Symptoms of cerebral atherosclerosis
If a patient has cerebral vessels affected by atherosclerosis, symptoms and treatment can be quite varied. However, there are a number of manifestations of this disease that are common to most cases.
- The initial stage of the disease is characterized by negative changes in the psyche. The patient becomes irritable, often experiences neuroses, depressive moods, gets tired quickly, and feels inhibited. Unreasonable headaches occur, the head sometimes becomes heavy, and sometimes a pressing feeling appears. And the main symptom is memory impairment: first, the patient has difficulty remembering new information, and then cannot remember past events.
- Then atherosclerosis of the cerebral vessels manifests itself in the form of more serious mental disorders. Patients are constantly concerned about their own state of health and suspect various pathologies. Delusions of persecution often occur, and sensitivity to external factors (stress) increases. New physiological symptoms appear: tingling, burning in different parts of the body.
- In an advanced state, the patient practically loses the ability to care for himself, and dementia develops. The patient does not remember new information, although he can still remember past events. He is disoriented in time and space, and therefore requires constant supervision. Transient ischemic attacks occur with disorders of speech, vision, and sensitivity. Circulatory disorders in the brain lead to spasms and strokes.
Senile sclerosis
Syphilis
Encephalitis
Stroke
Diabetes
3124 04 October
IMPORTANT!
The information in this section cannot be used for self-diagnosis and self-treatment.
In case of pain or other exacerbation of the disease, diagnostic tests should be prescribed only by the attending physician. To make a diagnosis and properly prescribe treatment, you should contact your doctor. Senile sclerosis: causes, symptoms, diagnosis and treatment methods.
Definition _
Senile sclerosis is called memory impairment in older people. In fact, there is no such disease officially, and “senile sclerosis” means late-life dementia, or senile dementia - acquired dementia, which is characterized by a persistent decline in cognitive activity, complete or partial loss of knowledge and practical skills, the inability to acquire new ones, and the collapse of mental functions .
This condition can manifest itself as disturbances in memory, abstract thinking, judgment, speech, the ability to perform purposeful actions, and recognize objects.
Causes of senile sclerosis
The expression “senile sclerosis” may owe its name to cerebral atherosclerosis (atherosclerosis of the blood vessels of the brain) as the earliest known cause of dementia in the elderly.
The term "sclerosis" means the replacement of normal connective tissue.
In English there is no phrase similar to our “senile sclerosis”, but the expressions Alzheimer's disease (Alzheimer's disease) or senile dementia (senile dementia) are used.
Currently, a large number of possible causes of dementia are known:
- metabolic (endocrinopathies, Wilson's disease);
- traumatic (subdural hematoma, hydrocephalus);
- tumor;
- infectious (brain abscess, tertiary cerebral syphilis, hydrocephalus, meningitis and encephalitis);
- vascular (cerebral infarction, multiple repeated cerebrovascular accidents);
- degenerative (Alzheimer's disease, Pick's disease);
- congenital (Huntington's disease), etc.
All these pathological conditions share common features:
- endogenous nature of the disease;
- slow onset and progressive course - from mild dementia to total dementia;
- presence of neurological disorders;
- familial nature of the disease;
- hallucinations, delusions.
Alzheimer's disease (AD) is a common form of primary degenerative dementia of late age, characterized by a subtle onset, steady progression of memory impairment and mental function until the total collapse of intelligence and mental activity.
Early-onset AD (presenile dementia of the Alzheimer's type) develops mainly before the age of 65 and leads to total dementia with severe speech disorders and impaired ability to perform sequential sets of conscious actions. The leading factor in the occurrence of early-onset asthma is genetic burden (10% of the total number of patients with asthma). Mutations in the genes encoding the proteins presenilin-1, presenilin-2 and amyloid precursor protein are associated with the risk of developing Alzheimer's disease in almost 100% of cases.
In AD with late onset at 65-85 years of age (senile dementia of the Alzheimer's type), the most complex forms of intellectual activity associated with abstract thinking and criticality are affected.
Risk factors for developing asthma:
- modifiable
(low level of education and low intellectual activity, physical inactivity, smoking, uncontrolled arterial hypertension in middle and old age, hyperlipidemia, hyperhomocysteinemia, diabetes mellitus, obesity, depression); - non-modifiable
(elderly and senile age, family history of asthma, carriage of genetic polymorphisms, presence of the APOE4 allele, female gender, history of traumatic brain injury).
In Alzheimer's disease, there are disturbances in the metabolism of amyloid precursor protein.
Normally, this protein is broken down into polypeptides that are not pathogenic (that is, not capable of causing disease). In AD, aggregation (sticking together) of its insoluble fragments occurs into a pathological protein β-amyloid, which has neurotoxic properties. Deposition of this protein in the brain parenchyma and in the walls of blood vessels (with the formation of senile plaques) leads to damage and death of neurons. Senile dementia can be of vascular origin and develops:
- as a result of a single heart attack or hemorrhagic stroke, which is localized in a strategically important area of the brain for cognitive and mental activity;
- as a result of repeated episodes of acute cerebrovascular accident of the ischemic type of cortical-subcortical localization;
- as a result of damage to the terminal small-caliber vessels supplying blood to the subcortical basal ganglia and deep parts of the white matter of the brain;
- as a result of disturbances in systemic hemodynamics with a sharp decrease in cerebral circulation (acute heart failure, a decrease in circulating blood volume, a pronounced and prolonged decrease in blood pressure).
As a result of vascular events in the brain, post-ischemic or post-hemorrhagic cysts, changes in white matter, death of nerve cells, and linear deposits of iron-containing pigment formed during the breakdown of blood occur.
Risk factors for developing dementia of vascular origin may include:
- arterial hypertension, coronary heart disease, heart rhythm disturbances;
- high cholesterol, atherosclerosis;
- diabetes;
- smoking;
- obesity;
- high levels of homocysteine;
- rheumatic diseases, vasculitis;
- blood clotting disorders;
- amyloid angiopathy;
- congenital vascular anomalies, etc.
Classification of the disease
Due to the cause of occurrence, senile dementia can be:
- vascular,
- atrophic (Alzheimer's type syndrome, dementia with Lewy bodies, dementia caused by chorea, Huntington's dementia),
- mixed.
By localization:
- cortical - with predominant damage to the cerebral cortex (Alzheimer's disease, frontotemporal lobar degeneration, alcoholic encephalopathy);
- subcortical - with predominant damage to subcortical structures (progressive supranuclear palsy, Huntington's disease, Parkinson's disease, multi-infarct dementia);
- cortical-subcortical (Lewy body disease, corticobasal degeneration, vascular dementia);
- multifocal - with multiple focal lesions (Creutzfeldt-Jakob disease).
There are mild, moderate and severe degrees of dementia.
Symptoms of senile sclerosis
Mild degree
: professional activity and social activity are possible, but limited, the circle of communication and interests is narrowed; independence in everyday life is maintained, but reminders, assistance in mastering new information and solving financial issues, and psychopathic sharpening of personality traits may be required.
Moderate degree
: decreased ability to use household appliances, problems with hygiene, dressing, cooking, movement, daily activities, difficulties in living independently. However, the patient can still be left alone for some time.
Severe degree
: the patient needs help in almost all activities and outside care.
With subcortical localization of the process, the earliest symptom is memory impairment. Patients demonstrate slowness, rigidity of mental processes, difficulties in switching from one type of activity to another, errors in planning activities and performing sequential actions.
Frontotemporal dementia is characterized by changes in personality and behavior. Within a short period of time, a person completely loses the ability to cope with his affairs and exist independently.
In patients with cortical-subcortical dementia, symptoms of cortical and subcortical lesions predominate.
Multifocal dementias are characterized by the presence of multiple disorders: speech, recognition, memory, spatial perception, purposeful movements and actions. There are also subcortical disorders:
- sustained repetition of any phrase, activity, emotion, sensation (perseveration);
- sudden, short, jerky movements of the muscles of the limbs, face, torso, not accompanied by loss of consciousness (myoclonus);
- pyramidal (paralysis, paresis, pathological reflexes) and extrapyramidal disorders (muscle tone disorders).
These disorders are combined with cerebellar pathology (disturbances in gait and coordination of movements).
There is increasing drowsiness. In Alzheimer's disease, first there is a decrease in memory for current events: insignificant details, new names, and the contents of recently read books are forgotten. Criticism of one's condition is preserved. The average duration of this stage in older people is about 5 years. Subsequently, the disease progresses, difficulties appear in everyday life: memorization of new material is impaired, while the storage of memorized information does not suffer, difficulty in orienting in unfamiliar terrain and time arises, speech disorders appear, and personal characterological characteristics become sharpened.
Personal changes are characterized by suspicion and conflict, delusional ideas directed against the immediate environment. Patients suspect relatives of stealing their things, planning to leave them without help, and putting them in a nursing home. In later stages of the disease, aggressiveness, inappropriate sexual behavior, untidiness, hallucinations, and decreased criticism of one’s condition are noted.
The clinical picture of senile dementia of vascular origin is determined by the volume and localization of changes in the brain.
The course of the disease can begin acutely with partial improvement and gradual deterioration. The following symptoms are observed: confusion, severe apathy, restriction of daily activity up to failure to comply with personal hygiene rules, severe memory impairment for current events, impaired perception of spatial relationships, difficulties with counting, understanding logical and grammatical speech structures. Patients cannot properly organize their activities, often abandon the work they started, get tired quickly, are unable to analyze information, work with several sources of information at once, or quickly move from one task to another. Emotional disorders appear in the form of a decrease in mood, the development of depression or anger.
Movement disorders and gait disturbances may be observed. Slowness and staggering appear, the patient cannot take the first step, marks time, the legs do not leave the floor, but slide along it (“skier’s gait”), balance suffers, the risk of falling increases at the beginning of walking, when turning and when stopping. The advanced stage of the disease is characterized by frequent urination and periodic urinary incontinence. Subsequently, a complete loss of control over the function of the pelvic organs develops.
The basis of the clinical picture of mixed dementia is a combination of focal neurological symptoms and mental disorders: disturbances in walking, speech, swallowing, urination, attention and memory. Patients with mixed dementia have more pronounced visual-spatial impairments, decreased attention, and the sleep-wake cycle is disrupted.
Thus, dementia syndrome is characterized by a deep impoverishment of intelligence, the use of past experience becomes impossible. Criticism towards one's condition and surroundings suffers greatly. The individual's adaptation to society is disrupted.
Diagnosis of senile sclerosis
The diagnosis of senile dementia is established on the basis of:
- complaints and information received from the patient and the patient’s environment (relatives, friends, acquaintances);
- data on the impact of existing disorders on the patient’s daily (basic and instrumental) activities;
- available drug therapy (drugs with anticholinergic properties, antipsychotics, barbiturates, benzodiazepine derivatives, antihistamines, some beta-blockers, HMG-CoA reductase inhibitors (statins) with lipophilic properties, cardiac glycosides and other drugs);
- patient examination data in order to detect concomitant diseases that can lead to the formation or aggravation of the severity of mental and cognitive disorders (hypothyroidism, diabetes mellitus, deficiency of vitamin B12, folic acid, neuroinfection (syphilis, HIV, etc.), cancer, renal, liver failure and etc.);
- certain data from laboratory and instrumental examination methods to clarify the diagnosis:
•
biochemical blood test, including:
- total protein, albumin, protein fractions;
Causes and risk factors
Pathology occurs due to metabolic disorders and cholesterol circulation. It accumulates in the body and is deposited on the walls of blood vessels in the form of plaques consisting of fibrin and other substances.
Main risk factors:
- excessive drinking and smoking;
- hyperlipidemia (high cholesterol);
- arterial hypertension and other vascular diseases;
- obesity and diabetes;
- constant stress;
- sedentary lifestyle;
- hormonal imbalances.
A person may also be genetically predisposed to this disease (close relatives have had strokes or heart attacks). In addition, there is an age-related risk factor: men over 45 and women over 55 are susceptible to atherosclerosis to the maximum extent.
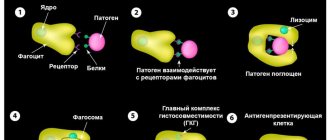
Pathogenesis of MS
The pathogenetic mechanism of development of neurological pathology consists of several successive stages. Under the influence of a combination of triggers, autoimmune processes are launched that provoke the activity of T-lymphocytes (immune blood cells) and the synthesis of auto-aggressive antibodies to the myelin protein. Autoreactive T lymphocytes cross the blood-brain barrier (BBB) and penetrate nerve fibers. Next, there is an uncontrolled release of specific pro-inflammatory cytokines, which disrupts the exchange of information and coordination of actions between cells. Active inflammation develops, destroying the myelin sheaths. A sclerotic plaque forms. The process of progressive death of nerve cells—neurodegeneration—begins.
The compensatory mechanism of the myelin sheaths is poorly developed, so remyelination (recovery) does not keep up with the rate of demyelination.
Diagnostics
Treatment of cerebral vessels should be preceded by a high-quality diagnosis, during which the doctor will determine the localization of plaques, the degree of their development, and assess the condition of the organs.
When undergoing diagnostics, it is important to follow a comprehensive principle, since the disease has many manifestations and complications. Therefore, do not be surprised if you are also asked to visit an ophthalmologist, cardiologist, neurologist, or vascular surgeon. Try to tell the doctors in as much detail as possible about the anomalies you notice in the body’s functioning.
The most effective and modern methods are:
- various types of electrocardiography with stress tests;
- Ultrasound of cerebral vessels;
- duplex and triplex scanning with ultrasound examination of blood vessels;
- magnetic resonance imaging (allows you to visually assess the condition of blood vessels and examine atherosclerotic plaques);
- angiography, coronary angiography - minimally invasive examinations, during which the doctor evaluates general atherosclerotic lesions.
The patient also undergoes a series of laboratory tests, the purpose of which is to identify metabolic disorders, hormonal imbalances and other causes of the development of pathology.
Causes of multiple sclerosis
The underlying cause of multiple sclerosis (MS) has not been definitively identified. In neurology, the theory of multifactorial occurrence of the disease is accepted, where the leading role is given to immunopathological reactions. Additional causes of damage to the brain and spinal cord are:
- Genetic predisposition. Recent research from the Canadian University of British Columbia proves the inheritance of the damaged NR1H3 gene.
- Viral infections. The main pathogens are herpes virus types 1 and 4, measles paramyxovirus, and rubella virus.
- Nicotine addiction. In a comparative analysis, the ratio of smoking and non-smoking patients with MS was 2:1.
- Psychogeny of psychotic level in the anamnesis.
- Climatic conditions. Countries with a temperate climate are considered a risk zone. The geographical factor has no scientific basis.
Shpidonov Gennady Stanislavovich
Neurologist
Rostov State Medical University (neurology)
10 years of experience
Thus, multiple sclerosis is the result of the combinatorial action of aggressive autoimmune processes, heredity and negative external influences on the body.
Treatment of cerebral atherosclerosis
If the patient has an early stage of cerebral vasoconstriction, treatment consists of drug therapy and lifestyle changes (diet, giving up alcohol, smoking, increasing physical activity). The goal is to reduce cholesterol levels to normal.
Drug therapy in the treatment of cerebral vascular spasms is aimed at strengthening the walls of blood vessels and stabilizing the atherosclerotic plaque. As a result, the development of atherosclerosis is inhibited, and lipid metabolism in the body is normalized. To prevent complications, statins, fibrates, and antiplatelet agents are used.
Among the surgical treatment methods, stenting and bypass surgery are common. In particular, stroke is prevented by stenting the carotid arteries.
- Operations to remove the plaque are carried out in an open manner (endarterectomy): access to the damaged vessel is organized, it is dissected, the plaque is removed, then a vascular suture is applied, and the tissue is sutured.
- The closed method involves the use of an endoscope and a stent. The operation is performed through a small (1-3 cm) incision, through which access to a large vessel is provided. A special catheter is brought through the circulatory system to the site of narrowing of the vessel, and then an artificial stent is inserted through the catheter, expanding the lumen of the vessel and strengthening its walls.
Symptoms of Multiple Sclerosis
The disease is not distinguished by pathognomonic (specific) signs. The early clinical picture is characteristic of a number of neurological diseases. Typical manifestations include:
- fatigue, dizziness;
- weakness of skeletal muscles;
- muscle twitching - fasciculations;
- numbness of the limbs, a feeling of “crawling goosebumps” throughout the body - paresthesia;
- loss of coordination and balance, unsteadiness of gait;
- signs of neuritis of the optic, oculomotor, abducens, trigeminal, facial nerve;
- decreased clarity of vision (most often, diplopia).
As the disease progresses, the neurological picture intensifies, which is explained by damage to the cranial nerves, the cerebellum and its connections. Patients experience symptoms such as:
- tremor turning into hyperkinesis;
- change (enlargement) of handwriting;
- dysarthria in the form of scanned (“ragged”) speech;
- neuropsychic weakness - asthenia;
- oscillatory movements of the eyeballs - nystagmus;
- wave-like twitching of the facial muscles - myokymia;
- neuropathic and muscle pain;
- decreased plantar extensor reflex;
- disruption of the intestines and bladder - urinary retention, constipation;
- cognitive disorders - decreased memory, attention, problems with thinking and processing information;
- depressive syndrome;
- anorgasmia in women, erectile dysfunction in men.
The severity of symptoms depends on the stage of the pathological process affecting the brain and spinal cord.
Prevention of cerebral atherosclerosis
- Daily physical exercise will help keep your blood vessels toned: physical activity that is appropriate for your age should be at least 40 minutes a day.
- To normalize cholesterol levels, watch your diet, weight, follow a special diet, and give up bad habits.
- Walk more in the fresh air to saturate your blood with oxygen.
- Limit emotional stress - protect yourself from stress.
- Monitor your blood pressure and glucose levels.
2. Reasons
To date, the etiopathogenetic mechanism of atherosclerosis continues to be the subject of intensive study and discussion. About ten main hypotheses are considered (viral, hereditary, chlamydia, autoimmune, etc.), each of which has the right to exist and finds well-reasoned confirmation. Perhaps atherosclerosis refers to the so-called. polyetiological, or multi-cause processes, or against the background of these conditions, is triggered by some common, not yet known trigger factor. However, risk factors have been quite reliably established that significantly increase this likelihood:
- - smoking and drinking alcohol;
- — physical inactivity combined with overeating and obesity;
- - arterial hypertension;
- - situations of chronic distress;
- - age-related hormonal changes;
- - diabetes;
- — certain metabolic disorders (metabolism), especially in relation to fats and proteins;
- - “viscosity” of blood (increased coagulability).
Visit our Cardiology page
Vascular atherosclerosis: treatment and diagnosis at CBCP
At an early stage of the disease, it is extremely important to undergo a high-quality diagnosis and begin treatment, during which negative consequences can be minimized. If you notice alarming symptoms, contact the Center for Circulatory Pathology, where you will be offered modern diagnostics and effective treatment methods.
CBCP provides a wide range of methods that provide objective and detailed information about the patient’s condition: location of pathology, complexity, possible complications.
Course of MS
Characteristic variants of the clinical course of multiple sclerosis:
- Remitting. Exacerbations are replaced by latent periods with partial restoration of lost functions.
- Secondary progressive. An undulating course of chronic progressive destruction of nerve fibers, with increasing neurological deficit;
- Primary progressive. Progressive increase in demyelination and neurodegeneration, accompanied by an increase in the intensity of symptoms.
A benign course of MS is considered to be the patient’s ability to maintain functionality for at least 15 years from the onset of the disease. The malignant course is characterized by an accelerated change in the patient's condition, rapid disability and mortality.
Shpidonov Gennady Stanislavovich
Neurologist
Rostov State Medical University (neurology)
10 years of experience