About CABG surgery
Coronary artery bypass grafting (CABG) is one of the most effective methods in the treatment of coronary heart disease (CHD).
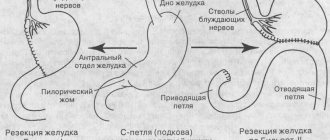
The operation is performed on a beating heart, without the use of artificial circulation, and is indicated in cases where damage to the arteries of the heart is so severe that the use of other methods of restoring coronary blood flow is impossible. In our clinic of the Federal Scientific and Clinical Center of Federal Medical and Biological Agency, coronary bypass surgery is performed using several methods:
- on a “working” heart without the use of artificial circulation;
- on a beating heart under conditions of assisted artificial circulation.
Indications for coronary artery bypass grafting
Indications for CABG are determined by varying degrees of arterial damage and manifestations of coronary heart disease:
As a rule, CABG is not performed:
- severe multiple organ failure;
- during the first months after cerebrovascular accident;
- malignant neoplasms.
Essence, indications and contraindications
Attention! Only your attending physician will give you health recommendations that are relevant to you. The article contains only general information that will help you navigate the problem.
As a rule, the operation is performed when the patient’s coronary bed is affected by 75% or more, and angina pectoris is resistant to medications.
During the operation, an additional path is created for blood flow to the heart, bypassing the arteries affected by atherosclerosis. The donor of shunts, vascular grafts, is the patient himself - they are taken from the internal mammary artery, the great saphenous vein in the leg or the radial artery in the arm. The duration of the operation depends on the number of affected arteries - on average, 4-5 hours.
Also, before surgery, it is necessary to take into account such risk factors as:
- diffuse lesions of all coronary arteries
- heart failure and kidney failure
- scarring and decreased performance of the left ventricle by more than 30%
- oncological diseases
- chronic nonspecific lung diseases: bronchitis, pneumonia, asthma, emphysema
Preparation for coronary artery bypass surgery
At the Federal Scientific and Clinical Center of the Federal Medical and Biological Agency, before performing coronary artery bypass surgery, the doctor draws up a preoperative examination plan. It includes laboratory tests and instrumental studies:
- general blood test, urine test;
- blood biochemistry;
- expanded coagulogram;
- ADP platelet aggregation;
- blood type and Rh factor;
- markers of infections: HIV, hepatitis B, hepatitis C, syphilis;
- Pro-BNP, SRP;
- ECG;
- Echo-CG;
- X-ray examination;
- EGDS (maximum duration – 1 month). An exception is patients with lesions of the left artery trunk;
- Ultrasound scanning of the brachiocephalic arteries (maximum duration – 3 months);
- Ultrasound scanning of the arteries of the lower extremities (maximum duration – 3 months);
- Ultrasound scanning of the veins of the lower extremities (maximum duration – 7 days);
- FVD (maximum duration – 7 days);
- Ultrasound of internal organs;
- coronary angiography.
If there is a concomitant pathology, additional tests may be prescribed:
- History of stroke - CT scan of the brain.
- thyroid diseases - TSH, T4, T3 (maximum duration - 30 days). Consult an endocrinologist if there are changes in the hormonal profile.
- diabetes mellitus - glycemic curve (maximum duration - 7 days). Consultation with an endocrinologist for glycemia more than 10 mmol/l.
- Gout - uric acid (maximum duration - 1 month). If the value exceeds 420 µmol/l, consult a therapist and select therapy.
- consultation with a dentist, urologist, gynecologist.
The day before surgery, the patient is examined by a surgeon and an anesthesiologist. On the eve of CABG, it is recommended to have a light dinner no later than 12 hours before surgery, not to eat or drink the night before, and to stop taking medications. A cleansing enema is given at night. In the morning the patient takes a shower.
After signing the informed consent, the patient is given premedication - medications are administered that will reduce emotional tension and help calm down. After 40-60 minutes, the patient is taken to the operating room.
At the cardiology center of the Federal Scientific and Clinical Center of the Federal Medical and Biological Agency, you can take all the tests and undergo studies recommended by your doctor before the operation. The structure of our center allows you to quickly go through the preparatory preoperative stage and get the results in hand. Having our own laboratory, we are responsible for the accuracy of tests and the quality of clinical and laboratory studies.
Work after valve replacement
Within a few weeks after surgery, patients usually manage to restore their ability to work at their previous level. In some cases, a transition to easier working conditions is required. Sometimes patients are given a disability group.
The above formulations are quite streamlined, but it is impossible to give specific figures here. Much depends on which valve was prosthetized, what type of artificial valve was, in connection with what disease the operation was performed, and in what field the person is employed.
In general, the forecast for work activity is favorable. Even professional athletes returned to sports after this surgical intervention and successfully continued their careers.
Carrying out CABG
Coronary artery bypass surgery on a beating heart begins with providing access to the operation site - the skin, subcutaneous layers, and muscles are cut layer by layer.
A graft (shunt) - a healthy section of a vein or artery - is taken from the patient's chest or limb (thigh, lower leg). To perform surgery on a beating heart, special equipment is used to stabilize the myocardium at the site of the anastomosis. One end of the healthy vessel is sutured to the aorta, the other to the coronary artery below the stenotic/narrowed area. Then full heart function is restored, the wound is sutured, and the patient is transferred to the intensive care unit.
Coronary bypass surgery in most clinics is performed with cardiac arrest using a heart-lung machine. The use of this method is associated with the risk of complications that prolong recovery time, worsen recovery, and can lead to bleeding, stroke, and heart attack. Carrying out surgery without artificial circulation - on a beating heart - reduces the risk of postoperative complications.
How is diastasis sutured?
There are several fundamentally different approaches to surgical correction of diastasis of the rectus abdominis muscles.
Most often, diastasis is sutured during abdominoplasty by our colleagues - plastic surgeons. Unfortunately, in the vast majority of cases they are limited to simple suturing of the white line (the so-called “plication”), sometimes with two rows of sutures.
Simple plication with “regular” absorbable suture material carries a risk of recurrence of diastasis (not to mention hernia) in 40% of cases, according to a study conducted by Van Uchelen et al [1]. Of course, such results cannot suit us.
Plastic surgery with local tissues without the use of a mesh implant is quite acceptable for small diastasis, up to 40 mm wide, and a hernia with a defect of up to 10 mm. This has been proven and recommended in the clinical guidelines of the European Hernia Society (EHS). When performing plastic surgery of the anterior abdominal wall, we use in our practice the latest generation non-absorbable suture material, “anchor” type (V-loc PBT), which, in our opinion, is much more reliable than traditionally used options, and this more than compensates for its high cost.
Good results are demonstrated by suturing the diastasis using tangential sutures, which we use in some cases.
Fig. 1. Tangential sutures during open suturing of diastasis of the rectus muscles make it possible to make the relief of the anterior abdominal wall flatter [2]
Diastasis of more than 40 mm or the presence of a hernia with a defect of more than 10 mm is an indication for the use of a mesh implant (“mesh”).
The mesh implant serves to strengthen the sutured white line and/or hernia defect. It makes no sense to simply close her diastasis, which I have observed with surprise several times among my colleagues - with this option, the protrusion of the white line after the operation occurs along with the mesh, and there is no cosmetic result of this operation.
In principle, the implant can be placed in different layers of the anterior abdominal wall:
We use all options, choosing the optimal one for each patient in a specific clinical situation. Except perhaps for option B, which has long proven its ineffectiveness.
We rarely use the location of the implant in the abdominal cavity (intra-abdominal). The fact is that polypropylene (or polyester), which the implant itself is made of, should not come into contact with the abdominal organs - it causes a massive adhesive process, leading to adhesive intestinal obstruction and other life-threatening complications. Implants for intra-abdominal plastic surgery have a special anti-adhesion coating on one side, which significantly increases the cost of the implant, but is not always able to “protect” the organs. And if recently these were isolated cases, today more and more often voices are heard among herniologist surgeons about abandoning this technique. I gave it up several years ago, after twice operating on patients (from other clinics, and even countries) with complications. Yes, this is not much, but why expose the patient to even a minimal risk of complications that can be avoided?
Rice. 2 Options for placing a mesh implant for hernia and diastasis repair: A – above the aponeurosis (onlay), B – sewing into the edge of the defect (inlay), C – in the axillary space, D – in the preperitoneal space (underlay preperitoneal), E – in the abdominal cavity (underlay intraperitoneal) [2].
The choice of the optimal layer for implant placement depends on many factors: from the presence and width of aponeurosis defects and the degree of diastasis to the body mass index and skin condition of the patient. Each option has its own advantages and disadvantages; we choose it together with the patient during consultation.
After operation
In general, rehabilitation and recovery after CABG without artificial circulation is faster and easier. If the early postoperative period passes without complications, then after a day the catheters are removed and the patient is transferred to the department, where he remains for up to 7-10 days. There the condition of the heart and the whole body will be monitored.
In the postoperative period, a rehabilitation plan is individually selected for the patient and physical therapy is prescribed.
A good method of maintaining health is walking for 10 minutes at the very beginning (after you are allowed to walk) to 30-60 minutes 2-3 weeks after surgery.
It is important that during physical activity, the heart rate does not rise above 100-115 beats per minute and there is no shortness of breath.
If, after the operation and the rehabilitation period in the ward - in the cardiac surgery department, you are worried about independent recovery, you can undergo a rehabilitation program at our center.
Upon discharge from the hospital, the attending physician will issue a reminder about the rules of prevention after surgery and prescribe medications. Taking any other medications, including those from your home medicine cabinet, should be agreed with a cardiologist.
Smoking and drinking alcohol after CABG surgery are prohibited for life. You will also need to follow a diet with a reduced content of salt, fats, and sweets.
Afterwards, you will need to undergo a heart study at 1 month, 3, 6, 12 months. You can also do this in our center.
Physical activity after valve replacement
Often, patients are sent for valve replacement if, before surgery, there were manifestations of chronic heart failure, which impair exercise tolerance and do not allow patients to move freely and actively.
The operation improves well-being, but patients often have no idea whether they can increase the load, in what specific mode to do this and to what limits. To determine the exercise regime, it is best for the patient to undergo a rehabilitation program in a sanatorium. An individual set of physical exercises will be selected for him, which he will perform under the supervision of a doctor. Gradually, taking into account the dynamics, the motor mode will expand. As a result, by the end of the rehabilitation period, a person will be able to live a full active life, freely endure everyday and other stresses.
If the patient does not plan to undergo rehabilitation in a sanatorium, he should contact a cardiologist with questions related to physical activity. You can clarify any questions with your doctor: the ability to engage in certain sports, lift weights, drive a car, etc.
In the first weeks, during the recovery period after surgery, it is very important to control the degree of stress. It is necessary to be active to such an extent that, on the one hand, it does not overload the heart, and on the other, does not slow down recovery and does not contribute to the development of complications.
Some patients move little because planning loads and performing exercises require discipline, diligence, and effort. Those who are too lazy to exercise should remember that physical activity improves the prognosis of heart disease, trains the cardiovascular system, has a general healing effect and helps to achieve better results from the operation.