written informed consent from the patient. Exclusion criteria
: diagnosis of dementia according to DSM-IV, ICD-10 criteria; other organic diseases of the nervous system, congenital and/or acquired metabolic encephalopathies, toxic and drug encephalopathies, Parkinson's disease, stroke, epilepsy, infectious diseases, demyelinating and hereditary degenerative diseases of the central nervous system); neoplastic and/or traumatic brain injury; systemic diseases; severe organ pathology: malignant extracerebral, HIV infection, diabetes mellitus in the stage of decompensation or other endocrine diseases; alcoholism and/or drug dependence; drug or other intoxication; depression with a score >18 on the Hamilton Depression Scale; systolic pressure level >180 mm Hg, diastolic >95 mm Hg; deficiency of folic acid and/or vitamin B12; hypothyroidism; treatment with procognitive agents for 4 weeks before or during the study.
At the end of the run-in period, which lasted up to 7 days, patients were prescribed Actovegin at a dose of 200 mg (5 ml) intramuscularly, and treatment continued for 28 days.
Concomitant therapy was allowed to use short-acting benzodiazepine drugs and drugs aimed at treating somatic pathology if therapy with them began 1 month before the present study and continued throughout the study in stable doses.
The assessment of the patients' condition during treatment using scales was carried out on fixed days: day 0 (before the start of therapy), day 14 of the study, day 28 of the study (end of the treatment course), day 56 (follow-up period).
Before and during the study, the following methods of examining patients were used: objective clinical examination, ECG, laboratory blood and urine tests.
In accordance with the recommendations of S. Kanowski [14], the effectiveness of a nootropic drug should be assessed in three areas: psychopathologically (assessment of clinical symptoms); psychometrically (testing); by behavior (self-esteem and assessment by others, taking into account age characteristics).
The following scales and tests were used to assess the state of cognitive functions and daily activity of patients: CGI (Clinical Global Impression Scale), MMSE, Speech Performance Test, Frontal Dysfunction Scale, Clock Drawing Test, Boston Naming Test, Mattis Dementia Scale, 10 Word Memory Test , Hamilton Depression Scale. The safety of the drug was assessed using an adverse event rating scale.
The study included 30 patients, 7 men and 23 women aged from 53 to 84 years (average 71.2±8 years), who were undergoing inpatient or outpatient treatment.
The age of the patients at the onset of the disease ranged from 52 to 81 years (average 67.8±7.9 years). The duration of the disease in all cases (with the exception of one) coincided with the duration of the psychopathological state that was the indication for the prescription of Actovegin, and ranged from 1 year to 7 years (on average 3.3 years).
All patients with sufficiently long duration of disorders that met the criteria for MCI syndrome had no signs of obvious progression of cognitive impairment. In all cases, the score on the General Deterioration Scale - GDS (Global Deterioration Scale) corresponded to point 3, which reflects the most initial manifestations of the disease [18]. The assessment of cognitive status according to the Clinical Dementia Rating - CDR (Clinical Dementia Rating) in all cases did not exceed 0.5 points, which excluded or made the diagnosis of dementia doubtful due to the mild degree of the disorder. According to the Clinical Global Impression - Severity (CGI-S) scale, the severity of the patients’ condition was classified as “borderline disorder” in 10 patients, and in the remaining 20 observations - as “mild illness”.
In 3 cases, mild cognitive impairment was combined with comorbid depression of mild severity (14-16 points on the Hamilton Depression Scale - HAM-D). Another 12 patients had individual depressive symptoms (5-13 points on HAM-D) , the totality of which did not meet the criteria for depressive syndrome, and their manifestations coincided with somatic complaints or overlapped with asthenic symptoms.The average group total score before the start of treatment with Actovegin according to HAM-D was 9.1.
The psychopathological history, along with mild cognitive decline and pseudoneurasthenic disorders, in 5 patients revealed time-bound episodes of psychopathological disorders that occurred 2-3 years before inclusion in the present study. One patient had experienced delirium in the past, another developed depression after an acute cerebrovascular accident (ACVA), and another 3 patients had previously reported psychogenic depressive reactions.
Determination of the neurological history revealed that 9 patients had previously suffered strokes - in 5 cases in the form of transient ischemic attacks (TIA), the remaining 4 patients suffered ischemic strokes (in one of these cases - again). The Hacinski scale score at the beginning of the study ranged from 4 to 10 points (average 6 points). The neurological diagnosis of all patients included in the study was formulated as stage 1-2 dyscirculatory encephalopathy [10].
The condition of the patients before starting treatment with Actovegin was characterized by a complex of symptoms of varying nature and varying degrees of severity. Common to all was a combination of signs of mild cognitive decline and asthenic (pseudoneurasthenic) disorders expressed to varying degrees and extent.
The reason for seeking medical help was primarily complaints of forgetfulness and various manifestations of asthenia. Manifestations of forgetfulness were described by patients as difficulties in memorizing or recalling, loss of natural ease in choosing words, “as if something had stopped.” Patients complained of absent-mindedness, slowed intelligence, admitted that it was “not easy for them to collect their thoughts” and remember recent intentions, especially when attention was distracted, but, as the patients noted, they could subsequently spontaneously remember what was necessary. Most patients, with rare exceptions, complained of frequent or constant headaches, sometimes only in one half of the head, but more often without clear localization, or heaviness in the head, described painful sensations in the head in the form of “tightening with a hoop” or “pressure on the eyes, on your ears." In addition, many patients complained of constant “ringing” in the ears, noise, and “hum” in the head.
The next most common complaints were unsteady balance, unsteadiness when walking, or a feeling that “the ground is falling away from under your feet.” In addition, patients noted the rapid onset of fatigue after light exertion, even after eating, making the bed, fatigue and decreased performance, weakness with a desire to lie down. The deterioration of general well-being was accompanied by sleep disturbances, difficulty falling asleep, a decrease in the depth and duration of sleep, abundant vivid dreams of sometimes frightening content or tiresomely changing meaningless content, in some observations with hypnagogic visual illusions of perception. Morning awakening was characterized by difficulties in the transition from sleep to wakefulness, and a lack of feeling of rest after sleep. Some patients complained of daytime sleepiness and drowsiness that interfered with their usual activities.
Patients noticed the appearance of tearful touchiness or heightened sensitivity to ordinary impressions from what they saw or heard. Mood instability was characterized by the ease of reactions of irritation and impatience; patients often noticed an increase in these manifestations after a restless night with frequent awakenings. A tendency toward a pessimistic assessment of everyday phenomena and life events could be combined with an influx of unaccountable anxiety and worry. The content of anxious fears often determined the appearance of forgetfulness and concentration on the disease as a whole or individual disorders.
In the mental state, manifestations of bradyphrenia were revealed with a slow pace of thinking and speech, difficulties concentrating attention, its instability and exhaustion, which was clearly revealed during testing and was manifested by difficulties in maintaining an activity program, distractibility, forgetting a task, and a slow pace of completion. At the same time, the patients willingly underwent the testing procedure, and when they noticed their mistakes or when shortcomings were pointed out, they lamented or sadly ironized about the weakening of memory or intelligence. Initial manifestations of difficulties in naming the proposed objects or images were compensated for by replacing or describing their purpose, while a minimal sound prompt quickly led to the desired result. Hesitations and pauses when choosing words, slowness of speech were combined with thoroughness and excessive detail, getting bogged down in details or with repeated repetition of what has already been said. Emotional lability was manifested by episodes of tearful weakness against the background of a predominantly complacent background of mood or the emergence of anxiety against the background of low mood.
Basic clinical and demographic data regarding the examined patients are presented in Table. 1
.
Magnetic resonance imaging (MRI) of the brain in the vast majority of patients revealed: expansion of the subarachnoid spaces - in 25 (83.3%) patients out of 30 and enlargement of the cerebral ventricles - in 26 (86.7%) patients. In 18 (60%) patients, post-ischemic foci of small volume located periventricularly were found: single up to 1.5 cm in diameter in 7 (23.3%) patients or multiple small ones in 11 (36.7%) patients. Leukoaraiosis was noted in 19 (63.3%) cases. In general, according to MRI data, signs of dyscirculatory encephalopathy were confirmed in almost all patients.
In the patients included in the study, the polymorphism of the apolipoprotein (ApoE) genotype was determined using a blood test. In two thirds of the observations, patients had the ApoE4(-) genotype with the following distribution of &egr;2 and &egr;3 alleles: 3.3, 3.2, 2.3 (51.9, 3.7 and 11.1%, respectively). 7 patients (25.9%) had the ApoE4(+) genotype, including 3.4, 4.4 and 2.4 (25.9, 3.7 and 3.7%, respectively). Various types of somatic pathology were identified in the patients included in the study (Table 2)
.
80% of patients suffered from arterial hypertension. More than half of the patients were diagnosed with coronary heart disease; in one third of these cases, disturbances in cardiac conduction and rhythm were noted.
results
Clinical positive dynamics in the process of treatment with Actovegin was expressed in a decrease in complaints, patients about “gained strength.” The feeling of dizziness, according to them, occurred noticeably less frequently, the unsteadiness of gait and instability of balance disappeared. In a number of cases, a decrease in the painful sensation of noise in the head or ears was also noted. Patients also noted improved night sleep, decreased fatigue, and increased activity and performance. The improvement in mood was accompanied by a decrease in the level of anxiety and de-actualization of overvalued fears (according to the patients, “it was as if they were wearing a filter”). While forgetfulness remained, patients showed a lesser tendency to fixate on these manifestations.
It was noteworthy that already from the 2nd week of treatment in patients whose condition before the start of therapy showed signs of subdepression or individual depressive symptoms, the general background of mood improved, and this positive dynamics persisted until the end of the course administration of Actovegin and even a month after its ending.
Along with a decrease in complaints, a reduction in asthenic disorders, restoration or increase in emotional stability, disturbances in cognitive functioning experienced significant positive dynamics. First of all, this relates to improving concentration and reducing inhibition. The acceleration of the pace of mental activity was manifested in faster answers to questions and an improvement in the pace of activity when completing test tasks. In some cases, there was a clear decrease in the torpidity of thinking and the manifestations of bradyphrenia in general. Activity and initiative in conversation and communication increased, and daily activities were restored to the required extent. The manifestations of speech difficulties decreased, hesitations and pauses disappeared in spontaneous speech, and patients coped with naming faster and better. Dysmnestic disorders noticeably decreased in their severity, which was reflected in an increase in the volume of memorization or in a greater ease of reproducing consolidated information. It is important to note that this effect turned out to be quite stable and persisted a month after completion of Actovegin administration, when patients did not receive any other treatment other than maintenance therapy for somatic diseases.
Changes in the condition of patients during therapy and during the follow-up period are shown in the figure.
.
Figure 1. Effectiveness of Actovegin therapy according to the CGI scale. 1 - minimal deterioration, 2 - no improvement, 3 - minimal improvement, 4 - moderate improvement, 5 - marked improvement. An improvement in the general clinical condition in the studied group of patients by the 14th day of therapy was noted in 96.7% of cases, including minimal improvement in 73.4% of patients and moderate improvement in 23.3% (see figure)
. In 1 patient, by the 14th day of treatment, the condition slightly worsened. By the time the course of therapy was completed (28 days), the overall frequency of improvement of varying degrees of severity remained the same (96.7%), however, moderate improvement was found in 66.7% of patients, pronounced improvement was achieved in 13.3% of patients, and only in 16.7% of patients showed minimal improvement. In 1 patient the condition did not change. 28 days after the end of the course of treatment, i.e. on day 56, the rate of improvement of varying severity was 100%. Moderate improvement was observed in 76.7% of patients, pronounced improvement was found in 13.3% of cases, minimal improvement in 10% of cases.
There was a statistically significant improvement on the MMSE scale ( p
<0.01) cognitive functions at each stage of the course of therapy: before treatment - 26.8±1.3 points, after 14 days - 28.0±1.3 points, after 28 days - 28.5±1.0 points and on the 56th day - 28.6±1.2 points.
Compared with the period before treatment, all indicators reached a degree of statistical significance ( p
<0.01). Moreover, by the 56th day of the study (28 days after completion of the course of treatment), the total score on the scale turned out to be even higher than the score at the end of the course of therapy.
There was a statistically significant increase in the number of words named within 1 minute (starting with the letter “k”): on the 14th day - 14.2±3.9; on the 28th day - 14.7±3.9 and on the 56th day - 15.5±2.5 compared to the period before treatment - 11.3±3.9 ( p
<0,01).
There was a significant improvement on the frontal dysfunction scale ( p
<0.01) was noted in the “Conceptualization” and “Sound Associations” tests - by the 14th and 28th days of the treatment course, as well as by the 56th day of the study, i.e.
28 days after the end of Actovegin administration (Table 3)
.
Scores on the tests “Simple choice reaction” and “Complicated choice reaction” reached a statistically significant value by the time the treatment course was completed ( p
<0.01). There was no improvement in the total score on the Dynamic Praxis test.
The clock drawing test score improved statistically significantly ( p
<0.01) at each stage of the course of therapy and after completion of treatment: before treatment - 8.3±1.8; 14th day - 9.1±1.6; 28th day - 9.3±1.5; 56th - 9.6±1.1.
According to the Boston Naming Test, the total group number of independent correct answers statistically significantly improved ( p
<0.01) at each stage of the course of therapy and after completion of treatment: before treatment - 42.7±6.8; on the 14th day - 46.2±5.6; on the 28th day - 49.1±5.1; on the 56th day - 49.5±5.4.
According to the Mattis Dementia Scale in the “Similarities” and “Memory” tests, there was a statistically significant improvement ( p
<0.01) was noted on the 14th and 28th days of treatment, as well as after 4 weeks of follow-up
(Table 4)
.
There was no improvement in total scores on the “Reciprocal Coordination” and “Graphomotor Test” tests.
According to the 10-word memorization test, there was a statistically significant improvement in total scores during 1, 2, and 3 attempts to memorize words ( p
<0.01) was noted on the 14th and 28th days of the course of treatment, as well as on the 28th day of follow-up
(Table 5)
.
A statistically significant improvement in the total assessment of delayed word recall was achieved by the 28th day of therapy.
The statistically significant level of its improvement remained after 4 weeks of follow-up observation, although the degree of improvement in the total assessment decreased somewhat. According to the HAM-D scale, a statistically significant improvement in the total group score is M±SD ( p
<0.01) was noted by the 14th day - 5.8±3.2 points and the 28th day - 3.9±3.1 points of the course of treatment, as well as by the 28th day of follow-up - 3.9 ±3.7 points compared to the period before treatment - 8.8±4.5.
There were no adverse events during treatment with Actovegin during the study.
Discussion
The incidence of mild cognitive impairment, not reaching the level of dementia, is extremely high among elderly patients in general somatic institutions. However, there is a certain paradox in the clinical thinking of internists, when a diagnosis of cerebrovascular disease is easily made, often only on the basis of so-called “vascular” complaints and nonspecific neurological symptoms, while complaints of elderly patients about forgetfulness or statements of dysmnestic disorders are regarded as age-related characteristics of cognitive status. Accordingly, medical prescriptions are limited to the prescription of antihypertensive therapy, less often in combination with antiplatelet agents and vasodilators, and the correction of cognitive impairment is considered an optional measure, sometimes left to the discretion of patients.
Assessing the condition of patients urgently requires the study of cognitive functions, especially since complaints of elderly people about weakened memory, impaired ability to concentrate, decreased productivity, and fatigue are often the leading ones when visiting a doctor and determine the search for help.
In the genesis of cognitive impairment, a predominant role is given to ischemic brain lesions, both focal and diffuse, with special importance attached to subcortical lesions. One of the main pathogenetic factors is arterial hypertension (AH) and vascular lipohyalinosis. In these conditions, when there is a decrease in blood pressure or circadian blood pressure fluctuations, heart failure, or inadequate antihypertensive therapy, hypoperfusion occurs in the areas of the terminal circulation (deep structures). A marker of the presence of chronic ischemia is leukoaraiosis as a neuroimaging sign of demyelination, gliosis, and expansion of perivascular spaces.
The leading role in the pathogenesis of cognitive disorders of vascular origin is played by damage to the deep parts of the white matter and basal ganglia, which leads to disruption of connections between the frontal lobes and subcortical structures (disconnection phenomenon).
The results of an open, uncontrolled study of the effectiveness of a course of treatment with Actovegin with daily intramuscular administration of the drug at a dose of 200 mg demonstrated a significant improvement in the condition of the vast majority of patients with MCI syndrome of vascular origin. There was a significant improvement in group average indicators in almost all tests used to assess cognitive dysfunction. It should be noted that the drug in the studied dosage form has an undoubted effect on improving concentration, accelerating the pace of mental activity and memory processes.
The data obtained correspond to the indications given in the literature on the improvement of cognitive functions in cerebrovascular insufficiency under the influence of treatment with Actovegin [6, 7, 10, 17]. Although it is not possible to reasonably judge the antidepressant properties of the drug, one cannot ignore the fact that during treatment with Actovegin there was a decrease in the severity or disappearance of depressive symptoms, especially since none of the patients received antidepressant therapy during the period of treatment with Actovegin. A decrease in the severity of affective disorders as a result of treatment with Actovegin was previously noted in a study by Kuntz (2004), where depressive disorders were detected in 53.3% of patients with MCI.
Of particular interest is the fact that the positive therapeutic effect continued to increase after the end of the Actovegin therapy course, which indicates not only the persistence of the improvement, but also its possible impact on the mobilization of compensatory mechanisms.
[]MCI syndrome in a number of works by domestic neurologists [3] is called moderate cognitive disorder (MCI).
List of used literature
- Karpov Andrey Vladimirovich “Complex treatment of patients with critical ischemia of the lower extremities.” Abstract for the degree of Doctor of Medical Sciences. St. Petersburg, 2007;
- Morozov Mikhail Yurievich “Evaluation of the effectiveness of mydocalm, emoxipin and actovegin in the complex treatment of patients with obliterating atherosclerosis of the lower extremities.” Abstract for the academic degree of Candidate of Medical Sciences. Saransk, 2007;
- Mainugin S. V., Fomin A. A., Krasavin V. A., Krasavin V. G., Averin S. V., Kamensky S. Yu., Khudoyarov T. A. “First experience in using laser Doppler imaging technology when choosing the level of amputation of the lower limb in patients with critical ischemia // Thrombosis, hemostasis and rheology”. – 2012, No. 3;
- Fomin A. A., Mainugin S. V., Krasavin V. A., Kazmiruk N. A., Kamensky S. Yu., Khudoyarov T. A. “Laser Doppler visualization in the practice of the department of purulent surgery // Thrombosis, hemostasis and rheology" - 2012, No. 4;
- Brecht M., de Grool H. “Protection from hypoxic injury in cultured hepatocytes hy glycine, alanine and serine. Amino Acids." 1994. Vol.6. P. 25-35.
diabetes ischemia lower limb ischemia surgery