What is a coma during a stroke? This is a dangerous condition in which a person is literally on the verge between life and death. This complication is characterized by damage and, as a consequence, disruption of the brain, which leads to a complete shutdown of physiological systems.
Coma is considered a protective reaction of our body in order to preserve the remnants of a functioning system; it is for this reason that recovery from a coma after a stroke is possible. Let's take a closer look at this condition.
Why does the patient fall into a coma?
The development of coma is regarded as the result of a disease or pathological process, which is based on:
- damage to the brain stem and reticular formation;
- diffuse lesions of the cerebral cortex.
Without the support of the reticular formation, the cerebral cortex loses activity, the transmission of nerve impulses between neurons is deeply inhibited, and the coordinated activity of brain structures is lost. The brain begins to work autonomously.
The following events disrupt brain function, leading to the development of coma:
- acute cerebrovascular accidents, trauma, infections, epilepsy;
- metabolic disorders due to endocrine pathology, hormonal imbalance;
- intoxication;
- lack of oxygen and the development of hypoxia.
Working offline, the brain loses control over the body. There is a loss of consciousness and reactions to external and internal stimuli.
Etiology
Provoking factors create conditions for damage to the vessel wall and the release of the liquid part of the blood beyond the vascular bed. There are many causes of hemorrhagic stroke. Let's note those that occur most often:
- Hypertension - a malignant form of the disease leads to cerebral hemorrhage in most cases. When pressure surges, the vessels are damaged and do not have time to recover.
- Atherosclerosis - arteries lose their strength and stretch worse when pressure changes.
- Congenital pathologies can cause rupture or dissection of the artery with subsequent hemorrhage.
- Chronic diseases - the cause of vessel rupture can be pathologies of an inflammatory or dystrophic nature. They can also provoke diapedesis.
Less common causes of hemorrhagic stroke include vitamin deficiencies, stress, and heart disease. Usually they aggravate the impact of the main factor and provoke hemorrhage.
There are risk groups that increase the likelihood of developing a stroke several times. Let's list them in descending order:
- hypertension;
- obesity;
- increased cholesterol;
- lack of leukocytes;
- eating disorders;
- stress;
- diabetes;
- hemorrhage in relatives.
How to determine who
In a coma state, the patient has no mental activity and no contact with the outside world. The degree of impairment of consciousness is reliably determined using the Glasgow scale. Response to stimuli, eye opening and speech function are assessed. Reliably confirms who the score is from 4 to 8 points. During the first 24 hours, the degree of coma on the Glasgow scale serves as a prognostic sign of recovery from this state. According to statistics, 80% of patients with an initial score of 7-8 points have a chance to emerge from a coma.
Signs of coma during stroke are determined by the type of cerebrovascular lesion. With hemorrhagic stroke, coma manifests itself:
- sudden loss of consciousness;
- purplish-red complexion;
- snoring breathing;
- on the affected side the cheek is swollen;
- high blood pressure and intense pulse;
- narrowing and sluggish reaction of the pupils to light;
- decreased muscle tone;
- presence of hemiparesis or plegia.
Ischemic brain lesions are less often complicated by the development of a coma. The characteristic symptoms in this case are the following:
- gradual development of depression of consciousness;
- bright cerebral symptoms precede the development of coma;
- pale face;
- breathing may not change, sometimes tachypnea;
- the pulse is soft, arrhythmia is possible;
- An increase in tone in the paralyzed limbs is noted early.
Involvement in the process of areas of the brain in which life support centers and cranial nerve nuclei are located is often complicated by coma.
Degrees of coma during stroke
Coma during a stroke is assessed by the depth of impairment of consciousness. The systematization is based on clinical manifestations corresponding to each stage. Separating the degrees of coma helps determine the prognosis of the disease.
Ischemic-type injuries are often characterized by the presence of precoma. Severe headache, dizziness, vomiting, paresthesia are possible. In the absence of proper attention, further depression of consciousness occurs. With hemorrhagic stroke, events develop without warning.
First degree
The first degree of depression of consciousness is called mild. The initial level of inhibition processes in the cerebral cortex is characterized by:
- complete disorientation;
- motor aphasia;
- increased muscle tone and reflexes;
- distortion of reaction to stimuli;
- constriction of the pupils, nystagmus and strabismus;
- preservation of breathing and cardiac activity;
- involuntary urination and defecation.
Second degree
Second-degree coma will manifest itself as deepening disorders reaching the brain stem. Clinical signs are as follows:
- complete lack of speech;
- tonic convulsions;
- suppression of reflexes;
- miosis, sluggish reaction to light;
- hyperthermia;
- hemodynamic instability;
- breathing disorders.
Even with adequate therapy in older people, the process may spread and develop a deep stage of coma.
Third degree
Third degree coma is considered deep. Disorders occur in the medulla oblongata. The threat to life with a cerebral hemorrhage increases. Signs of this stage are characterized by:
- loss of pain;
- loss of corneal reflexes;
- decreased muscle tone;
- dilated pupils, lack of reaction;
- shallow, arrhythmic breathing;
- decrease in hemodynamics;
- convulsive syndrome.
During the period of deep coma, tissue trophism is disrupted, which contributes to the rapid formation of bedsores.
Fourth degree
The fourth degree coma is called terminal. There are no signs of brain activity. This shows up:
- muscle atony;
- areflexia, dilated pupils;
- cessation of spontaneous breathing;
- inability to determine blood pressure.
Extensive cerebral stroke complicated by coma will have a poor prognosis.
Causes
Who can be called:
- High pressure in any part of the brain, which can lead to hemorrhage;
- Lack of blood supply to any organ;
- Degeneration of vascular walls;
- Defect in the development of vascular walls;
- Deposits in blood vessels;
- Intoxication;
- Blood diseases;
- Acute lack of vitamins.
- In addition, high blood pressure, old age, severe emotional shock and atherosclerosis can increase the risk.
Introduction to an artificial coma after a stroke
Massive damage during a stroke is accompanied by an increase in intracranial pressure, the development of edema and necrosis of brain tissue. Patients are put into a coma during a stroke to avoid such complications. In this case, metabolic processes slow down and cerebral blood flow decreases.
The patient is put into an artificial coma using special drugs. This is always a controlled process. The patient is returned to normal after the swelling is eliminated.
Medically induced coma has a number of consequences that negatively affect the functioning of internal organs. With further treatment, such reactions can be corrected.
How does a person feel
There is no clear and uniform answer to the question of how a person feels while in a coma. But scientists have recorded brain activity when visiting relatives or changes in breathing and heartbeat when trying to communicate with a patient. Many relatives wonder: can a person in a coma hear them?
The people themselves who have experienced such an experience describe their sensations differently: some were conscious, but could not show it, some saw various dreams, and some communicated with deceased loved ones; there are also cases when patients couldn't remember anything.
Care and treatment of patients in a coma
Patients in a coma require special care. Medical supervision and care in the acute period is carried out in the intensive care unit.
The severity of the condition requires artificial ventilation and special care. Parenteral and tube nutrition. Prevention of bedsores, trophic ulcers, and the development of infection is carried out.
Treatment is aimed at ensuring the vital functions of the body. Hemodynamic parameters are monitored.
During the treatment period, the functioning of brain neurons gradually improves and is reorganized. The cells located near the affected area take on the active function.
Nutrition
The patient is provided with adequate nutrition. Feeding occurs through a tube and parenterally. In tube feeding of patients, special mixtures are used, which contain the necessary components.
It is acceptable to use baby food. Solutions for parenteral nutrition contain complexes of vitamins and microelements.
Hygiene
An immobile position and loss of sensitivity quickly lead to tissue trophic disorders and the development of bedsores. Hygiene measures are aimed at daily prevention of these violations.
For this purpose, the following is carried out:
- treatment of the oral cavity with solutions of boric acid, soda;
- treating the skin with soapy water;
- rubbing with camphor alcohol;
- changing body position in bed.
Control urination and bowel function.
Treatment
Therapeutic measures are aimed primarily at maintaining the vital functions of the body. Such measures are taken urgently and regardless of the etiology of the disease.
The patient's breathing is supported by artificial ventilation. Hemodynamic parameters are monitored. Normal levels of blood pressure and circulating blood volume are maintained. In order to correct disorders, symptomatic therapy is used using antiemetic and anticonvulsant drugs. Sedatives are prescribed.
Accurate diagnosis of stroke coma allows etiological treatment.
Surgery in the absence of contraindications increases the chances of recovery for hemorrhagic strokes. Early removal of the hematoma preserves the damaged areas to restore lost brain functions.
Coming out of a coma
When emerging from a comatose state, a gradual restoration of lost connections occurs. Cerebrovascular disorders are accompanied by the death of nerve cells. The task of the rehabilitation period is to prevent the spread of the process. This is only possible with adequate treatment.
The emergence of consciousness makes additional examinations possible for the purpose of further correction of lost skills.
Coma may emerge from a vegetative state, which indicates a poor prognosis for recovery. Only consciousness is restored, and other functions are lost. The patient can remain in this condition for a long time, death occurs from the development of infections and bedsores.
What the awakening will be like depends on the type of violation, the degree of damage, and adequate treatment.
Diagnostics
To accurately identify the disease and differentiate hemorrhage from ischemia, an instrumental examination is performed:
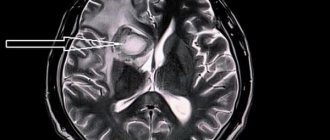
- MRI or CT scan - the images show a limited area of the hematoma. The safety of magnetic tomography allows for multiple examinations and monitoring of neuronal recovery.
- Angiography - shows the condition of blood vessels. Well displays arterial rupture, signs of atherosclerosis and congenital anomalies.
- Lumbar puncture - taking cerebrospinal fluid in the lumbar region for analysis. The diagnosis of hemorrhagic stroke is made when red blood cells are detected in the cerebrospinal fluid in high concentrations.
Recommendations for relatives of patients
Patients require increased attention when emerging from a comatose state. The help and support of relatives during this period is of great importance. It has been proven that the period of functional restoration with the support of relatives is significantly reduced and gives positive dynamics. The risk of repeated cerebral accidents increases with the development of diabetes, lipid disorders, and hypertension.
You can avoid a recurrent stroke and irreparable consequences by doing the following:
- creating a favorable environment;
- motivation to conduct daily classes to restore speech and motor skills;
- obligatory praise for achieved results;
- mastering simple massage skills;
- proper care and nutrition;
- control of blood sugar, cholesterol;
- instilling hope for recovery.
These measures, together with complex therapy, give positive results.
What could be the outcome
Extensive cerebral hemorrhages with the development of coma leave behind consequences, which are presented in the following form:
- recovery from a coma with partial restoration of lost functions;
- exit without restoration of nervous system functions;
- transition to a vegetative state;
- the onset of brain death.
Often, persistent cognitive impairment remains at the end of treatment. Speech is not fully restored, and attention and memory impairments persist.
Major strokes accompanied by coma leave little chance of survival. Such conditions cannot be avoided without the preservation of paralysis and motor impairment. Characterized by frequent mood swings and personality changes.
The consequences of emerging from a coma after a stroke can be complications in the functioning of internal organs and systems. Complications after a long stay in a coma are manifested by pneumonia, cystitis, vascular disorders, and the development of muscle atrophy.
Brain death occurs as a result of hypoxia. Manifested by a lack of breathing, cardiac activity, and consciousness. Life is supported by hardware.
Features of recovery from unconsciousness
A distinctive feature is the return of an adequate state in the opposite manner of oppression. With positive dynamics, muscle and skin reflexes appear. The patient begins to swallow and respond to pain. The return of consciousness is combined with episodes of delirium and hallucinations. Speech, memory, coordinated movements require long-term rehabilitation.