Atherosclerosis is a chronic disease of the arteries, which occurs due to disturbances in fat and protein metabolism and is accompanied by the deposition of cholesterol and lipoproteins on the inner walls of blood vessels. These deposits form in the form of plaques. Due to the subsequent proliferation of connective tissue (sclerosis) and calcification of the vessel walls, deformation and narrowing of the lumen occurs, leading to blockage of the vessel. The main danger of atherosclerosis is a significant increase in the risk of developing coronary heart disease. Due to the fact that the disease is becoming the main cause of this and other serious health problems, the prevention and treatment of atherosclerosis must be given due attention.
Treatment of atherosclerosis is complex and includes a number of measures related to lifestyle correction, dietary changes, giving up bad habits, as well as drug treatment that helps restore normal metabolism in the body.
What it is
Atherosclerosis is one of the most common chronic arterial diseases. Because of it, an atherosclerotic plaque of cholesterol (cholesterol) forms in the wall of the vessel. These plaques narrow the lumen of the vessel, which affects blood flow, and in extremely advanced cases, plaques can completely block the blood flow. If this happens in a large artery, then the situation is fraught with serious complications, including death: cardiovascular diseases have been one of the main causes of mortality for many years. In addition, the presence of a plaque in a vessel changes the flow of blood: turbulence appears, which contributes to the formation of blood clots (platelet sticking together). The appearance of blood clots poses a risk of their breaking off and clogging the vessel in a narrow place.
Shall we dance?
But what to do in cases where the pressure does not just jump, but seems to dance around normal values - sometimes falling slightly below the normal level, sometimes rising a little higher? To be treated or not? Doctors believe that the following measures have a good effect at the initial stage of arterial therapy.
Diet
The basis of the diet of a “beginner hypertensive patient” is vegetables, fruits and cereals. Low-fat dairy products, fish, lean meat (preferably veal) are allowed. Difficult to digest, salted, fried, smoked, canned foods that complicate the course of hypertension should be excluded.
An important point is that it is necessary to control the consumption of salt, which retains fluid in the body, thereby increasing blood pressure. It has been proven that reducing salt intake to 5 g per day (a full teaspoon of salt is 7 g) lowers blood pressure by about 10 mmHg. Art. This is comparable to the effect of taking antihypertensive drugs.
Article on the topic
Diagnosis: hypertension.
Is self-medication justified for this disease? Physical activity
The same effect (decrease in blood pressure by 10 mm Hg) is achieved by feasible physical activity. Running, swimming, and dancing work best. With such exercises, the blood is saturated with oxygen and the condition improves.
Proper sleep
7–8 hours is the minimum nightly rest that the heart needs to recover. Frequently recurring sleepless nights are a direct path to persistent hypertension.
Calm
There are several theories as to what triggers hypertension. Most doctors are inclined to think that chronic stress is the basis of this disease. And the best effect in the initial stages is provided by such methods of dealing with it as psychotherapy, meditation, etc.
Causes and prevention of atherosclerosis
The cause of atherosclerosis is a disorder in fat metabolism - the accumulation of cholesterol (namely low-density lipoproteins) in excess quantities. Cholesterol is necessary for the body because... participates in many important processes such as the production of certain hormones, and is also part of the cell membrane. With a genetic predisposition to the accumulation of cholesterol, with an unbalanced diet, this substance becomes too much, the body cannot cope with its breakdown, and the excess begins to be deposited in the walls of blood vessels, leading to atherosclerosis.
Factors contributing to the development of atherosclerosis are considered to be: high blood pressure, diabetes mellitus, excess weight, stress, smoking, alcohol, age over 50 years. It is worth noting that the development of the disease often begins at a young age, and by the age of 50-60 the main symptoms appear.
A good method of preventing atherosclerosis is an active lifestyle, balanced physical activity and the fight against excess weight, if present.
Most resources also offer a balanced diet, or more precisely, reducing the consumption of animal fats as the main method of preventing atherosclerosis, i.e. the appearance of excess cholesterol. But some studies indicate that vegetable fats and carbohydrates can provoke an increase in blood cholesterol levels. Therefore, in your approach to your own nutrition, you should be guided by common sense and moderation. Both animal and vegetable fats are necessary for the body to function comfortably, and their excess (like an excess of any other substances) can lead to lipid metabolism disorders. But all researchers agree that consuming vegetables and fruits, adding fish to the diet, and moderate calorie intake are key and proven methods for preventing problems with blood vessels and more.
Consequences of atherosclerosis
Since atherosclerosis is based on a disorder of lipid (fat) metabolism in the body, leading to damage to the walls of blood vessels, the disease can contribute to partial or complete disruption of the functions of any organ. The consequences of atherosclerosis can pose a serious danger to human health and life. The main possible complications include the following.
Coronary heart disease. Atherosclerosis can lead to the development of heart rhythm disturbances, angina pectoris, myocardial infarction and sudden cardiac arrest, since the narrowing of the coronary vessels leads to the fact that the heart muscle does not receive enough oxygen, and the heart, compensating for its deficiency, strengthens its work.
Brain dysfunction. Without treatment, cerebral atherosclerosis can lead to deterioration of blood supply to the brain and, as a result, stroke, paralysis, systematic headaches, dizziness, visual and hearing disorders, swallowing and speech disorders, etc. Deterioration of blood circulation in the tissues of the eyes leads to a gradual decrease in visual acuity, which cannot be compensated. Therefore, it is important to pay timely attention to the treatment of cerebral atherosclerosis.
Thrombosis of the mesenteric arteries. Atherosclerosis can provoke acute blockage of the arteries that supply blood to the intestines, as evidenced by severe abdominal pain.
Shriveled kidney. Lack of oxygen in the tissues can lead to the gradual destruction of the kidney tissue, in its place connective scar tissue forms. The kidney decreases in size and partially loses its functions.
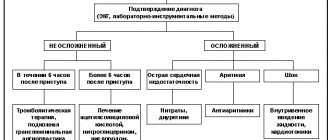
Diagnostics
To diagnose atherosclerosis, both laboratory and instrumental methods can be used:
- general blood analysis;
- blood cholesterol level test;
- angiography (injection of a contrast agent into the blood, which reflects X-ray radiation and gives the specialist a detailed map of the condition of the vessels of the entire body);
- CT, MRI;
- coronary angiography (to study the coronary arteries);
- ECG, echocardiography (echocardiography);
- Holter ECG monitoring (to detect disturbances in heart rhythms);
- Ultrasound (to study the condition of the aorta, kidney vessels, heart).
Diagnostics usually does not cause problems for an experienced doctor - for this, our center has all the necessary equipment. After all, modern high-tech devices will be required - the better the equipment, the more detailed the examination data will be, which will help the doctor choose the optimal treatment method.
Literature
1. Pavlova O.S. Modern possibilities of effective cardiovascular prevention in patients with arterial hypertension and dyslipidemia. Honey. news. 2012; 1:62–68. 2. Arterial hypertension, lipid metabolism disorders and atherosclerosis. V.V. Kukharchuk. In “Guide to Arterial Hypertension” / Ed. E.I.Chazova, I.E.Chazova. M.: Media Medica, 2005; 289–299. 3. Klahr S., Morrissey JJ The role of vasoactive compounds, growth factors and cytokines in the progression of renal disease. Kidney Int. 2000; 57; Suppl 75:7–14. 4. Wolf G. The Renin-Angiotensin System and Progression of Renal Disease. Jn: Contributions to Nephrology. Editor G. Wolf. 2001. 5. Delcayre C., Swynghedauw B. Molecular mechanisms of myocardial remodeling. The role of aldosterone. J. Mol. Cell. Cardiology. 2002; 34:1577–1584. 6. Ross R. Atherosclerosis an inflammatory disease. N Engl J Med. 1999; 340:115–26. 7. O'Donnell VB. Free radicals and lipid signaling in endothelial cells. Antiox Redox Signal. 2003; 5: 195–203. 8. Wolfrum S., Jensen KS, Liao JK Endothelium-dependent effects of statins. Arterioscler Thromb Vasc Biol. 2003; 23: 729–36. 9. Kaplan M., Aviram M. Oxidized low density lipoprotein: atherogenic and proinflammatory characteristics during macrophage foam cell formation. An inhibitory role for nutritional antioxidants and serum paraoxonase. ClinChem Lab Med. 1999; 37:777–87. 10. Campese VM, Bianchi S., Bigazzi R. Association between hyperlipidemia and microalbuminuria in essential hypertension. Kidney Int. 1999; 56(Suppl 71):S10–3. 11. Diagnosis and treatment of arterial hypertension. Systemic hypertension. 2010; 3:5–26. 12. Oshchepkova E.V., Dmitriev V.A., Titov V.N. et al. Indicators of nonspecific inflammation in patients with hypertension. Ter. Arch. 2007; 12: 18–25. 13. Breiser A., Recinos A., Eledrisi M. Vascular inflammation and the renin-angiotensen system. Atherioscler. Thromb Vasc. Biol. 2002; 22; 1257–1266. 14. Verma S., Bucshanan M., Anderson T. Endothelial function testing as a biomarker of vascular disease. Circulation. 2003; 108:2054–2059. 15. Sesso H., Burning J., Rifai N. et al. C-reactive protein and the risk of developing hypertension. JAMA. 2003; 290:2945–2951. 16. Niscanen L., Laaksonen D., Nyssonep K. et al. Inflammation, abdominal obesity and smoking as predictors of hypertension. Hypertension. 2004; 44(6):859–865. 17. Fliser D., Buchholz K., Haller H. For the European Trial on Olmesartan and Pravastatin in Inflammation and Atherosclerosis (EUTOPIA) Investi Circulation. 2004; 110:1103–7. 18. Stumpe KO, Agabiti-Rosei E., Zielinski T. et al. Carotid intima-media thickness and plaque volume changes following 2-year angiotensin II-receptor blockade. The Multicentre Olmesartan atherosclerosis Regression Evaluation (MORE) study. Ther. Adv. Cardiovasc. Dis. 2007; 1:97–106. 19. Smith RD, Yokoyama H, Averill DB et al. The protective effects of angiotensin II blockade with olmesartan medoxomil on resistance vessel remodeling (The VIOS study): rationale and baseline characteristics. Am J Cardiovasc Drugs. 2006; 6 (5): 335–42. 20. Smith RD, Yokoyama H., Averill DB, Schiffrin EL, Ferrario CM Reversal of vascular hypertrophy in hypertensive patients through blockade of angiotensin II receptors. J Am Soc Hypertens. 2008; 2: 165–172. 21. Hirohata A., Yamamoto K., Miyoshi T. et al. Impact of olmesartan on progression of coronary atherosclerosis a serial volumetric intravascular ultrasound analysis from the OLIVUS (impact of OLmesartan on progression of coronary atherosclerosis: evaluation by intravascular ultrasound) trial. J Am Coll Cardiol. 2010; 55 (10): 976–82. 22. Naya M., Tsukamoto T., Morita K. et al. Olmesartan, but not amlodipine, improves endothelium-dependent coronary dilation in hypertensive patients. J Am Coll Cardiol. 2007; 50 (12): 1144–9. 23. Lorenzen JM, Neuhoeffer H., David S. Angiotensin II receptor blocker and statins lower elevated levels of osteopontin in essential hypertension – results from the EUTOPIA trial. Atherosclerosis. 2010; 209(1):184–8. 24. Takiguchi S., Ayaori M., Uto-Kondo H. et al. Olmesartan improves endothelial function in hypertensive patients: link with extracellular superoxide dismutase. Hypertens Res. 2011; 34 (6): 686–92. 25. Pimenta E., Oparil S. Impact of olmesartan on blood pressure, endothelial function and cardiovascular outcomes. Integr Blood Press Control. 2010; 3:113–23. 26. Hirohata A., Yamamoto K., Miyoshi T. et al. Four-year clinical outcomes of the OLIVUS-Ex (impact of Olmesartan on progression of coronary atherosclerosis: evaluation by intravascular ultrasound) extension trial. Atherosclerosis. 2012; 220(1):134–8. 27. Brunner HR The new oral angiotensin II antagonist olmesartan medoxomil: a concise overview. J Hum Hypertens. 2002; 16(Suppl. 2):S13–16. 28. Corsini A. et al. Blood Pressure. 1998; 7(Suppl 2): 18–22. 29. Catapano A. Cardiologia. 1997; 42(Suppl 3): 19–26.
Atherosclerosis of the cerebral arteries
When cholesterol plaques form and the arteries of the brain narrow, the brain cells experience a lack of blood and nutrients. The following symptoms may indicate this condition:
- periodic dizziness,
- noise in ears,
- headache,
- increased fatigue,
- disturbances in coordination of movements.
The narrowing of the main carotid artery supplying the brain is identified as a separate diagnosis - carotid artery stenosis. Damage to the vessels supplying the brain carries the threat of a serious disease - ischemic stroke of the brain.
Causes of vascular atherosclerosis
There are many theories about the development of atherosclerosis, they are mainly associated with lipid metabolism disorders, hereditary factors, inflammation, poor environmental conditions, etc. For example, according to one version, the cause of the pathology lies in the presence of an infection in the body (chlamydia, cytomegalovirus, etc. ). The theory is supported by the fact that an immune test in the blood of some patients with atherosclerosis detects antibodies to these pathogens. However, what really leads to vascular atherosclerosis is not known for certain.
The causes of atherosclerosis are usually divided into correctable (depending on the person) and non-correctable .
The first group includes:
- Hypertonic disease;
- smoking;
- obesity, craving for fatty foods;
- diabetes;
- adynamia.
The second group includes:
- Gender - men get sick earlier and under 50 years of age - more often; women usually “join” them after menopause and quickly “catch up” in terms of incidence;
- age - aging of the body inevitably causes changes in blood vessels;
- hereditary factor.
1 Bicycle ergometry for atherosclerosis
2 VEM for atherosclerosis
3 ECG - diagnosis of atherosclerosis
Atherosclerosis of the arteries of the lower extremities
Damage to the arteries of the lower extremities is called obliterating atherosclerosis. People over 65 years of age, especially men, are susceptible to it. This disease manifests itself in the following symptoms:
- pain in the calves, cramps at rest;
- pain when walking, causing you to limp;
- numbness in the legs, fatigue when walking;
- the appearance of non-healing wounds, and in advanced cases - ulcers.
If you do not consult a doctor in the presence of such symptoms, then there will be a threat of limb amputation as the only treatment measure for extremely advanced cases of obliterating atherosclerosis.
Symptoms of atherosclerosis
Symptoms of atherosclerosis (impaired blood supply to tissues) are:
- cold extremities and a change in their color to bluish-white;
- discomfort in the heart area, rapid heartbeat;
- memory impairment and poor concentration;
- change in mood to predominantly nervous and irritable;
- feeling of general fatigue and weakness.
Symptoms of cerebral atherosclerosis are cerebral ischemia and deterioration of brain functions, which is manifested by weakening of memory, decreased intellectual abilities, and changes in the psyche. Atherosclerosis of the renal arteries causes renal ischemia and arterial hypertension. Symptoms of atherosclerosis of the arteries of the legs are cold feet, pain in the calves while walking. In addition, ulcers may appear and, in severe cases, gangrene may develop. Atherosclerosis of the mesenteric arteries is manifested by dysfunction of the gastrointestinal tract and intestinal necrosis, including pain in the upper abdomen.
When the first signs of atherosclerosis appear, you should immediately consult a doctor, since at an early stage of development the process can be stopped by changing your lifestyle.
Atherosclerosis of the coronary arteries
Atherosclerosis of the coronary arteries (which bring blood to the tissues of the heart) is one of the main causes of coronary heart disease and myocardial infarction: when the disease affects the vessels of the heart, heart muscle cells begin to die due to insufficient nutrition. And the risk of blood clot formation and vessel blockage only aggravates the situation. This condition is extremely dangerous, life-threatening and requires consultation with a doctor. You should pay special attention to possible symptoms:
- chest pain;
- feeling of heaviness, tightness in the chest;
- arrhythmia, i.e. fast or slow heartbeat;
- feeling of a sinking heart.
Do not underestimate the above symptoms. Let us remember that the risk of developing atherosclerosis is present in many people. Complications of the disease without proper treatment are so dangerous that you should consult a doctor, even if you are afraid of a confirmed diagnosis or surgery. Modern medicine has advanced far in the treatment of atherosclerosis of various localizations.
New approaches to the use of statins in the treatment of atherosclerosis
Over the last decade of the last century, mortality from cardiovascular diseases in Russia more than doubled. Especially high rates of growth in mortality rates from these diseases were observed among young (20-30 years old) and middle-aged (40-50 years old) people (E.I. Chazov, 2003). If this trend continues, Russia will lose a significant number of working-age citizens every year. Today, decisive measures are needed to introduce programs for primary and secondary prevention of cardiovascular diseases, to improve treatment methods, and to expand the use of modern methods of surgical care for patients with coronary heart disease. Statins can be very useful in solving a number of these problems. Their unique properties, such as ease of use, proven safety and high efficiency, determine the paramount importance of this group of drugs. At the same time, statins have proven to be an effective means of both primary and secondary prevention of cardiovascular diseases.
As can be seen from Table 1, pravastatin and lovastatin were used in two studies on primary prevention of coronary heart disease (CHD) with a total number of patients of more than 13 thousand people with risk factors. In a study using pravastatin (the WOSCOPS study), overall all-cause mortality decreased by 22% over five years, and coronary mortality itself decreased by 33%. Approximately the same results were obtained in a well-known American, Texas, study with lovastatin. Over five years, fatal and nonfatal myocardial infarctions were reduced in the observed population by 40%, the need for revascularization by 33%, and major coronary events occurred 37% less often than in the placebo group.
The number of patients suffering from manifest coronary heart disease in Russia amounts to millions, while secondary prevention programs are practically absent.
As can be seen from Table 2, in five evidence-based secondary prevention studies involving a total of approximately 40,000 patients with coronary heart disease, it was found that taking simvastatin reduced the risk of mortality over five years. from coronary heart disease by 42%, total mortality from all causes - by 30%. Trials with pravastatin (CARE, LIPID) also found a reduction in coronary and total mortality, but more moderate than that found in the study with simvastatin. A fairly high effectiveness of fluvastatin was observed when the drug was used for six months, which suggests that all statins have the ability to reliably and significantly reduce not only the risk of coronary events, including death from them, but also overall mortality rates.
What explains the dramatic success of statins? As studies on primary and secondary prevention have shown, using methods that affect only the level of low-density lipids (LDL), the divergence in the survival curves of patients in the control and main groups begins to appear only after three and a half years. We are talking about studies with small intestinal bypass (POSCH, 1990) and with cholestyramine (Brensike et al., 1984). In these studies, only hypocholesterolemic effects were exerted.
In studies with statins in both primary and secondary prevention, a discrepancy in survival curves between patients in the main and control groups was detected after a year and a half. In other words, statins have a much more significant effect than just a lipid-lowering effect on low-density lipids. These effects, not associated with a decrease in lipidemia, are called pleiotropic, i.e., additional, and, as it turns out, play a significant role in the formation of the early and late effects of statins. If, based on the above results of clinical studies, it was possible to establish that statins, compared with purely lipid-lowering methods of treatment, are more effective and act faster, then studies with dynamic coronary angiographic control have shown that the cessation of progression of coronary atherosclerosis, the prevention of new cases of atheromatosis and even partial regression of atheromatous plaques in the coronary and other large arteries are also observed two years earlier than with the use of lipid-lowering effects alone. Pleotropic properties are due to various, not yet fully understood mechanisms, but the main ones are definitely associated with the improvement under the influence of statins of endothelial functions impaired in atherosclerosis.
Since pleotropic effects appear already in the coming days and weeks from the onset of the disease, they play an important role in stabilizing the so-called unstable atheromatous plaques. At the same time, statins:
- reduce the volume of a large lipid core consisting of semi-liquid cholesterol esters due to their resorption;
- suppress the inflammatory process that necessarily accompanies unstable atheroma by reducing the release of cytokines, inflammatory mediators (tissue necrosis factor), interleukin-I and interleukin-6 by activated macrophages;
- protect the fibrous membrane of the plaque from destruction by metalloproteases produced by activated macrophages;
- suppress the tendency to thrombus formation at the local and systemic levels;
- increase the vasodilator reserve of arteries. Thus, statins help stabilize unstable atheroma over the next 6-14 weeks, preventing dramatic (acute myocardial infarction, unstable angina, stroke) and tragic clinical outcomes (sudden death; Ridker et al., 2000, Fruchert JF, 2002).
In a study by Horne et al. (2000), conducted in patients with acute myocardial infarction (AMI) who randomly received placebo or simvastatin, it was found that treatment with statins from the first days of the patient’s admission to the hospital had an early beneficial effect, expressed in a rapid divergence of survival curves after two months ( see figure 1).
By the end of the four-year follow-up period, the difference in survival reached high degrees and was especially different in patients who had the highest blood level of C-reactive protein (CRP) during acute myocardial infarction (5th quintile of the distribution). Control patients with similarly high CRP levels had a mortality rate of 18.5% during the follow-up period, while patients treated with simvastatin had a mortality rate of only 4.6% (Horne et al. 2000, 36, 6 ). A larger study involving 20,000 patients with acute myocardial infarction, based on data from 58 clinical centers in Sweden, found that one-year mortality in patients treated with statins was more than half (4%) compared with with patients in the placebo group (9.3%). When standardizing by gender, age, and primary clinical data, the identified pattern remained.
But the most convincing data are obtained from the MIRACL study, in which atorvastatin was used in more than 3.5 thousand patients with unstable angina. During the short follow-up period (16 weeks) in the placebo and atorvastatin groups, the cumulative incidence of endpoints (including death from any cause, nonfatal myocardial infarction, resuscitation after cardiac arrest, progressive angina requiring readmission) and the risk of death in the atorvastatin group were found to be decreased by 16% and amounted to 14.8% versus 17.4% in the placebo group. In addition, in this short period of time it was possible to reduce the number of new cases of unstable angina by 40%. This indicates that patients with acute coronary syndrome, including patients with myocardial infarction, stable angina, and those who have undergone surgical invasive or non-invasive intervention on the coronary arteries, require statins from the first days of admission to the hospital, regardless of the level of cholesterolemia. We remind you that a significant proportion of so-called coronary deaths occur in cases associated with instability of blood flow in the coronary or cerebral arteries. Stabilization and prevention of atheroma instability in these arterial regions may prevent up to 30% of deaths and nonfatal heart attacks and strokes in a cohort of patients suffering from cerebral coronary atherosclerosis.
Statins play an extremely important role in reducing the serious complications of coronary heart disease during long-term follow-up. One of the most serious and life-threatening complications of coronary artery disease is chronic heart failure. Statins have been found to have the ability to reduce the incidence of new cases of heart failure, as can be seen in Table 3.
In the 4S study, simvastatin reduced the risk of new cases of circulatory failure by 19%, in the UK Heart Protection Study (HPS) by 30%, and pravastatin in the CARE study by 21%. This means that with long-term use, statins have the ability to reduce myocardial dysfunction, maintain normal morphology and pumping function of the myocardium, and maintain hemodynamics at a satisfactory level without the development of congestive heart failure.
In our country, elderly patients are treated with extreme disrespect. Many people believe that various public benefits, including medical care, should be provided to people of working age. The possibility of effective prevention and treatment of elderly patients, including with drugs such as statins, is implicitly and sometimes explicitly questioned. In this sense, the study by W. Aronov et al. is indicative. (2002), during which 1410 patients who had myocardial infarction after 80 years of age were treated. Patients were of both sexes with low-density lipid cholesterol >125 mg/dl. One group of patients with myocardial infarction was treated with statins (simvastatin - 89%, pravastatin 10%, lovastatin - 1%), while patients in the second group did not receive lipid-lowering drugs. The observation period is three years. New cases of heart failure in the statin group developed in 31% of cases, in the control group - in 42%, which means a reduction in the risk of the former by 26%. The incidence of the main endpoint “death + nonfatal myocardial infarction” in the groups was 46 and 72%, respectively (reduction in the risk of “death + nonfatal myocardial infarction” was 64% in favor of those treated with statins). This once again proves the groundlessness of the approach to older people as therapeutically unpromising, and also serves as evidence of the high effectiveness of treating older people with statins.
Statins, stroke and dementia
Statins have a strong effect not only on coronary, but also on cerebral atherosclerosis. Under their influence, in all major clinical trials conducted under the secondary prevention program, a decrease in the number of strokes and deaths from them was observed.
In particular, in The Heart Protection Study (HPS), the number of strokes in patients receiving simvastatin decreased by 27% (2p<0.00001), and ischemic strokes by 35%.
In addition, it has been noted that long-term use of statins (from three years or more) leads in people over 50 years of age to a significant reduction in the incidence of vascular dementia (Jick et al., 2000), including the development of Alzheimer's disease (Wolozin et al., 2000; Lacotelli al., 2003). It has also been established that long-term use of statins (more than three years) prevents the development of osteoporosis and, accordingly, reduces the incidence of pelvic and femoral fractures in elderly patients (Cumming and Bauer, 2000; Wang et al., 2000). Statins reduce the incidence of gallstone disease by reducing the saturation of bile with cholesterol (Batezon, 1990).
Statins and diabetes
Statins have a beneficial effect not only on heart and vascular diseases, but also on other diseases, in particular diabetes. It is known that at the same level of cholesterolemia, mortality among patients with diabetes is two to three times higher than among others. Thus, with a normal level of cholesterolemia ≤ 4.7 mmol/l (180 mg/dl), the mortality rate is seven per 10 thousand; a person with the same level of cholesterolemia in people with diabetes mellitus, the mortality rate increases to 60 per 10 thousand people . (versus seven people per 10 thousand; see Figure 2).
Therefore, patients with diabetes require immediate treatment with statins, regardless of the level of cholesterolemia. It has been shown that the incidence of new cases of diabetes mellitus in people receiving statins in a primary prevention program was reduced by 30% compared with patients in the placebo group (Friman et al., Circulation, 2001, 103, 357-362).
As can be seen from Table 4, statins not only reduce the number of new cases of diabetes mellitus, but also significantly reduce mortality in people suffering from a combination of coronary heart disease and diabetes mellitus. Moreover, in such patients, the effectiveness of statins is much higher than in patients with coronary heart disease alone. This once again confirms that all patients with diabetes need treatment with statins, even with normal cholesterol and low-density lipids. In other words, with a certain degree of certainty it can be said that statins are an antidiabetic drug. In addition, a moderate decrease in glycemic levels was found in patients with diabetes mellitus when treated with atorvastatin (D. Aronov, M. Bubnova, 2003).
As can be seen from this brief review, statins are a unique drug that can be effectively used in primary and secondary prevention programs and lead to a significant reduction in mortality among patients suffering from coronary heart disease and other atherogenic diseases of vital organs.
D. M. Aronov, Doctor of Medical Sciences, Professor of the State Research Center for Medical Sciences of the Ministry of Health of the Russian Federation
Table 4. Diabetes mellitus, coronary risk, statins.
- The presence of hyperglycemia 110 mg/dL or diabetes mellitus doubles the 10-year coronary risk.
- Insulin resistance and the involvement of pathological mechanisms and factors (dyslipidemia, hypertension, endothelial dysfunction, atherosclerotic markers of inflammation, procoagulation factors, etc.), common to diabetes and atherosclerosis, are the main reason for the aggravation of their course.
- Statins significantly reduce coronary risk in patients with diabetes, with: pravastatin by 25% for 5 years
- lovastatin by 43% 5 years
- simvastatin by 55% 5 years
- atorvastatin by 58% 3 years
Hypertension and the nervous system
The nervous system controls and regulates all processes occurring in our body. The extremely complex activity of the nervous system is carried out thanks to two main processes in nerve cells - excitation and inhibition, which constantly restrain and balance each other.
Innervation plays a big role in maintaining the normal functioning of the heart and blood vessels, in particular in the regulation of blood pressure.
What can disrupt the normal coordinated activity of the nervous system? The cause of such a violation may be emotions of a negative nature if they are of great strength, duration or are often repeated (see article Mental Health and Neuroses).
The nervous system, like other organs and tissues of our body, has a certain endurance limit. Stimuli acting on the cerebral cortex that exceed the endurance limit of brain cells can cause them to become overstrained and exhausted. Then the normal interaction, mutual balancing of the processes of excitation and inhibition in the cerebral cortex is disrupted. As a result, the control of the cerebral cortex over the subcortical centers is weakened. These centers begin to function uncoordinated, thereby causing surges in blood pressure.
It should be noted, however, that the cerebral cortex, like other organs, can adapt to different, even unfavorable conditions. The size and scale of such adaptability largely depend on the type and nature of nervous activity. Therefore, in the development of hypertensive fear, an important role is played not only by the extreme strength and duration of negative emotions, but also by insufficient stability
nervous system, its insufficient adaptability to adverse influences, insufficient endurance during nervous shocks. The disease most likely occurs in those whose body is weakened due to one or another infection or other unfavorable factors. We especially note the effect of prolonged overfatigue, when the limit of the working capacity of nerve cells is exceeded and their exhaustion occurs. All this prepares the ground for the disease.
But this is only the first part of the emergence of the so-called pathological circle. Spasm or weak tone of brain vessels leads to disruption of the nutrition of its cells, disruption of oxygen delivery and elimination of waste products. This, in turn, further reduces the adaptive properties of nerve cells and the pathological circle is closed. The body cannot cope with this problem on its own. If adequate treatment measures are not applied, a chronic disease develops.
A chronic pathological condition leads to the development of compensatory functions within the pathological circle. If the vessels are in spasm for a long time and are affected by increased blood pressure, then a change occurs in the vascular wall itself. Consequently, with a drug reduction in blood pressure, the internal diameter of the changed vessel will not allow the required volume of blood to pass through. As a result, a problem arises with the delivery of oxygen and nutrition to the cells. The neurons begin to starve, and the brain tries to compensate for the lack of blood volume by increasing blood pressure, bypassing the drugs. The circle is closed at the next level of pathology development. In this situation, it is necessary to examine cerebral circulation. Consider the blood flow to the brain, its volume and uniform distribution within the vascular beds. But an important factor is the outflow of blood. If it is disturbed, stagnation and tissue swelling may occur, which can cause intense headaches. Determining the level of pathological processes in the blood supply to the brain can be done using Dopplerography, tetrapolar high-frequency computer rheoencephalography (REG).
After conducting a series of studies, you can try to break the pathological circle and begin the healing process.
Diagnosis of atherosclerosis
All diagnostic measures begin with collecting anamnesis and physical examination of the patient, measuring his blood pressure. If necessary, the person is weighed (to calculate the body mass index).
To diagnose vascular atherosclerosis, the following are prescribed:
- biochemical blood test (lipid profile: total cholesterol, LDL, HDL, triglycerides + less often VLDL, LDLP);
- ECG, ECG with exercise (Veloergometry);
- 24-hour ECG monitoring in 12 leads;
- ECHO-CG (ultrasound of the heart and aorta);
- duplex and triplex scanning of arteries;
- magnetic resonance angiography;
- MSCT with contrast of arteries;
- CT scan to determine the accumulation of calcium in the arteries of the heart;
- X-ray contrast examination of the arteries (coronary angiography).
1 Laboratory diagnosis of atherosclerosis: testing
2 Laboratory diagnosis of atherosclerosis: testing
3 Pressure control in atherosclerosis