Clinic experts:
- Zotov Alexander from the Federal Scientific and Clinical Center of FMBA
- Vasiliev Vladislav from the National Medical Research Center of Cardiology
- Amir Kramer from TASMC
- Dmitry Pevny from TASMC
For severe angina, atherosclerosis, and coronary heart disease, the best solution is CABG (coronary artery bypass grafting) surgery.
It is this procedure that not only saves a person’s life, but also significantly improves its quality. The Medis Clinic offers patients who have appropriate indications to undergo heart bypass surgery in Moscow or Israel with the most experienced and competent cardiac surgeons who have the most modern techniques for heart interventions, in premium hospitals. We also offer aortic or mitral valve replacement or surgery, as well as aortic root replacement. The cost of CABG and hospitalization is 300 thousand rubles, performed by a leading cardiac surgeon in the leading cardiac surgery center in the country. We approach the selection of doctors very carefully and cooperate only with conscientious, honest doctors who have extensive practical experience and have worked in various large clinics not only in Russia, but also abroad. International experience, the ability to perform the most modern procedures in high-tech and patient-safe ways, following medical protocols currently accepted in the world, as well as placing human health and well-being at the forefront - these are what we and our patients value in doctors.
Doctors who operate on patients
We “collaborate” with such luminaries as the legendary professor Renat Akchurin, that is, if you have a complex problem, we will try to get you to an academician. We also work with the world-famous cardiac surgeon Maruo del Giglio , as well as with famous Israeli cardiac surgeons Amir Kramer and Dmitry Pevny , and other highly qualified specialists in whom we have complete confidence. The medical team involved in the operation and nursing is also highly qualified and gives our patients maximum attention.
What do you get when you seek treatment from us:
Rehabilitation period
Typically, patients remain on a ventilator for some time after CABG. After restoration of independent breathing, it is necessary to combat congestion in the lungs: rubber balls (or special devices) are well suited for this, which the patient inflates 10-20 times a day, thereby ventilating and straightening the lungs.
The next task is the treatment and dressing of wounds of the sternum and legs. After 7-14 days, the skin wounds heal and the patient is allowed to shower.
During CABG surgery, the sternum is dissected, which is then secured with metal sutures, since it is a very massive bone and bears a large load. For faster healing, it is necessary to provide her with rest; for this purpose, special medical bandages are used. You can do without a corset, however, there are cases when the sutures cut through in operated patients and the sternum diverged, as a result of which repeated operations were performed, although not such large ones. Therefore, patients are recommended to purchase and use a chest bandage.
The next stage of rehabilitation is an increase in motor activity. After the operation, when angina is no longer a concern, the doctor prescribes how to increase the pace. Usually they start by walking along the corridor up to 1000 meters per day, and gradually increase the load. Over time, the motor mode is not limited. After discharge from the hospital, it is advisable to go to a sanatorium for final recovery.
2-3 months after surgery, it is recommended to conduct a VEM or Treadmill stress test in order to assess how passable the new bypass paths are and how well the myocardium is supplied with oxygen. If there is no pain or changes on the ECG during the test, then recovery is considered successful.
In case of violation or cessation of medicinal, dietary and physical measures during the recovery period, recurrence of plaques is possible, and re-operation may be refused. In some cases, new narrowings may be stented.
Cost of CABG
Yes, the price of CABG from such “gurus” of cardiac surgery is quite high, from a quarter of a million rubles, but you pay for the highest quality of work and materials used, deep attention to all details, complete immersion in the patient’s problem and solving it in the best way. We will organize for you the most professional assistance, high-tech and effective surgical techniques, competent rehabilitation and constant communication with your doctor to resolve all emerging issues. The cost of CABG (coronary artery bypass surgery) organized by Medis is from 250 thousand rubles or more. The same operation in Israel already costs from 25 thousand dollars, but it is worth doing. The complex, which includes an operation performed by Academician Akchurin, anesthesia and a stay in a premium hospital in Moscow for 7-10 days, will cost 720,081 rubles .
| Services | Cost, rub.) |
| CABG (coronary artery bypass grafting) | from 250,000 rubles |
| A complex including an operation performed by Academician Akchurin, anesthesia and stay in a premium hospital in Moscow for 7-10 days | 720,081 rubles |
The result of the operation is the restoration of normal blood supply in the large arteries of the heart, bypassing the sites of blockage, curing ischemia and eliminating the root cause of angina. The operation significantly reduces the risk of developing myocardial infarction, as well as the likelihood of sudden cardiac arrest. Thanks to successful surgery, life expectancy increases or the risk of problems with blood supply is completely eliminated.
Risks and complications
- postoperative bleeding;
- inflammatory process of a postoperative wound;
- respiratory complications;
- heart rhythm disturbances;
- pain associated with nerve fibers, muscle spasm or dislocation of costal cartilage;
- encephalopathy;
- cardiac weakness, perioperative myocardial damage, stroke, death.
Anyone can calculate the risk of surgery using the international table for calculating the risk of cardiac surgery EuroSCORE II, which takes a few minutes.
Indications for CABG surgery
- Severe angina (extensive, more than 50 percent, narrowing or blockage of several coronary arteries);
- Severe ischemic disease, with 50% or more obstruction of the left coronary artery;
- Cardiomyopathy, acute coronary syndrome.
Before heart bypass surgery in Moscow, patients must undergo a comprehensive examination, which we conduct according to an international protocol. Its cost is from 15,000 rubles and it takes on average 2-4 days. The examination includes the following procedures necessary to make an accurate diagnosis and further plan patient management tactics:
- Advanced laboratory tests of blood and urine;
- Electrocardiography and echocardiography, as well as stress echo CG;
- Daily monitoring using the Holter method;
- Coronary and angiography (x-ray of heart vessels with contrast);
- X-ray or computed tomography of the lungs;
- Appointment with a cardiologist and cardiac surgeon;
- Other tests may be required as prescribed by your doctor.
After a comprehensive diagnosis, a decision is made on the most effective surgical technique for the patient. In some cases, stenting is performed, that is, dilation of the vessel using a special wire tube - a stent, and in more severe cases, when the artery section is narrowed by 70 percent or more, CABG surgery is performed.
The cost of CABG may vary for different patients and will depend on individual indications, the scope of the operation, as well as the class of the selected surgeon. With us you will be able to be treated by real luminaries of cardiac surgery, renowned international specialists, which means that the quality of work will be impeccable and durable. In many cases, doctors try to carry out interventions using the most gentle, endoscopic methods, which, of course, are much easier to tolerate by patients.
The heart bypass operation for which we refer you to our hospital can be performed in different ways: with an opening of the chest on a beating heart with or without the use of a heart-lung machine, or on a stopped heart with artificial circulation. The final decision on the surgical technique is made by the cardiac surgeon based on the patient's needs. Parts of the patient's own arteries are taken as a shunt: from the chest, arms or legs. These vascular grafts are pulled from the aorta to the area below the blockage (the diseased artery itself is clamped to stop blood flow). The result of such manipulations is that blood begins to flow through a new, healthy artery. If the operation is performed endoscopically, that is, through small incisions, the blood flow is directed through the mammary artery instead of the blocked coronary artery.
The duration of a coronary bypass surgery with opening of the chest is approximately three to six hours, depending on the number of anastomoses. The duration of minimally invasive surgery is less - one to two hours. After the operation, the patient remains under the close supervision of doctors for at least a week in an equipped, comfortable hospital. Of course, a gentle type of operation is preferable for the patient, but it requires enormous skill of the surgeon. We will refer you to those doctors in Moscow who are fluent in any method of heart bypass surgery.
To find out the exact price of CABG (coronary artery bypass grafting) specifically in your case, as well as to ask any important questions, call or write to us, and we will advise you in detail and make an appointment for a consultation with a doctor.
During the examination:
ECG: sinus rhythm. Heart rate 63 per minute. Insufficient blood supply to the myocardium in the area of the posterolateral wall of the left ventricle.
EchoCG: the size of the heart is not increased, the ejection fraction (EF) of the left ventricle (LV) is 46%. The diameter of the aorta at the level of the sinuses of Valsalva is 3.5 cm, the ascending aorta is 4.0 cm, the walls are dense. The walls of the aortic valve are compacted, with isolated inclusions of calcium. Hypokinesis of the middle anterolateral segment of the LV. Severe atherosclerotic changes at the base of the aorta, moderate dilatation of the ascending aorta, disturbances of local LV contractility, decreased global LV systolic function, slight enlargement of the left atrium.
Coronary angiography: right type of coronary circulation. Stenosis of the LMCA trunk up to 70%, extended stenosis of the LAD in the middle segment up to 80%, circumflex artery in the proximal segment up to 80%. RCA stenosis in the proximal segment up to 70%. Occlusion of the posterior interventricular branch (POIB) with retrograde filling.
Ultrasound of the abdominal cavity: diffuse changes in the tissue of the liver and pancreas. Cholesterosis of the gallbladder wall. Along the ascending colon, a volumetric formation of a heterogeneous echostructure is determined; with duplex scanning, it is vascularized and connected to the wall of the colon.
Doppler ultrasound: S-shaped tortuosity of both ICAs with stenosis of their orifices by 40-55%. Acceleration of blood flow up to 0.8 m/s.
brain: mixed hydrocephalus.
Colonoscopy: tumor of the ascending colon. Two polyps of the sigmoid colon with a diameter of up to 1 cm. Dolichosigma. Histological examination of the biopsy specimen revealed a section of the colon mucosa and a tumor with the structure of a poorly differentiated adenocarcinoma with extensive necrosis.
CT scan of the abdominal organs: the liver and spleen are not enlarged. There are no focal liver formations. The retroperitoneal and mesenteric lymph nodes are visualized, enlarged to 1.8 cm. Adrenal glands without features. Localized 10 cm from the hepatic angle, diffuse circular thickening of the wall of the cecum and a segment of the ascending colon is noted with signs of obstruction of its lumen and a picture of extra-organ spread of the tumor over 6 cm. Perifocal tissue is diffusely infiltrated. The area of the small-colic junction is difficult to differentiate. Atherosclerosis of the aorta. Ostial stenosis of the renal arteries more than 50%.
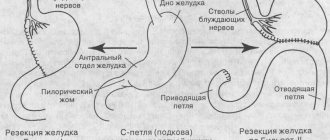
After a consultation consisting of leading specialists from the Russian Scientific Center for Surgery on October 29, a one-stage operation was performed: MCB and 2-CABG (Fig. 1) under IR conditions and extended right hemicolectomy (Fig. 2) with lymphadenotomy in the volume of D3.
Complete longitudinal median sternotomy with simultaneous sampling of the great saphenous vein from the left leg and thigh. The left internal mammary artery was isolated and externally treated with papaverine solution. Heparin was introduced. The pericardium was opened and placed on supports.
Rice. 1. Scheme of MKSh and 2KSh
Rice. 2. Scheme of right-sided hemicolectomy (B.E. Peterson et al. Atlas of oncological operations 1987)
Purse string sutures were placed on the aorta and right atrium. Cannulation according to the vena cava - aorta scheme. Start of CPB, cooling to 32° C. Antegrade pharmacocold cardioplegia with Custodiol solution. The aorta is compressed. During revision, the cervical vein is atherosclerotically changed throughout and is not shuntable. The posterolateral branch (PLB)2 with a diameter of 2 mm, originates from the RCA, is atherosclerotically changed in the proximal segment. The lumen of the WMV2 in the middle third was opened. An end-to-side anastomosis was formed between the autovein and the PV2 using a continuous wrapping suture using 7/0 prolene thread. ZMA1 with a diameter of 2 mm, atherosclerotically stenotic in the proximal segment. The latter was opened at the border of the middle and distal thirds, and an end-to-side anastomosis was formed with the autovein using a continuous wrapping suture using 7/0 prolene thread. The LAD is not visualized, lies deep in the epicardium, and is atherosclerotically changed up to the distal third. The lumen of the diagonal artery (DA) in the proximal third was opened. Artery with a diameter of 2 mm. An end-to-side anastomosis was formed between the left internal mammary artery and the DA using a continuous wrapping suture using 8/0 prolene thread. The clamp is removed from the aorta. With lateral compression of the aorta, two proximal anastomoses were formed. Prevention of air embolism. Cardiac activity was restored after a single defibrillation. The shunts are not tense by palpation, the discharge is satisfactory. Decrease IR performance, stop IR. Decannulation. Protamine The anastomoses are sealed (Fig. 3). The pericardium is partially sutured with a continuous suture.
Careful hemostasis. Two electrodes are sutured to the anterior wall of the right ventricle. Drains were installed in the pericardium and anterior mediastinum. Wire sutures were placed on the sternum. The wound is sutured in layers.
Rice. 3. Final view of the first stage of the simultaneous operation
The abdominal stage of the surgical intervention began after suturing the sternotomy wound. Complete longitudinal median laparotomy. During intraoperative inspection, focal formations in the liver are not identified. A tumor conglomerate measuring 10x15 cm is located in the projection of the lower third of the ascending colon, it involves the tissues of the right lateral canal, the tumor is moderately mobile. The first stage was an extended lymphadenectomy in the volume of D3 using a harmonic scalpel (Fig. 4). For this purpose, the distal part of the ileocolic vessels was visualized and skeletonized, and their identification was continued in the proximal direction until the origin of the middle colic vessels. The right colic artery and vein were isolated and ligated immediately after their departure from the superior mesenteric vessels using a LigaSure vessel sealer. The dome of the cecum and the ascending colon were mobilized while preserving their own intestinal fascia and removed en bloc with the fiber located along the superior mesenteric vessels and the peritoneum of the right lateral canal. The omental bursa was opened, the gastrocolic ligament was crossed with simultaneous mobilization of the greater omentum from the left flexure to the intersection of the colon. A platform was formed for transecting the transverse colon 15 cm proximal to the tumor. The transverse colon was transected at the level of the prepared platform. The ileum is divided 20 cm distal to the ileocecal angle using the TST 50 apparatus.
Rice. 4. Extended lymphadenectomy in volume D3 using a harmonic scalpel
Rice. 5. The drug is removed
The ends of the intestine are immersed in a purse-string suture. A double-row isoperistaltic ileotransverse anastomosis, side to side, was performed with 3/0 Vicryl thread. The mesenteric window is sutured with a continuous suture. Careful hemostasis is performed, leaving two drains in the right lateral canal and the pelvis. A suture was placed on the wound.
Duration of operation 600 minutes, IR 92 minutes, myocardial ischemia 44 minutes. Blood loss 1900 ml. Using the Cell-Saver device, 460 ml of autologous blood was returned.
Histological examination of the specimen: undifferentiated adenocarcinoma of the ascending colon with invasion of all layers and the peritoneum of the lateral canal, complicated by an extensive purulent inflammatory process in the tumor and surrounding tissue. Metastases in three lymph nodes (1-N3 and 2-N2).
An hour after the end of the operation, the patient experienced arterial bleeding through the drains at an extremely high rate (1000 ml over 1 hour). During relaparotomy, arterial bleeding was detected from a 2-mm lateral defect in the wall of the superior mesenteric artery (possibly caused by the discharge of a coagulation scab). Hemostasis was achieved by suturing the defect.
On October 30, a hemofiltration session was performed due to an increase in blood lactate to 16 mmol/l, blood creatinine to 2.5 mg/%.
On October 31, relaparotomy was performed again due to diffuse biochemical bleeding of the tissues of the right lateral canal. The bleeding was stopped using hemostatic sponges. The total volume of blood loss by October 31 was more than 10,000 ml. The expanded coagulogram corresponded to the picture of the hypocoagulation stage of DIC syndrome. All necessary intensive measures were carried out (transfusions of plasma, cryoprecipitate).
01.11 drainage was removed from the pericardium, mediastinum and pleural cavities. Since 01.11, a disturbance of the heart rhythm of the tachyform type of atrial fibrillation with paroxysms of atrial flutter, relieved by infusion of cordarone, has been noted. From the moment of the initial operation, hemodynamics were maintained by infusion of renal doses of cardiotonics.
02.11 the patient was extubated with satisfactory gas exchange rates, the administration of cardiotonics was stopped, a pleural puncture was performed, during which 500 ml of serous-hemorrhagic exudate was evacuated from the left pleural cavity.
On November 3, enteral feeding was started. On November 05, sinus rhythm was restored. On November 05, an episode of temperature rise to 40 °C was noted, blood cultures showed anaerobic flora, antibiotic therapy was intensified (Tie-nam 0.5 g 3 times a day, Metrogyl 500 mg 2 times a day).
The patient was discharged in satisfactory condition on the 20th day after surgery with recommendations for polychemotherapy at the place of residence:
Rice. 6. View of the patient before discharge (20th day after surgery)
After operation
Of course, your health will improve significantly after surgery. However, under unfavorable circumstances, plaques may begin to form again. Therefore, it is extremely important if you want to maintain health for many years, give up bad habits and lead a healthy lifestyle. Yes, this sounds trivial, but it is precisely this tactic that gives the greatest chance for a long life without relapses after surgery. If you smoke, you will have to give up cigarettes as soon as possible. This will normalize blood pressure and slow down the development of atherosclerosis. You definitely need to address the issue of obesity if it exists, lose extra pounds, eat healthy and balanced, try to be physically active - go for walks, engage in those types of physical exercise that your doctor allows you. A normal, not elevated, cholesterol level is very important for you, so you will need to greatly reduce fatty foods in your diet. Good eating habits should become a daily routine for you. Give preference to a diet containing fish, white poultry, and sufficient amounts of vegetables and fruits. You should not fry food; it is much healthier to bake, stew or boil it. In addition, you will be prescribed medications that you will need to take constantly.
By following all the recommendations of your doctor and leading a healthy lifestyle, you will protect yourself from relapses of the disease and the need for new treatment measures.
Patient reviews
Georgy Ts.: As they say, if aortic bypass surgery is performed perfectly, then you should forget about it, but if it’s mediocre, then you’ll live for three to five years and good luck. So I decided to do it perfectly, I found out from my specialist who was worth what and decided to order everything to be done by the Medis clinic. I will not say anything about choosing a doctor, but I chose from the best, a famous heart surgeon flew to Moscow for the operation, and his team was local, but from the best. And as they explained to me at Medis, nursing also means a lot for recovery, so they provided it at the level. Everything went well, material for a shunt was taken from my leg, since the veins in my leg are good. Israeli surgeon Amir Kramer performed surgery on me when my heart stopped. An Israeli doctor took care of me and controlled everything. This is, of course, a “special order”, that is, a product specially built for me, this is me as a gene. I'm talking to the director. This is how you can ensure the highest level of CABG performance.
Samvel Karapetyan: I asked to organize a coronary artery bypass surgery with Medis and for three hundred thousand everything was done very well, quickly and efficiently.