What happens to a person after gastric resection? Gastric resection is a surgical treatment of certain stomach diseases (complicated gastric ulcers, stomach tumors, etc.).
Depending on the nature of the operation, there may be total removal of the stomach, Billroth I resection, Billroth II resection and other modifications of operations. In the early stages after surgery, various medical and dietary measures are carried out in the hospital.
We will talk about the lifestyle of patients who underwent gastric surgery 5-6 months ago. I’ll say right away that stomach surgery is not a death sentence. Life after gastrectomy means many years of careful attention to yourself, a good quality of life, and proper nutrition. After the operation, the anatomical features of the gastrointestinal tract change, and the digestive processes in it also change.
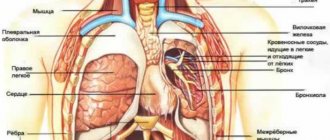
Let me remind you that the stomach is the organ where food enters from the oral cavity. It is subjected to deposition, mechanical and chemical processing and evacuation of stomach contents into the intestines. The duration of food in the stomach is from 1 to 3 hours, depending on its nature. After the operation, all functions of the stomach are lost. Nitrogenous substances in protein foods are quickly absorbed into the blood, which leads to disruption of the absorption of nitrogen by the tissues of the body, and nitrogen is excreted in the urine. The nitrogen balance in patients after surgery is disturbed; it becomes negative, i.e. More nitrogen is excreted in the urine than is taken in from protein foods. This leads to weight loss and weakness.
Surgeons should always warn a patient undergoing gastric surgery that the body weight lost before and after the operation cannot be restored, it will remain reduced, but this is not the main thing, the basis is a good quality of life and work capacity.
How does the gastrointestinal tract function after gastric resection?
The stomach takes part in hematopoiesis; the cells of the gastric mucosa produce intrinsic Castle factor, an enzyme that converts vitamin B12 from food into an absorbable form. Without intrinsic factor, vitamin B12 is not absorbed and does not enter the bloodstream, but is excreted in the feces. The source of vitamin B12 is animal food; there are no plant sources of B12. For more information about B12 deficiency anemia, read the article in the healthy lifestyle “Red vitamin and anemia (if blood is on a fast ration)” or on the website.
The first blow from food intake is the intestines, primarily the small intestine - this is the most extensive organ of the human digestive system. In it, under the influence of pancreatic enzymes and bile of intestinal juice, the main processes of digestion occur, transforming food into simple components that can be absorbed by the body, determine the state of metabolic processes and, ultimately, human health.
Pancreas. It produces 1.5-2.0 liters of pancreatic juice, which has a pH of 7.5. The main part of pancreatic juice is pancreatic enzymes (trypsin, chymotrypsin, elastase, carboxypeptidases, pancreatic lipase, phospholipases, etc.) Pancreatic juice contains a huge range of enzymes that digest almost all components (macronutrients) of food consumed by humans. These enzymes are produced only in the pancreas. In practice, the pancreas takes over the functions of the stomach in digesting protein foods.
Large intestine - carries out residual final digestion of food, secretion and absorption of water, electrolytes, gases, formation and evacuation of feces.
An important role is played by intestinal microflora, the enzymes of which utilize digestive enzymes secreted by the digestive organs. The breakdown products of enzymes and bile acids are absorbed into the blood and returned to the digestive organs for the re-synthesis of digestive enzymes and acids.
New paradigm
Although preexisting hypertension is a significant perioperative risk factor, it is important to recognize that acute circulatory hypertension per se, commonly observed during and after surgery, may differ in mechanism of occurrence and sensitivity to treatment from chronic preexisting hypertensive pathology. Likewise, acute circulatory hypertension is not quite the same as other acute hypertensions, which represent 1-2% of the overall spectrum of hypertensive diseases (Zampaglione et al, Hypertension 1996;27:144, Sullivan AF. Acad Emerg Med 2004;11:454; IOM Emergency Medical Care Report 2006, Cline DM Acad Emerg Med 2006).
The mechanisms of perioperative hypertension are: hyperadrenergic response to surgery, increased vascular systemic resistance, end-diastolic pressure deviations, rapid changes in intravascular volume, activation of the renin-angiotensin system, adrenergic stimulation (cardiac and nervous), overproduction of serotonin, baroreceptor denervation, impaired cardiac reflexes , inadequate anesthesia and local mechanical action (application of vascular occlusion clamps).
Conditions that change vascular tone (nervous, endothelial and mechanical) are essentially the same conditions that cause acute changes in local and/or systemic hemodynamics due to dilating or constricting effects, which in turn can subsequently initiate acute procoagulative and inflammatory reactions (JACC 2007, 50; 1-13, JACC 2003, 42; 1149-60). These induced changes in blood pressure (distension and/or tension), endothelial function, and CNS stimulation often coexist in some combination. Adverse vascular outcomes associated with acute fluctuations in blood pressure secondary to preexisting hypertension are accelerated by surgery; manifesting itself within a few days rather than weeks, as occurs without surgery, as follows from data from extensive studies of outcomes in patients with essential hypertension. The circumstances causing acute changes in hemodynamics during surgery are well known and include: acute changes in systemic vascular resistance depending on the depth of anesthesia, surgical exposure, occlusive compression and release of the aorta, redistribution of fluids, bleeding, side effects of medications, and much more. These changes usually occur in situations of CBF insufficiency and may affect patients differently depending on the initial vascular elasticity (Circ research 1968,23;567-79, Hypertension 2001,38;1461-6, Circ 1997,96;308-15 , N Engl J Med 1990,322;100-10, Am J Cardiol 1978,41;327-32, Hypertension 2005,46;200-4). There is a close relationship between age, duration of existence of arterial hypertension, specific vascular disease and pulsating disturbances in the aortic wall from surgical manipulations (compression and expansion of the aorta, insertion and removal of catheters) on the one hand and the inflammatory reaction associated with cardiopulmonary bypass, “providing” pathophysiological basis for the increased incidence of postoperative vascular complications, on the other hand, in patients with “non-law-abiding” arteries. These hemodynamic disturbances also contribute to endothelial dysfunction (Circ 2006,113;2335-62, Arterioscler Thombo Vasc Biol 2005,25;274-8). It has been established that changes in stretch and stress of the endothelial wall in the presence of endothelial plaques can contribute to inflammation and destabilization of the sensitive plaque with subsequent remodulation leading to necrosis of the vascular wall, loss of flexibility, increased vascular resistance and deterioration of organ perfusion. (Circ 2006,113;2679-82, Circ 2003, 108;17-23, Circ 2006,113;2335-62, JACC 2007, 49;2073-80, JACC 2007;49:2379-93, Eur Heart J 2007 ,28;705-10).)
| Cronic HTN - chronic hypertension Acute Circulatory HTN - acute circulatory hypertension HTN Emergencies - urgent cases of hypertension |
How to eat properly after gastric resection
Now, having understood the burden placed on the digestive organs, you can move on to the rules of a healthy lifestyle and, most importantly, nutrition.
- The first stage of digestion begins in the oral cavity, where food is mechanically processed and soaked in saliva. Thanks to saliva enzymes, the digestion of food in the gastrointestinal tract is facilitated. Under the action of salivary enzymes, simple sugars are absorbed in the oral cavity. You need to chew slowly, without rushing; if your teeth are good, you can chew a piece of meat.
- You need to eat often, 5-6 times a day, observing the rhythm of food entering the digestive tract.
- It is necessary to monitor the amount of food taken at one time; the volume should be no more than 1 glass (200 ml).
What are the dangers of surgery for low blood pressure?
Everyone knows that hypertension is very life-threatening. But low blood pressure is also associated with a certain amount of risk, especially when it comes to surgical interventions. If the patient has hypotension during the operation and for some time after it, death is possible.
These fears are supported by statistical data. Thus, over 252 thousand patients in need of surgical operations were under the supervision of doctors for a long time.
The determining factors during the examination of the patient were:
- health problems;
- floor;
- nationality;
- taking medications;
- objective risks during and after surgery;
- patient pressure.
It turned out that patients with low systolic pressure (less than 100 mm H.S.) were 40% more likely to die on the operating table or immediately after surgery. The situation was even worse for those whose lower indicator was less than 40 mm.r.s. – their risk of death increased two and a half times.
The presented statistical data allowed us to conclude that the attention of surgeons preparing patients with low blood pressure for operations cannot be called sufficient. The number of deaths convincingly proves this.
Now the question of whether it is possible to perform surgery for hypotension should be answered this way - with indicators close to critical (less than 100/below 40), this is extremely dangerous.
But a clear verdict has not yet been made.
Scientists have yet to find out whether taking medications that increase blood pressure will be an effective means for successful operations and a stable rehabilitation period.
Patients with hypotension are automatically at risk during surgical interventions, and after surgery, they should not only be aware of this, but also take measures to bring their condition back to normal.
How should the ratio of gastrointestinal tract change after gastric surgery?
Increased amounts of protein
must be included in the diet .
Among proteins, there is a hierarchy of the need for enzymes for their digestion: chicken egg white is the easiest to digest, then comes milk protein, which is one of the first places in terms of nutritional value. Next comes fish protein and then chicken, turkey, and animal proteins. The latter require quite a lot of enzymes, so it is better to prepare them in a thermally processed form. Culinary processing significantly increases digestibility, and with it the biological value of proteins. The amount of carbohydrates should be limited to prevent carbohydrate metabolism disorders and the occurrence of dumping syndrome. Reducing carbohydrates allows you to reduce the amount of food introduced. Carbohydrates are the main source of energy for the human body. Sources of carbohydrates in the diet are products of plant origin: yesterday's bread, cereals, potatoes, vegetables, fruits, berries, as well as sugar, honey, milk sugar in milk.
It has long been known that the digestive glands adapt to the composition of food: when the ratio of proteins, fats and carbohydrates in food changes, the composition of pancreatic juice will adequately change. The absorption of food proteins depends on the ratio of all nutrients in the diet, primarily fats, carbohydrates, vitamins, and minerals.
Fats support the metabolic processes constantly occurring in the body. Fats are needed both animal and vegetable in small quantities. It is important that vitamins A, E, D and K enter the body with fats, which do not dissolve in water.
After gastric surgery, the diet should be complete and contain sufficient amounts of vitamins. Pay special attention to vitamin B12 and folic acid, especially if the patient has anemia (see above).
In view of the often observed decrease in appetite after surgery, foods with high calorie content should be introduced into the diet . You need meat and fish dumplings, butter, cream, and broths. It is allowed to consume dairy products, cottage cheese, sour cream, and soft-boiled eggs. Include in your diet boiled and mashed porridge, vegetable and fruit purees, baked vegetables and fruits, stewed vegetables, jelly, compotes, jelly, jelly.
Introduction
Hypertension remains one of the most important preventable risk factors for heart disease and stroke; it is one of the direct causes of death in cardiovascular diseases in approximately 14-18% of cases (Circulation 2008,117;905-14). About 1/3 of the entire US population (70 million people) have some form of hypertension (Circulation 2005,112;1651-62, JAMA 2003;289;2560-72, Hypertension 2004;44,398-404, NHANES 1999-2004- Source , NCHS and NHLBI). Among those with hypertension, approximately 25% are treated, 25% are treated occasionally; in 50% of cases hypertension remains undiagnosed. (JAMA 2003;290;199-206, JAMA 2003;289;2560-72). According to several forecasts, approximately 90% of US residents will have hypertension by the age of 60-70 (JAMA 2002,287;1003-10, JAMA 2003;289;2560-72), that is, precisely the category of people who make up today the majority of the population is growing at a rapid pace (US Census Bureau. International data base at www.census.gov/ipc/www/idb/). Borderline hypertension (formally defined as “high usual BP”) also has a clear association with increased morbidity and mortality from cardiovascular disease, along with subclinical atherosclerosis and end-organ damage (Circulation 2007;115:593-9, Stroke 2005; 36,1859-63, Am J Cardiol 2004, 94;1496-1500). The annual cost of treating hypertension in the United States alone is $70 billion (Arch Intern Med; 1997;157:2413-46, Circulation. 2003;111:1094-1096). It is estimated that intensive BP control saves approximately $2000 per quality-adjusted life year (JAMA 2002.287;2542-51). According to public health experts, it is predicted that by 2025, about 1.5 billion people in the world will suffer from hypertension (Circulation. 2003;111:1094-1096). Cardiovascular disease, being both a cause and a consequence of hypertension, is the direct cause of death in 30% of people worldwide; these diseases are expected to remain one of the most serious public health problems in the coming decades. According to statistics, the number of deaths and re-hospitalizations due to acute hypertensive crises (8 and 38%, respectively) is almost equal to the number of similar outcomes due to acute coronary insufficiency (5-7% and 30%, respectively) and congestive heart failure (8, 5% and 26%, respectively) (OASIS -5 NEJM 2006, GUSTO IIb NEJM 1996, GRACE JAMA 2007, IMPACT - HF J Cardiac Failure 2004, STAT Registry preliminary results; SCCM 2008). Given that approximately 25 to 30 million people per year in the United States undergo surgery requiring anesthesia, and hypertension is a known risk factor for poor surgical outcomes, it should not be surprising that poorly controlled hypertension remains one of the most common causes of postponement of elective surgical interventions (J of Htn 2005, 23;19-22, JAMA 2002,287;2043-5).
For nearly a century, healthcare practitioners have considered hypertension as a cornerstone in the clinical assessment of cardiovascular dysfunction, cerebral dysfunction, dementia, and diabetes mellitus (Lancet. 2002;360(9349):1903-1913, Lancet. 2003;362:1527-1535, Anesth & Analg 95(5):1079-84, 2002, N Engl J Med 1996;335:1857-1863, Stroke 2004,35;1024-, Hypertension Research. 2005;28:385-407, Heart 2003,89;49- 53, Circulation 2007;115:733-42). Various studies have found that the risk of morbidity and mortality from cardiovascular diseases continuously increases proportionally with increasing blood pressure, even at blood pressure levels that are significantly lower than the recognized threshold in the standard definition of hypertension. So, at the age of 40 to 70 years, for every increase in systolic pressure by 20 mm Hg. or diastolic pressure by 10 mm Hg. the chances of developing cardiovascular disease double (within the blood pressure range of 115/75 to 185/115) (Circulation . 2003;111:1094-1096). Over time, significant advances have occurred in understanding both the characteristics of hypertensive conditions associated with morbidity and mortality, and the effectiveness and safety of antihypertensive therapy. It has been irrefutably proven that different phenotypes of blood pressure changes (mean, systolic, diastolic, pulse pressure) are independently associated with the development of adverse outcomes in outpatient practice (Benetos et al. J Hypertens.2003;21:1635-1640, Hypertension Research. 2005;28: 385-407, Am Jour of Card; 85, 2000, JNC VII - JAMA 2003, 289;2560-72). There is evidence indicating that a certain phenotype of blood pressure changes can be considered an independent risk factor for perioperative outcome (Anesth Analg 94;1079-84,2002, Anesth Analg 95;273-7,2002, Circulation 2007; 115: 733-42,) . Low preoperative diastolic pressure can serve as a basis for predicting perioperative risk, success or failure of antihypertensive therapy, and planning clinical trials (Br J Anaesth 1971;43;122-37, Arch Intern Med 2001;161:2343-50). Mean arterial pressure is widely regarded as an intraoperative index of perioperative risk, both in non-cardiac surgery (Ann Surg 1989,210;637-48, Ann Surg 1990,212;567-80, Anesthesiology 1979,50;285-92) and during heart surgery with cardiopulmonary bypass (J Thorac Cardiovasc Surg 1995, 110;1302-14, Anesthesiology 1996,83;701-8, Arch Neurology 2007, 64(8) e 1-4). Data have recently been published on the relationship between preoperative isolated systolic hypertension and perioperative outcome in cardiac and non-cardiac surgery (Anesth & Analg 2002;94:1079-84, Anesth & Analg 2002;95:273-7): the presence of isolated systolic hypertension is associated with 40% increased mortality after coronary artery bypass surgery. Interestingly, the latter indicator remains unchanged, regardless of the characteristics of preoperative antihypertensive therapy and other preoperative cardiovascular risk factors.
It has been shown that pulse pressure can also be considered as an important and independent prognostic factor for adverse postoperative outcomes in cardiac surgery (Circulation 2007; 115: 733-42). There is virtually no evidence of a relationship between high pulse pressure and outcomes in patients undergoing non-cardiac surgery. In the context of high-risk surgery and critical care, high (“dilated”) pulse pressure, occurring predominantly in the elderly, may be the most common and important preoperative hemodynamic abnormality.
A recent review on the topic of perioperative hypertension and risk (Br J Anaesthesia 2004, 92;570-83) points to the importance of patient-specific disease characteristics in assessing the perioperative risk of hypertensive stroke. Our traditional focus on hypertension “in general” as a factor influencing the degree of risk or a factor determining the characteristics of patient management does not contribute to the awareness of the insufficiency of our ideas in the field of targeted blood pressure control. Despite our efforts to understand the impact of different BP phenotypes in each individual patient under real-world conditions on perioperative outcome, a generally accepted strategy for perioperative BP control remains undeveloped.
| Type of adverse outcome | Event rate per group (%) | Odds ratio (OR) | |
| Without isolated high systolic pressure (n = 1457 people) | High isolated systolic pressure (n = 612 people) | ||
| Kidney failure | 6,7 | 8,8 | 1,3 (0,9-1,9) |
| Stroke | 6,3 | 10,1 | 1,7 (1,2-2,3) |
| Left ventricular dysfunction | 29,1 | 34,3 | 1,3 (1,0-1,6) |
| Renal failure, stroke, LV dysfunction, death | 33,2 | 40,9 | 1,4 (1,1-1,7) |
| Anesth Analg 94;1079-84,2002 |
Preoperative risk factors
| Preoperative risk factors | Grade |
| Age over 75 | 7 |
| Pulse pressure (mmHg) | |
| 40 | 0 |
| 41-60 | 4 |
| 61-80 | 8 |
| 81-100 | 12 |
| >100 | 16 |
| Anamnesis | |
| Congestive heart failure | 9 |
| Myocardial infarction | 6 |
| Kidney disease | 13 |
Intraoperative risk factors
| Intraoperative risk factors | Grade |
| Use of more than 2 inotropes | 10 |
| Intra-aortic balloon catheter | 15 |
| Cardiopulmonary bypass over 122 min | 6 |
| Circulation 115,733-42, 2007 |
Three rules of nutrition after gastric surgery
Experience shows that even with total removal of the stomach, the intestines and pancreas well compensate for the lack of gastric digestion. If belching or bitter regurgitation appears, you should limit cream, sour cream, sour and salty foods. They enhance these phenomena. They can be replaced with jelly, jelly, jelly, etc.
The absorption of food is influenced by the three most general patterns: 1. the relationship between the chemical composition of food and enzymes of the digestive tract, 2. the balance of the composition of food according to essential nutritional factors, and, finally, 3. compliance with a certain physiological rhythm of food entering the body, i.e. . strict diet.
Summary
For nearly a century, blood pressure control has remained the most important clinical goal of basic treatment, as poor or absent blood pressure control is consistently associated with cardiovascular disease morbidity and mortality. Despite the existence of close BP monitoring during surgery, not enough is known about the perioperative outcomes associated with inappropriate BP control. Perioperative hypertension is characterized by acute physiological changes, including excess catecholamine release, reperfusion injury, humoral and cellular inflammatory responses, and platelet activation, impairing microcirculation. Additionally, perioperative hypertension increases myocardial oxygen consumption and increases left ventricular end-diastolic pressure, which contributes to subendocardial hypoperfusion and myocardial ischemia, intraoperative bleeding and anastomotic dehiscence, and increases the risk of stroke, neurocognitive impairment and renal dysfunction. In surgical patients with preexisting hypertension, control of acute perioperative BP fluctuations is even more difficult as the therapeutic range of acceptable BP values narrows and shifts to the right. This is especially important in elderly patients with hypertension, who respectively require surgery and anesthesia in conditions of altered physiology of autoregulatory mechanisms.
It is now known that poor blood pressure control is an important prognostic factor for adverse postoperative outcomes in cardiovascular patients. It appears that targeted blood pressure control should reduce this risk. Much remains to be clarified in developing optimal BP control strategies and tactics based on the application of this concept in real-world conditions in individual patients. Perhaps nowhere else is the assessment, characterization and control of blood pressure more widely accepted and becoming more and more relevant than in the perioperative period. It is the perioperative period that is characterized by the presence of acute and stressful shifts, including excessive release of catecholamines, reperfusion injury, humoral and cellular inflammatory response and platelet activation, which impair microcirculation; It is this period that is very sensitive to acute circulatory hypertension.
Video on the topic
About methods of treating hypotension in the video:
Monitoring blood pressure is one of the most important commandments of a doctor during surgery; after surgery, the patient must independently monitor the condition of his body, immediately informing the doctor about the appearance of unwanted symptoms.
The information on the MyMedNews.ru website is for reference and general information, collected from publicly available sources and cannot serve as a basis for making a decision on the use of medications in the course of treatment.
MyMedNews.ru
And we also have
A sedentary lifestyle can shrink the brain and lead to dementia