Features of the course and treatment of hypothyroidism in patients with coronary heart disease
Why is it important to promptly stop the manifestations of hypothyroidism in patients with coronary artery disease, and especially in the elderly? What causes the difficulty in diagnosing hypothyroidism in the elderly? What is the difficulty of managing patients with coronary artery disease and concomitant hypothyroidism?
The steady increase in the number of thyroid diseases observed in recent years has forced practicing doctors of various specialties to pay close attention to thyroidology. At the same time, throughout the world there is a high prevalence of cardiovascular diseases, and primarily coronary heart disease (CHD). Thus, at present, in patients, especially in older age groups, combined thyroid and cardiac pathology is often encountered, which sometimes complicates diagnosis and often causes inadequate treatment.
Hypothyroidism is a clinical syndrome resulting from a deficiency of thyroid hormones in the organs and tissues of the body. Hypothyroidism, which is a fairly common pathology, occurs: among the adult population - in 1.5-2% of women and in 0.2% of men; among people over 60 years old - in 6% of women and 2.5% of men [2]. Thyroid hormone deficiency is based on structural or functional changes in the thyroid gland itself (primary hypothyroidism) or a violation of the stimulating effects of pituitary thyroid-stimulating hormone (TSH) or hypothalamic thyrotropin-releasing hormone (TRH) (central or secondary hypothyroidism) (Table 1).
The clinical picture of hypothyroidism is variable and depends on the severity of the disease.
The mildest and most common form of hypothyroidism is subclinical hypothyroidism (occurs in 10-20% of cases), in which clinical symptoms of hypothyroidism may be absent and an elevated blood TSH level is detected with normal thyroid hormone levels.
Manifest hypothyroidism is accompanied by clinical manifestations, increased TSH levels and decreased levels of thyroid hormones.
Severe long-term hypothyroidism can lead to the development of hypothyroid (myxedematous) coma.
The first clinical description of cardiovascular complications of hypothyroidism dates back to 1918, when the German physician N. Zondak first coined the term “myxedematous heart syndrome,” highlighting its main symptoms: bradycardia and cardiomegaly. 20 years later, he also described ECG changes characteristic of hypothyroidism: smoothness of the P and T waves.
Thyroid hormones both directly and indirectly affect the state of the cardiovascular system. Clinical and laboratory changes in the cardiovascular system in hypothyroidism are based on a weakening of the inotropic and chronotropic functions of the myocardium, a decrease in minute and systolic blood volumes, the amount of circulating blood and blood flow velocity, as well as an increase in total peripheral vascular resistance (Polikar).
However, the clinical picture of the disease in patients with hypothyroidism without initial damage to cardiovascular pathology and in patients with cardiosclerosis differs, which significantly complicates the timely diagnosis of hypothyroidism in patients with coronary artery disease (Table 2).
| Table 2. Main differential diagnostic symptoms of myocardial dystrophy in hypothyroidism and coronary artery disease |
As can be seen from table. 2, patients with hypothyroidism without concomitant coronary heart disease are characterized by pain in the heart region of the cardialgia type. They occur in approximately 35% of patients with hypothyroidism and are stabbing, aching, and long-lasting. For patients with hypothyroidism against the background of coronary artery disease, short-term compressive pain behind the sternum, similar to angina pectoris, is more typical. However, it should be noted that with a decrease in thyroid function, the number of ischemic attacks may decrease, which is associated with a decrease in myocardial oxygen demand.
Of the heart rhythm disturbances, bradycardia is the most typical for hypothyroidism: it occurs in 30-60% of patients. However, hypothyroidism developed against the background of ischemic heart disease and cardiosclerosis can be accompanied by tachycardia (10% of patients), supraventricular or ventricular extrasystole (24% of patients) and even atrial fibrillation. Such heart rhythm disturbances, atypical for hypothyroidism, are the reason for untimely diagnosis of this condition.
Swelling due to hypothyroidism and coronary artery disease can be localized both on the face and legs, and on the ankles and feet. Dyspnea is also more common in patients with concomitant pathology.
With hypothyroidism, the lipid spectrum of the blood changes: hypercholesterolemia appears, LDL increases, HDL decreases and hypertriglyceridemia is observed. Dyslipidemia, along with increased blood pressure, is a risk factor for the development of coronary artery disease. However, hypothyroidism will become an indirect risk factor for the development of coronary artery disease only in older people, and in patients with coronary sclerosis, uncompensated hypothyroidism aggravates the course of the disease.
If untreated, long-term hypothyroidism can be the cause of pericardial effusion, which can be detected by ECHO-CG, X-ray and ECG studies.
When diagnosing hypothyroidism in patients with coronary artery disease, a legitimate question arises about compensation of thyroid function. In most cases, patients with hypothyroidism require lifelong thyroid hormone replacement therapy. However, one should always remember that the rapid restoration of euthyroidism is accompanied by increased anabolism, an increase in myocardial oxygen demand, and the longer the patient suffers from uncompensated hypothyroidism, the higher the sensitivity of the myocardium to thyroid drugs. This is especially true for elderly patients. When carrying out replacement therapy for hypothyroidism in patients with coronary artery disease, the following cardiovascular complications are possible:
- exacerbation of myocardial ischemia: increased frequency of angina attacks, transition of stable angina to unstable;
- myocardial infarction;
- severe rhythm disturbances;
- sudden death.
However, a possible exacerbation of myocardial ischemia cannot be a reason for refusing thyroid hormone replacement therapy.
Taking into account the above, our task is optimal correction of hypothyroidism against the background of constant adequate cardiac therapy.
When treating patients with hypothyroidism and cardiac pathology, great care should be taken. In patients over 50 years of age with hypothyroidism who have never previously undergone cardiac testing, it is necessary to exclude CAD or a risk factor for CAD. The drug of choice for the treatment of hypothyroidism in patients with coronary artery disease is thyroxine. The initial dose of this drug should not exceed 12.5-25 mcg per day, and the dose of thyroxine should be increased by 12.5-25 mcg per day at intervals of 4-6 weeks (provided that the dose is well tolerated and there are no negative ECG dynamics) . If clinical and electrocardiographic signs of worsening coronary circulation appear, you should return to the original dose of thyroxine and lengthen the adaptation period, as well as adjust cardiac therapy.
On average, to compensate for hypothyroidism in patients without cardiovascular pathology, it is necessary to prescribe thyroxine at a dose of 1.6 mcg per 1 kg of body weight per day, however, for patients with coronary artery disease, the clinically optimal dose of thyroxine may not be the one that completely restores normal T4 levels and TSH in the serum, but one that alleviates the symptoms of hypothyroidism without worsening the condition of the heart.
Treatment with thyroxine in patients with hypothyroidism and ischemic heart disease should always be carried out against the background of adequately selected cardiac therapy: it is preferable to combine thyroxine therapy with combined treatment of ischemic heart disease with selective beta-blockers, long-acting calcium antagonists and cytoprotectors, and, if necessary, diuretics and nitrates.
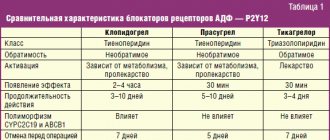
The combination of thyroxine and β-blockers (or long-acting calcium antagonists) reduces the reactivity of the cardiovascular system to thyroid therapy and shortens the time of adaptation of patients to thyroxine [3]. Currently, the “gold standard” in the treatment of coronary artery disease is therapy with preductal [4], which can effectively and reliably reduce the number and duration of attacks of myocardial ischemia, including during treatment with thyroid drugs.
When treating with cardiac glycosides (if atrial fibrillation and heart failure are present), it should be remembered that thyroid hormones increase the sensitivity of the heart muscle to glycosides and, accordingly, the risk of overdose of cardiac glycosides. Therefore, such combined treatment should be carried out under weekly ECG monitoring.
Perhaps adequate replacement therapy for patients with hypothyroidism and coronary heart disease should be selected only in a multidisciplinary hospital (endocrinology, cardiology and cardiac intensive care units are required), especially in severe forms of coronary heart disease (unstable angina, severe functional classes of stable angina, recent myocardial infarction, atrial fibrillation, extrasystole of high gradations, NC more than 2 fc).
Against the background of already selected replacement therapy for hypothyroidism, constant monitoring by an endocrinologist and cardiologist is necessary with dynamic monitoring of not only the TSH level, but also the state of the cardiovascular system (ECG, ECHO-CG, Holter ECG monitoring) once every 2-3 months.
However, for a certain category of patients with hypothyroidism and coronary artery disease, it is impossible to select adequate replacement therapy even if the above rules are observed, because treatment with thyroxine, even in small doses, sharply worsens myocardial ischemia. The reason for this may be severe stenosis of the coronary arteries. Therefore, in such cases, the patient needs to undergo selective coronary angiography, and if the diagnosis is confirmed, coronary artery bypass grafting is indicated. Hypothyroidism cannot serve as a contraindication to surgical treatment and will not cause possible complications or death as a result of surgery [6]. After successful surgical treatment, patients are prescribed thyroxine along with cardiac therapy.
With adequate replacement therapy for hypothyroidism, the following are achieved:
- persistent elimination of clinical manifestations of hypothyroidism;
- improvement of myocardial contractility;
- increased heart rate;
- normalization of cholesterol levels;
- resorption of effusion in the pericardium;
- restoration of repolarization processes on the ECG.
Hypothyroidism left untreated for a long time can be complicated by the development of hypothyroid coma, which poses a real threat to the patient’s life. In elderly patients with undiagnosed hypothyroidism, hypothyroid coma develops spontaneously. The difficulty of diagnosing hypothyroidism in old age is due to the fact that the initial clinical manifestations of hypothyroidism are taken for age-related changes and disorders of the cardiovascular system, and manifestations of a coma are taken for vascular complications.
Clinical manifestations of hypothyroid coma include hypothermia, hypoventilation, respiratory acidosis, hyponatremia, hypotension, convulsive readiness, hypoglycemia. Of these, the most consistent symptom is hypothermia, and the decrease in body temperature can be significant, sometimes up to 23 degrees.
If a hypothyroid coma is suspected, the patient should be hospitalized in the intensive care unit and immediately begin therapy with thyroid drugs and glucocorticoids. And in this case, for patients with cardiovascular pathology, the drug of choice will be thyroxine, which is prescribed intravenously or, in the absence of injectable forms of the drug, through a gastric tube in the form of crushed tablets at a dose of 250 mcg every 6 hours (the first day), in subsequent days - according to 50-100 mcg.
Administration of glucocorticoids should be carried out in parallel. Hydrocortisone is administered 100 mg IV once and then 50 mg IV every 6 hours.
Oxygenation or transfer of the patient to artificial ventilation, fluid restriction to 1 liter per day and, in case of hypoglycemia, intravenous administration of a 40% glucose solution are recommended.
In order to correct blood pressure when hypotension develops, norepinephrine should not be used, which in combination with thyroid drugs can worsen coronary insufficiency.
With correct and timely therapy, improvement in the patient's condition is possible by the end of the first day. However, mortality in hypothyroid coma in elderly patients with cardiovascular pathology can reach 80% [1]. Therefore, for patients with hypothyroidism, especially when it comes to older age categories, timely diagnosis and adequate replacement therapy are vital.
Thus, the treatment of hypothyroidism in patients with coronary artery disease is a very serious, responsible and complex task that endocrinologists and cardiologists need to solve together, relying not only on their own experience, but also on modern research. Only in this case it is possible to achieve compensation for hypothyroidism and avoid all sorts of complications that arise as a consequence of the disease itself, as well as during its replacement therapy.
Literature
1. Vetshev P. S., Melnichenko G. A., Kuznetsov N. S. et al. Diseases of the thyroid gland / Ed. I. I. Dedova. M.: JSC "Medical Newspaper", 1996. P. 126-128. 2. Gerasimov G. A., Petunina N. A. Diseases of the thyroid gland. M.: Publishing house of the magazine “Health”, 1998. P. 38. 3. Kotova G. A. Hypothyroidism syndrome. Diseases of the endocrine system / Ed. I. I. Dedova. M.: Medicine, 2000. P. 277-290. 4. Lallotte A. Trimetazidine: a new approach to the treatment of patients with severe forms of coronary artery disease // Heart and Metabolism. 1999. No. 2. P. 10-13. 5. Polikar R., Burger A., Scherrer U. et al. The thyroid and the heart // Circulation. 1993. Vol. 87. No. 5. P. 1435-1441. 6. Wienberg AD, Brennan MD, Gorman CA Outcome of anesthesia and surgery in hypothyroid patients // Arch. Intern Med. 1983. Vol. 143. P. 893-897.
Note!
- Currently, patients, especially in older age groups, often have combined thyroid and cardiac pathology, which sometimes complicates diagnosis and often causes inadequate approaches to treatment.
- The first clinical description of cardiovascular complications of hypothyroidism dates back to 1918, when the German physician N. Zondak first coined the term “myxedematous heart syndrome,” highlighting its main symptoms: bradycardia and cardiomegaly, and 20 years later he described ECG changes characteristic of hypothyroidism: smoothness P and T waves.
- For patients with hypothyroidism against the background of coronary artery disease, short-term compressive pain behind the sternum similar to angina pectoris is more typical, however, it should be noted that with a decrease in thyroid function, a decrease in the number of ischemic attacks may occur, which is associated with a decrease in myocardial oxygen demand.
- The drug of choice for the treatment of hypothyroidism in patients with coronary artery disease is thyroxine. The initial dose of thyroxine should not exceed 12.5-25 mcg per day and an increase in the dose of thyroxine by 12.5-25 mcg per day should occur at intervals of 4-6 weeks, provided that the dose is well tolerated and there are no negative ECG dynamics.
- Adequate replacement therapy for patients with hypothyroidism and coronary artery disease should be selected only in a multidisciplinary hospital.
Symptoms of the disease
A decrease in the activity of the thyroid gland leads to a slowdown in metabolism. and the appearance of the following symptoms:
- general weakness;
- apathy;
- decreased blood pressure;
- decreased heart rate (bradycardia);
- sexual dysfunction (infertility, impotence, problems with the menstrual cycle, decreased libido);
- violation in the intellectual sphere.
With hypothyroidism, mood swings, increased anxiety, sleep problems, uncorrectable weight gain, hair loss, poor tolerance of high and low temperatures, constipation, and frequent colds due to reduced immunity are often observed.
Often a person complains of a feeling of a lump in the throat and difficulty breathing. Swelling, poor appetite, nausea, stiffness in movements, depression, deterioration of hearing and vision may be a concern.
Read also
Symptomatic arterial hypertension
Arterial hypertension is a very common disease of the human cardiovascular system.
According to statistics, 20-30% of the population suffers from arterial hypertension, aged 60 years and above... Read more
Metabolic syndrome
Metabolic syndrome is a “pandemic of the 21st century.” The prevalence of metabolic syndrome is 20–40%. In the Russian Federation, 40% of the population have 2 components of metabolic syndrome, 11% –...
More details
Osteoporosis
Osteoporosis is a progressive metabolic disease of the skeletal bones, which results in a decrease in bone density and disruption of its internal structure. The result of osteoporosis is...
More details
Diabetes mellitus, type 2
Diabetes mellitus (DM) is a group of metabolic diseases characterized by chronic hyperglycemia, which results from impaired insulin secretion, insulin action, or both...
More details
Hyperprolactinemia
Hyperprolactinemia is a persistent increase in the level of the hormone prolactin in the blood. Hyperprolactinemia syndrome is a complex of symptoms that occur against the background of increased prolactin levels, the most characteristic...
More details
Diagnosis of pathology
After a visual examination and clarification of family history, the specialist prescribes the following types of laboratory and instrumental studies:
- clinical and biochemical blood test;
- blood test for thyroid hormones (TSH, T4, T3 and antibodies to thyroid peroxidase (AT TPO, AT TG);
- ultrasonography;
- x-ray of the thyroid gland (in rare cases);
- CT scan;
- Magnetic resonance imaging.
Scintigraphy and/or thyroid biopsy can be used as an auxiliary diagnosis.
Prevalence of hypothyroidism
Hypothyroidism is a very common disease. Scientific evidence suggests that the prevalence of hypothyroidism is higher in northern regions than in southern regions. The average incidence of hypothyroidism is 19 per 1000 women. Among men, hypothyroidism is rare - in 1 case per 1000. With age, hypothyroidism begins to occur even more often - in some regions, hypothyroidism can be detected in 2-3% of women aged 50 years and older.
The number of patients with hypothyroidism is so large that sometimes up to 50% of patients present with hypothyroidism-related complaints when visiting an endocrinologist.