- Circulatory and lymphatic systems
- How common is acute leukemia in adults?
- What causes acute leukemia and can it be prevented?
- How are acute leukemias in adults classified?
- Is early detection of leukemia possible?
- How is acute leukemia diagnosed?
- Treatment of acute leukemia in adults
- What happens after treatment of acute leukemia?
Leukemia (leukemia) is a malignant disease of white blood cells. The disease begins in the bone marrow and then spreads to the blood, lymph nodes, spleen, liver, central nervous system (CNS), and other organs. Leukemia can occur in both children and adults.
Leukemia is a complex disease and has many different types and subtypes. Treatment and outcome vary widely depending on the type of leukemia and other individual factors.
Circulatory and lymphatic systems
To understand the different types of leukemia, it is helpful to have basic information about the circulatory and lymphatic systems.
Bone marrow is the soft, spongy, inner part of bones. All blood cells are produced in the bone marrow. In infants, bone marrow is found in almost all the bones of the body. By adolescence, bone marrow is stored mainly in the flat bones of the skull, shoulder blades, ribs, and pelvis.
Bone marrow contains blood-forming cells, fat cells, and tissues that help blood cells grow. Early (primitive) blood cells are called stem cells. These stem cells grow (mature) in a specific order and produce red blood cells (erythrocytes), white blood cells (white blood cells) and platelets.
Red blood cells carry oxygen from the lungs to other tissues of the body. They also remove carbon dioxide, a waste product of cellular activity. A decrease in the number of red blood cells (anemia, anemia) causes weakness, shortness of breath and increased fatigue.
White blood cells help protect the body from germs, bacteria and viruses. There are three main types of leukocytes: granulocytes, monocytes and lymphocytes. Each type plays a special role in protecting the body against infection.
Platelets prevent bleeding from cuts and bruises.
The lymphatic system consists of lymphatic vessels, lymph nodes and lymph.
Lymphatic vessels resemble veins, but they do not carry blood, but a clear liquid - lymph. Lymph consists of excess tissue fluid, waste products and immune system cells
Lymph nodes (sometimes called lymph glands) are bean-shaped organs located along the lymphatic vessels. Lymph nodes contain cells of the immune system. They can increase in size more often during inflammation, especially in children, but sometimes their increase can be a sign of leukemia, when the tumor process has spread beyond the bone marrow.
Top
Diet for leukemia
There is no special diet for leukemia. Nutrition must be nutritious, since the pathological process occurring in the body leads to a weakening of the immune system. In order for the bone marrow to produce healthy blood cells, it needs large quantities of protein, carbohydrates, fats, vitamins, micro- and macroelements. Therefore, a child’s daily diet should include fruits, berries and vegetables. Freshly squeezed juices from pomegranate, carrots and beets are beneficial.
Due to anemia, you need to eat foods rich in iron. It is advisable to limit:
- fatty fish;
- fatty dairy products (can lead to metabolic disorders);
- baked goods, sweets;
- fried and smoked.
Replace pork with turkey or chicken.
How common is acute leukemia in adults?
In 2002, 8149 cases of leukemia were identified in Russia. Of these, acute leukemia accounted for 3257 cases, and subacute and chronic leukemia - 4872 cases.
It is estimated that 33,440 new cases of leukemia will be diagnosed in the United States in 2004. Approximately half of the cases will be acute leukemia. The most common type of acute leukemia in adults is acute myeloid leukemia (AML). At the same time, 11,920 new cases of AML are expected to be identified.
During 2004, 8,870 patients may die from acute leukemia in the United States.
The average age of patients with acute myeloid leukemia (AML) is 65 years. This is a disease of older people. The chance of developing leukemia for a 50-year-old person is 1 in 50,000, and for a 70-year-old it is 1 in 7,000. AML occurs more often in men compared to women.
Acute lymphoblastic leukemia (ALL) is more often diagnosed in children than in adults, and is most common before the age of 10 years. The probability of being diagnosed with ALL in a 50-year-old person is 1 in 125,000, and for a 70-year-old it is 1 in 60,000.
African Americans are 2 times less likely to develop ALL than the white population of America. Their risk of developing AML is also slightly lower than that of the white population.
With AML and ALL in adults, long-term remission or recovery can be achieved in 20-30% of cases. Depending on certain features of leukemia cells, the prognosis (outcome) of patients with AML and ALL may be better or worse.
Stages
Since in blood cancers the tumor as such does not develop, general staging criteria are not suitable for assessing their course. The initial stage of acute lymphoblastic leukemia is considered to be the period from the appearance of a malignant clone to the appearance of pronounced symptoms. Next, the following stages are distinguished.
- The first attack, or debut. At this time, the disease develops rapidly, the patient consults a doctor, is placed in a hematology hospital and undergoes induction therapy.
- Remission. It can be complete, with a decrease in the level of blast leukocytes of less than 5% and the presence of all healthy hematopoietic germs in the myelogram, and partial, in which the improvement in blood counts is temporary and stops after a certain period.
- Relapse. The condition occurs after remission and is characterized by the return of signs of the disease with an increase in the level of blastosis above 5%. There are early (with remission for less than a year) and late (with remission for more than a year) relapse of acute lymphoblastic leukemia.
Sometimes, after several remissions and relapses, the patient enters the terminal stage, in which the therapy does not produce any results. After this, death inevitably occurs. In most patients, treatment results are more favorable, and after remission, as a rule, recovery occurs.
What causes acute leukemia and can it be prevented?
A risk factor is something that increases the likelihood of disease. Some risk factors, such as smoking, can be eliminated. Other factors, such as age, cannot be changed.
Smoking is a proven risk factor for acute myeloid leukemia (AML). Although many people know that smoking causes lung cancer, few realize that smoking can affect cells not directly exposed to smoke.
Cancer-causing substances found in tobacco smoke enter the bloodstream and spread throughout the body. One fifth of AML cases are caused by smoking. People who smoke should try to quit smoking.
There are some environmental factors that have been linked to the development of acute leukemia. For example, long-term exposure to gasoline is a risk factor for AML, and exposure to high doses of radiation (atomic bomb explosion or nuclear reactor incident) increases the risk of AML and acute lymphoblastic leukemia (ALL).
People who have had other cancers and were treated with certain anticancer drugs are at increased risk of developing AML. Most of these cases of AML occur within 9 years of treatment for Hodgkin's disease (lymphogranulomatosis), non-Hodgkin's lymphoma (lymphosarcoma), ALL, or other malignancies such as breast and ovarian cancer.
There is some concern regarding high-voltage transmission lines as a risk factor for leukemia. According to some data, in these situations the risk of leukemia is not increased or increased slightly. What is clear is that most cases of leukemia are not associated with high-voltage transmission lines.
A small number of people with very rare diseases or the HTLV-1 virus have an increased risk of developing acute leukemia.
However, most people with leukemia have no identified risk factors. The cause of their illness remains unknown to this day. Due to the fact that the cause of leukemia is unclear, there are no methods of prevention, with the exception of two important points: avoid smoking and contact with substances that cause cancer, such as gasoline.
Questions and answers
How long do people live with acute lymphoblastic leukemia?
The disease has a rapid course, so without medical care, death occurs within a few months. With timely treatment, 80-90% of children and about 40% of adults have a chance to live more than 7 years.
How long does treatment for acute lymphoblastic leukemia last?
- The preparatory stage of treatment lasts 1-2 weeks.
- Induction – up to 8 weeks.
- Consolidation – up to 4 months.
- Reinduction – several months.
- Maintenance therapy – up to one and a half years.
The total duration of treatment is approximately two or two and a half years.
How do you know if you have acute lymphoblastic leukemia?
If you have:
- symptoms of general malaise – lethargy, weakness, fever;
- bleeding from the nose, gums, and other mucous membranes;
- poorly healing wounds on the skin;
- severe sweating at night -
It is necessary to contact an oncologist or hematologist as soon as possible and have tests done. The listed symptoms do not always indicate the onset of acute lymphoblastic leukemia, but this disease develops rapidly and aggressively. For the success of treating roads literally every day.
Attention! You can cure this disease for free and receive medical care at JSC "Medicine" (clinic of Academician Roitberg) under the State Guarantees program of Compulsory Medical Insurance (Compulsory Medical Insurance) and High-Tech Medical Care. To find out more, please call +7(495) 775-73-60, or on the VMP page for compulsory medical insurance
How are acute leukemias in adults classified?
Most tumors are classified into stages of disease (I, II, III, and IV), which are based on the size of the tumor and its extent.
This staging is not appropriate for leukemia because leukemia is a disease of the blood cells that does not usually cause tumor formation.
Leukemia affects the entire bone marrow and in many cases, by the time of diagnosis, has already involved other organs in the process. In leukemia, laboratory studies of tumor cells make it possible to clarify their characteristics, which help in assessing the outcome (prognosis) of the disease and choosing treatment tactics.
Three subtypes of acute lymphoblastic leukemia and eight subtypes of acute myeloid leukemia have been identified.
There are four main types of leukemia:
acute versus chronic
lymphoblastic versus myeloid
"Acute" means rapidly developing. Although the cells grow quickly, they are not able to mature properly.
"Chronic" means a condition where the cells appear mature but are actually abnormal (altered). These cells live too long and replace some types of white blood cells.
"Lymphoblastic" and "myeloid" refer to the two different types of cells from which leukemia arises. Lymphoblastic leukemia develops from bone marrow lymphocytes, myeloid leukemia arises from granulocytes or monocytes.
Leukemia can occur in both children and adults, but different types of leukemia predominate in one group or the other.
Acute lymphoblastic leukemia (ALL)
— Occurs in children and adults
- More often diagnosed in children
— Accounts for slightly more than half of all cases of leukemia in children
Acute myeloid leukemia (AML) (often called acute nonlymphoblastic leukemia)
- Affects children and adults
— Accounts for less than half of all cases of leukemia in children
Chronic lymphocytic leukemia (CLL)
- Occurs only in adults
— Detected twice as often as chronic myeloid leukemia (CML)
Chronic myeloid leukemia (CML)
- Mainly affects adults and is very rarely detected in children
— CLL is diagnosed twice as rarely.
Causes and risk factors
The direct cause of the disease is always a malignant mutation of cells of the hematopoietic system, due to which they become capable of rapid uncontrolled reproduction. There is an assumption that changes in the genome occur during intrauterine development, but until a certain point the process remains incomplete. External circumstances often become the “trigger”:
- radioactive radiation of any nature, including during treatment of other forms of cancer;
- some chemical compounds - benzene, certain chemotherapy drugs;
- viral infections (Epstein-Barr, HTLV);
- inherited predisposition.
Acute lymphocytic leukemia often develops in children, less often in people over 60 years of age, and very rarely in adults. Representatives of the white race get sick more often than blacks, men – somewhat more often than women.
How is acute leukemia diagnosed?
Leukemia can be accompanied by many signs and symptoms, some of which are nonspecific. Please note that the following symptoms most often occur with diseases other than cancer.
Common symptoms of leukemia may include fatigue, weakness, weight loss, fever, and loss of appetite.
Most symptoms of acute leukemia are caused by a decrease in the number of red blood cells as a result of the replacement of normal bone marrow, which produces blood cells, with leukemia cells. As a result of this process, the patient's number of normally functioning red blood cells, white blood cells and platelets decreases.
Anemia (anemia) is the result of a decrease in the number of red blood cells. Anemia leads to shortness of breath, fatigue and pale skin.
A decrease in the number of white blood cells increases the risk of developing infectious diseases. Although leukemia patients may have very high white blood cell counts, these cells are not normal and do not protect the body from infection.
A low platelet count can cause bruising, bleeding from the nose and gums.
Spread of leukemia beyond the bone marrow to other organs or the central nervous system can cause various symptoms such as headache , weakness , seizures , vomiting , and disturbances in gait and vision .
Some patients may complain of pain in the bones and joints due to their damage by leukemia cells.
Leukemia can lead to an increase in the size of the liver and spleen . If the lymph nodes are affected, they may become enlarged.
In patients with AML, gum disease causes swelling, tenderness, and bleeding. Skin lesions are manifested by the presence of small multi-colored spots that resemble a rash.
In T-cell type ALL, the thymus gland is often affected . A large vein (superior vena cava), which carries blood from the head and upper extremities to the heart, runs next to the thymus gland. An enlarged thymus gland can put pressure on the trachea, causing coughing, shortness of breath, and even suffocation.
When the superior vena cava is compressed, swelling of the face and upper extremities is possible (superior vena cava syndrome). This can cut off the blood supply to the brain and be life-threatening. Patients with this syndrome should begin treatment immediately.
The presence of some of the above symptoms does not mean that the patient has leukemia. Therefore, additional studies are carried out to clarify the diagnosis and, if leukemia is confirmed, its type.
Blood test.
Changes in the number of different types of blood cells and their appearance under a microscope may suggest leukemia. Most people with acute leukemia (ALL or AML), for example, have too many white blood cells and not enough red blood cells and platelets. In addition, many white blood cells are blast cells (a type of immature cell that does not normally circulate in the blood). These cells do not perform their function.
Bone marrow examination.
A small amount of bone marrow is removed using a thin needle for testing. This method is used to confirm the diagnosis of leukemia and evaluate the effectiveness of treatment.
Lymph node biopsy.
In this procedure, the entire lymph node is removed and then examined.
Spinal tap.
During this procedure, a thin needle is inserted in the lower back into the spinal canal to obtain a small amount of cerebrospinal fluid, which is examined for leukemia cells.
Laboratory research.
To diagnose and clarify the type of leukemia, various special methods are used: cytochemistry, flow cytometry, immunocytochemistry, cytogenetics and molecular genetic studies. Specialists study bone marrow, lymph node tissue, blood, and cerebrospinal fluid under a microscope. They evaluate the size and shape of the cells, as well as other characteristics of the cells, to determine the type of leukemia and the degree of maturity of the cells.
Most immature cells are blast cells, unable to fight infection, which replace normal mature cells.
- X-rays are taken to identify tumor formations in the chest cavity, damage to bones and joints.
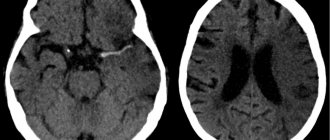
- Computed tomography (CT) is a special X-ray method that allows you to examine the body from different angles. The method is used to detect lesions in the chest and abdominal cavities.
- Magnetic resonance imaging (MRI) uses strong magnets and radio waves to produce detailed images of the body. The method is especially suitable for assessing the condition of the brain and spinal cord.
- Ultrasound examination (ultrasound) makes it possible to distinguish tumor formations and cysts, as well as the condition of the kidneys, liver and spleen, and lymph nodes.
- Lymphatic and bone system scan: In this method, a radioactive substance is injected intravenously and accumulates in the lymph nodes or bones. Allows differentiation between leukemic and inflammatory processes in lymph nodes and bones.
Symptoms
The first manifestations of acute lymphoid leukemia are nonspecific and are characteristic of many diseases:
- pale skin due to developing anemia;
- lethargy, loss of strength, drowsiness;
- frequent infectious diseases due to decreased immunity;
- elevated body temperature.
With the development of the disease, an increase in the number of blast lymphocytes in the blood and a lack of healthy cells, more pronounced symptoms appear:
- bleeding of mucous membranes;
- bruises, pinpoint skin hemorrhages;
- long-term healing of even small scratches and wounds, accompanied by infection, inflammation, suppuration;
- pain in the limbs caused by the growth of a bone marrow tumor;
- an increase in the size of the liver, spleen, lymph nodes, leading to abdominal pain;
- difficulty breathing, shortness of breath;
- paralysis of the facial nerve, blurred vision, vomiting due to damage to the meninges.
In each individual case, an individual symptom complex is formed, which may include the listed signs partially or completely.
Treatment of acute leukemia in adults
Acute leukemia in adults is not one disease, but several, and patients with different subtypes of leukemia respond differently to treatment.
The choice of therapy is based both on the specific subtype of leukemia and on certain characteristics of the disease, called prognostic features. These features include the patient's age, white blood cell count, response to chemotherapy, and whether the patient has previously been treated for another tumor.
Chemotherapy
Chemotherapy refers to the use of drugs that destroy tumor cells. Typically, anticancer drugs are prescribed intravenously or orally (by mouth). Once the drug enters the bloodstream, it is distributed throughout the body. Chemotherapy is the main treatment method for acute leukemia.
Chemotherapy for acute lymphoblastic leukemia (ALL).
Induction . The goal of treatment at this stage is to destroy the maximum number of leukemia cells in a minimum period of time and achieve remission (no signs of the disease).
Consolidation . The goal at this stage of treatment is to destroy those tumor cells that remain after induction.
Maintenance therapy . After the first two stages of chemotherapy, leukemia cells may still remain in the body. At this stage of treatment, low doses of chemotherapy are prescribed for two years.
Treatment of damage to the central nervous system (CNS) . Due to the fact that ALL often spreads into the membranes of the brain and spinal cord, patients are injected with chemotherapy into the spinal canal or given radiation therapy to the brain.
Chemotherapy for acute myeloid leukemia (AML):
Treatment of AML consists of two phases: remission induction and therapy after remission is achieved.
During the first phase, most normal and leukemic bone marrow cells are destroyed. The duration of this phase is usually one week. During this period and for the next few weeks, the white blood cell count will be very low and therefore measures will be required against possible complications. If remission is not achieved as a result of weekly chemotherapy, repeated courses of treatment are prescribed.
The goal of the second phase is to destroy the remaining leukemia cells. Treatment for a week is then followed by a period of bone marrow recovery (2-3 weeks), then chemotherapy courses are continued several more times.
Some patients are given very high doses of chemotherapy to kill all the bone marrow cells, followed by a stem cell transplant.
Side effects.
In the process of destroying leukemia cells, normal cells are also damaged, which, along with tumor cells, also grow rapidly.
Cells in the bone marrow, oral and intestinal mucosa, and hair follicles grow rapidly and are therefore exposed to chemotherapy.
Therefore, patients receiving chemotherapy have an increased risk of infection (due to a low white blood cell count), bleeding (low platelet count), and increased fatigue (low red blood cell count). Other side effects of chemotherapy include temporary baldness, nausea, vomiting, and loss of appetite.
These side effects usually go away soon after chemotherapy is stopped. Typically, there are methods to combat side effects. For example, antiemetic drugs are given along with chemotherapy to prevent nausea and vomiting. Cell growth factors are used to increase the white blood cell count and prevent infection.
You can reduce the risk of infectious complications by limiting contact with germs by thoroughly cleaning your hands and eating specially prepared fruits and vegetables. Patients receiving treatment should avoid crowds and patients with infection.
During chemotherapy, patients may be given strong antibiotics to further prevent infection. Antibiotics may be given at the first sign of infection or even earlier to prevent infection. If the number of platelets decreases, a platelet transfusion is possible, as is a transfusion of red blood cells if there is a decrease and the occurrence of shortness of breath or increased fatigue.
Tumor lysis syndrome is a side effect caused by the rapid breakdown of leukemia cells. When tumor cells die, they release substances into the bloodstream that damage the kidneys, heart and central nervous system. Giving the patient plenty of fluids and special medications will help prevent the development of severe complications.
Some patients with ALL, after treatment, may later develop other types of malignant tumors: AML, non-Hodgkin lymphoma (lymphosarcoma), or others.
Chemotherapy damages both tumor and normal cells. Stem cell transplantation allows doctors to use high doses of anticancer drugs to improve the effectiveness of treatment. And although anticancer drugs destroy the patient's bone marrow, the transplanted stem cells help restore bone marrow cells that produce blood cells.
Stem cells are taken from the bone marrow or peripheral blood. Such cells are obtained both from the patient himself and from a selected donor. In patients with leukemia, donor cells are most often used, since there may be tumor cells in the bone marrow or peripheral blood of patients.
The patient is prescribed chemotherapy with very high doses of drugs to destroy tumor cells. In addition to this, radiation therapy is given to destroy any remaining leukemia cells. After such treatment, the preserved stem cells are given to the patient in the form of a blood transfusion. Gradually, the transplanted stem cells engraft into the patient's bone marrow and begin to produce blood cells.
Patients who have received donor cells are given drugs to prevent the cells from being rejected, as well as other drugs to prevent infections. 2-3 weeks after the stem cell transplant, they begin to produce white blood cells, then platelets, and eventually red blood cells.
Patients who have undergone SCT should be protected from infection (stay in isolation) until the necessary increase in the number of leukocytes. Such patients are kept in the hospital until the leukocyte count reaches about 1000 per cubic meter. mm of blood. Then, almost every day, such patients are observed in the clinic for several weeks.
Stem cell transplantation is still a new and complex treatment option. Therefore, such a procedure should be carried out in specialized departments with specially trained personnel.
Side effects of TSC.
Side effects of TSC are divided into early and late. Early side effects differ little from complications in patients receiving chemotherapy with high doses of anticancer drugs. They are caused by damage to the bone marrow and other fast-growing tissues of the body.
Side effects can persist for a long time, sometimes years after the transplant. Late side effects include the following:
- Radiation damage to the lungs, leading to shortness of breath.
- Graft-versus-host disease (GVHD), which occurs only when cells are transplanted from a donor. This serious complication occurs when cells of the donor's immune system attack the skin, liver, oral mucosa and other organs of the patient. In this case, the following are observed: weakness, increased fatigue, dry mouth, rash, infection and muscle pain.
- Damage to the ovaries, leading to infertility and menstrual irregularities.
- Damage to the thyroid gland causing metabolic disorders.
- Cataract (damage to the lens of the eye).
- Bone damage; If the changes are severe, part of the bone or joint may need to be replaced.
Radiation therapy (the use of high-energy X-rays) plays a limited role in the treatment of patients with leukemia.
In adult patients with acute leukemia, radiation may be used if the central nervous system or testicles are affected. In rare emergency cases, radiation therapy is prescribed to relieve compression of the trachea by the tumor process. But even in this case, chemotherapy is often used instead of radiation therapy.
When treating patients with leukemia, unlike other types of malignant tumors, surgery is usually not used. Leukemia is a disease of the blood and bone marrow and cannot be cured with surgery.
During the treatment of a patient with leukemia, a small surgical intervention can be used to insert a catheter into a large vein to administer antitumor and other drugs and draw blood for research.
List of sources
- Savchenko V.G., Parovichnikova E.N. Acute leukemia//Clinical oncohematology: a guide for doctors. Ed. Volkova M.A.. 2nd ed., revised. and additional 2007
- Blindar, Valentina Nikolaevna Algorithm for laboratory diagnosis of acute leukemia. Guide for doctors / Blindar Valentina Nikolaevna. — M.: Medical Information Agency (MIA), 2013
- Gavrilov, O.K. Bone marrow and peripheral blood cells / O.K. Gavrilov, G.I. Kozinets, N.B. Chernyak. — M.: Medicine, 2014
- Davidenkova, E.F. Clinic and genetics of leukemia / E.F. Davidenkova, S.I. Sherman, N.N. Kolosova. — M.: Medicine, 2010
What happens after treatment of acute leukemia?
After completion of treatment for acute leukemia, dynamic observation in the clinic is necessary. Such observation is very important, as it allows the doctor to monitor possible relapse (return) of the disease, as well as side effects of therapy. It is important to tell your doctor immediately if you experience any symptoms.
Typically, relapse of acute leukemia, if it occurs, occurs during treatment or shortly after its completion. Relapse develops very rarely after remission, the duration of which exceeds five years.
Prevention of leukemia
Primary prevention of leukemia in children (that is, carried out before the disease develops) includes:
- strengthening the immune system in order to reduce the risk of contracting infectious diseases (proper nutrition, hardening, etc.);
- avoiding contact with carcinogens, sources of ionizing radiation, and potentially hazardous chemicals.
After the onset of leukemia, secondary prevention is possible. It involves undergoing regular preventive examinations in order to timely detect relapses.
This article is posted for educational purposes only and does not constitute scientific material or professional medical advice.
Palliative care
There are a large number of treatment methods available for the treatment of acute leukemia. This could be chemotherapy, targeted therapy, immunotherapy. All these methods can lead to remission even after multiple relapses. Therefore, as such, palliative therapy is rarely prescribed and, as a rule, in older patients who cannot tolerate severe treatment.
In this case, chemotherapy, drug therapy and radiation therapy are used.
Chemotherapy
Chemotherapy in palliative treatment is not carried out with the goal of achieving remission, but to keep the tumor clone from rapidly multiplying. At this stage, standard cytostatic drugs in lower dosages, immunotherapy, targeted therapy and other methods of antitumor treatment can be used.
Radiation therapy
Radiation therapy can be used to relieve pain in severe bone damage, as well as in the presence of extramedullary lesions.
Diagnostics
Since the disease develops very quickly, when contacting an oncologist or oncohematologist, the symptoms of acute lymphoid leukemia are usually already pronounced. However, to confirm the diagnosis and determine treatment methods, laboratory tests are necessary, as well as instrumental studies:
- general and biochemical blood tests;
- myelogram - study of bone marrow cells, cytochemical analysis, immunophenotyping;
- spinal cord puncture with histological and cytological examination of the biopsy;
- Ultrasound of internal organs and lymph nodes;
- chest x-ray;
- ECG and other studies according to symptoms.