Why does the left side of my head hurt?
Physiological reasons
Under certain circumstances, pain in half the head can occur in a healthy person. Features of the pain syndrome are episodic in nature, rapid disappearance after rest or taking an analgesic. The symptom is observed in the following cases:
- Intense physical activity
. A combination with darkening of the eyes, dizziness, shortness of breath, palpitations and tingling in the heart area is possible. - Stressful situations
. The left or right half of the head hurts due to the release of stress hormones, causing vasoconstriction and increased blood pressure. There is pronounced emotional stress. - Mental fatigue
. Pain is caused by significant mental stress, as well as the need for prolonged concentration and tension when staying in one position, for example, when preparing for an exam or working at a computer. - Bad habits
. The symptom sometimes appears with the abuse of tonic drinks (coffee, strong tea, energy drinks), smoking and drinking alcohol. The cause is changes in vascular tone and the entry of toxic substances into the body.
Cluster headache
It develops in people of a certain type - it affects mainly tall men with an athletic build, ambitious but indecisive. The pain syndrome develops acutely, reaches a peak within a few minutes, lasts from 15 minutes to 3 hours. The pain most often occurs in the left side of the head. It is most strongly expressed in the orbit, burning, stabbing, unbearable, reminiscent of a “rupture” or “squeezing out” of the eye. Cluster headache is accompanied by autonomic disorders. It decreases with movement, so patients rush around and punch the wall.
Migraine
During a migraine, the left side of the head hurts somewhat less frequently than the right side. The pain is pressing, throbbing, with the epicenter in the temple, forehead or eye. Sometimes painful sensations arise in the back of the head, and from there spread to the entire half of the head. A typical sign of pathology is the periodic change of the affected side. Manifestations vary slightly depending on the type of migraine:
- Simple migraine.
Diagnosed in 80% of cases. There is no aura. A prodrome in the form of drowsiness, worsening mood, and decreased performance is possible. Hemicrania is combined with nausea and vomiting, and intensifies with movements and exposure to auditory and sound stimuli. Lasts from 4 hours to 2-3 days. - Migraine with aura.
The attack itself proceeds in the same way as with a simple migraine. The difference lies in the presence of an aura - visual disturbances, transient sensitivity disorders, ringing in the ears, the appearance of unusual smells or sounds, and deterioration of speech. Migraine in children is often preceded by “Alice syndrome” - visual distortion of objects, visual hallucinations. Lasts from several hours to 4 days. - Ocular migraine.
Typically there is loss of certain areas of the visual field, the presence of paracentral or central scotomas, and flickering before the eyes. The headache is throbbing, occurs in the forehead, moves to the orbit. The duration of visual disturbances is 10-20 minutes, the duration of an attack of cephalgia is 30-120 minutes. - Vestibular migraine.
Manifests with a prodrome, which is subsequently joined by dizziness, sometimes in combination with other variants of the aura. Then half of the patients develop pain in the left or right side of the head, lasting no more than 3 days. Dizziness stops with the onset of hemicrania, persists throughout the entire painful attack or becomes its only manifestation (painless paroxysms).
If the symptom persists for more than 3 days or a series of continuous paroxysms during this time, they speak of migraine status. The pain is very intense, wave-like. Pallor, adynamia, severe weakness, inability to take food and medications due to repeated vomiting, and increasing dehydration are observed. The condition is serious.
Pain in the left side of the head
Paroxysmal hemicrania
Unilateral pain is paroxysmal, very severe. It can be aching, pulsating, burning, boring, stabbing or reminiscent of a fist blow. It is localized mainly in the temple or orbit, less often in the area of the forehead, back of the head or crown of the head. Associated with damage to the trigeminal nerve. An attack of paroxysmal hemicrania lasts from 5 to 45 minutes; during the period of exacerbation, from 1 to 40 episodes can be observed per day. It is supplemented by vegetative symptoms, drooping eyelids, constriction of the pupil, and photophobia.
Vertebrobasilar insufficiency
Left-sided or right-sided headache is observed in the spondylogenic form of vertebrobasilar insufficiency. Develops suddenly with movement. From the neck and back of the head it spreads to the forehead, temple and eye socket, and radiates into the arm. A clear connection is revealed between the intensity of cephalalgia and the position of the cervical spine. The pain syndrome is complemented by unilateral hearing loss, noise in the ear, dizziness, visual disturbances, cerebellar disorders and autonomic reactions.
Hypnic headache
It is observed in people over 50 years of age and is chronic. It always develops during sleep, in 40% of cases it occurs only in the left or right half, in other cases it spreads to the entire head. An attack of hypnic headache forces the patient to wake up. On average, it lasts 30-60 minutes, repeats from once a week to several paroxysms throughout the night. The painful sensations are dull, moderately expressed, less often intense. Mild nausea and increased sensitivity to sounds and bright light may occur.
Cerebral tumors
Local pain in the left side of the head becomes an early symptom of tumors on the left side. Deep, bursting, quite intense, often occurring in the form of paroxysms. As neoplasia progresses, hemicrania is complemented by increasing focal symptoms. Then there are cerebral manifestations caused by edema and intracranial hypertension. The pain becomes diffuse, bilateral, accompanied by dizziness, nausea, and vomiting.
Arachnoiditis
The left half of the head may hurt with limited arachnoiditis, which developed in the long-term period after a head injury, inflammatory and infectious diseases. Symptoms increase gradually. The pain is bursting, more disturbing in the morning, combined with emotional instability, fatigue, irritability, and sleep disturbances. Subsequently, focal symptoms may develop, the process may spread with diffuse headaches and liquorodynamic crises.
Other reasons
Pain in the left side of the head is provoked by certain rheumatic and otolaryngological pathologies and diseases of the spine. The cause of the symptom is:
- Horton's disease.
The pain is one- or two-sided, dull, throbbing, with an epicenter in the temple area, intensifying at night, growing over several weeks. Fever, anorexia, myalgia, arthralgia, thickening and tenderness of the temporal and parietal arteries are noted. - Sinusitis.
Left-sided hemicrania accompanies unilateral frontal sinusitis and sinusitis with damage to the left paranasal sinus. Pulsating, bursting, localized in the eyebrow and forehead area, radiating to the temple. Complemented by general hyperthermia, intoxication, nasal discharge. - Mastoiditis.
Develops against the background of purulent otitis media. Accompanied by intense pain in the ear and behind the ear, which spreads to the crown, temple, orbit and upper jaw, sometimes covering the entire half of the head. Febrile temperature, intoxication, and profuse suppuration from the ear are observed. - Spine pathologies
. Unilateral compression of blood vessels and nerves due to osteochondrosis, protrusion, hernia and some other diseases of the cervical spine causes pain in the left half of the head. It is accompanied by pain in the neck, and sometimes by numbness and weakness of the upper limb.
Feelings experienced by the patient
Before consulting a neurologist, the patient should listen to himself so that during the appointment he can describe as accurately as possible exactly how his head hurts at one point. Feelings may be as follows:
- Sharp and sudden pain, reminiscent of a puncture with a sharp needle.
- Localization of the problem: headache in one point - on the top of the head, in the back of the head or in another place.
- The vision becomes dark when an attack occurs, or perhaps the patient lost consciousness during an exacerbation of a migraine.
- During an attack, the patient observes any shadows, flickering on the left or right, darkening of some areas in the field of vision.
It will also be necessary to clarify how long the attacks last - a few seconds or minutes? The more detailed the patient describes the symptoms to the neurologist, the easier it will be to draw up a clinical picture for prescribing appropriate treatment.
Diagnostics
A neurologist is involved in determining the nature of the disease that provokes pain in the left half of the head. According to indications, a rheumatologist, oncologist, and otolaryngologist are involved. Primary cephalgia (migraine, cluster and hypnic headache, paroxysmal hemicrania) are diagnosed based on clinical symptoms, auxiliary methods are prescribed to exclude organic pathology.
In other cases, when establishing a diagnosis, they rely on both objective data and the results of imaging and laboratory techniques. The examination program includes the following procedures:
- Echoencephalography.
It is produced to measure intracranial pressure and helps to exclude conditions accompanied by intracranial hypertension. Despite the possibility of detecting volumetric processes, in the early stages of tumors it may not be informative due to the small size of the formations. - Assessment of cerebral blood flow
. Includes duplex scanning, ultrasound examination of the vessels of the head and neck. As part of differential diagnosis, it allows you to detect hemodynamic disorders characteristic of atherosclerosis and other diseases. Recommended for patients with vertebrobasilar insufficiency to clarify the nature and structure of the stenosis. - Radiography
. Standard photographs of the cervical spine reveal signs of hernia, osteochondrosis and other diseases of the spinal column. To confirm extravasal compression of the vertebral artery, radiographs with functional tests are taken. For sinusitis, an X-ray of the paranasal sinuses is performed, and for mastoiditis, an X-ray of the temporal bone is performed. - Tomography
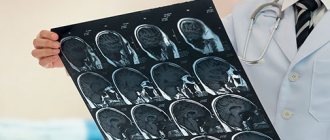
. MRI of the brain is prescribed for suspected tumors and arachnoiditis. In angiography mode, it provides comprehensive information about the condition of the main arteries. If a vertebrogenic etiology of pain is suspected, MRI and CT of the cervical spine are performed. For sinusitis, an MRI of the sinuses is sometimes performed.
Consultation with a neurologist
Advice from neurologists: how to avoid the development of cluster and point pain
A list of simple recommendations that will help prevent the development of migraines of any etiology and diseases that provoke them:
- You need to sleep at least eight hours every night. no matter what problems the patient may be experiencing, no matter what stress he may be experiencing, a good night’s sleep should be a must.
- Good nutrition is the basis of a healthy nervous system. Under no circumstances should you adhere to strict diets and starve yourself - even if the consequences do not appear immediately, they will come over time (the nervous system exhausted by fasting does not forgive such an attitude).
- A sufficient amount of amino acids, vitamins and microelements in the diet.
- The correct reaction to stress is to remain calm in any situation, so that later you don’t think about why your head hurts (the back of your head, the crown or your forehead).
- Moderate physical education - do not exhaust yourself with exercises, do not provoke overwork.
Treatment
Conservative therapy
Therapeutic tactics are determined taking into account the cause of the symptom. The basis is medicines, which in some cases are supplemented with non-drug methods:
- Migraine
. The attack is stopped with the help of non-narcotic analgesics and caffeine-containing drugs. Sometimes therapeutic blockades are performed. Very intense pain and prolonged attacks are indications for the use of triptans. For repeated vomiting, medications are administered subcutaneously, used in the form of sprays or rectal suppositories. - Cluster headache
. To eliminate paroxysm, triptans are prescribed, oxygen inhalations are performed, and local anesthetics are applied to the nasal mucosa. As part of prevention, calcium channel blockers are recommended; in case of intolerance, antiepileptic drugs or glucocorticosteroids are recommended. - Paroxysmal hemicrania
. The effectiveness of non-steroidal anti-inflammatory drugs, sometimes steroids, and calcium channel blockers is noted. Due to long-term use of painkillers, damage to the gastric mucosa is possible, so patients are additionally prescribed antacids and proton pump blockers. - Hypnic headache
. There is no uniform treatment regimen. It is possible to use lithium and melatonin preparations, hypnotics, benzodiazepines, NSAIDs, steroids and caffeine-containing drugs. - Vertebrobasilar system syndrome
. The treatment regimen includes medications with vascular, hypotensive and neuroprotective effects, anticoagulants, antiplatelet agents, and antidepressants. Non-drug therapy includes hyperbaric oxygenation, exercise therapy, vestibular exercises, massage, post-isometric relaxation, and magnetic laser therapy. - Arachnoiditis
. Anti-inflammatory, antiepileptic, absorbable, antiallergic and dehydration agents, metabolites, neuroprotectors, tranquilizers, and antidepressants can be prescribed. - ENT pathologies
. Antibacterial therapy, antihistamines and vasoconstrictor medications, immunocorrectors, UHF, and diadynamic currents are indicated. For sinusitis, punctures and sinus evacuation are performed; for mastoiditis, paracentesis of the tympanic membrane is performed.
Surgery
Patients with primary cephalgia do not require surgery. Surgical techniques can be used in the following cases:
- Insufficiency of vertebrobasilar blood flow
: carotid-subclavian bypass, endarterectomy. - Brain tumor
: removal of a tumor using microsurgical techniques or stereotactic radiosurgery methods, shunt operations for hydrocephalus. - Diseases of the ENT organs
: open and endoscopic maxillary sinusotomy or frontotomy, mastoidotomy, sanitizing and general cavity interventions on the middle ear. - Spinal lesions
: laser vaporization, microdiscectomy, interbody fusion, fixation with cages.
A harbinger of serious illness
Cluster cephalgia, in which the patient constantly experiences pinpoint throbbing pain in the right side of the head, may indicate the development of the following diseases and conditions:
- brain tumors of various origins;
- withdrawal state;
- aneurysms;
- hematomas due to traumatic brain injuries and concussions;
- poisoning with certain drugs;
- taking vasodilators (for example, nitroglycerin) or histamine.
Causes of neck pain on the left side
It becomes clear that the area around the neck on the left can hurt for many reasons. It is worth learning more about each disease and determining the symptoms in order to roughly understand what triggered the development of pain and discomfort in the neck.
Osteoarthrosis and osteochondrosis
Osteochondrosis manifests itself in the fact that the cartilage tissue of the spinal column gradually begins to deteriorate. The intervertebral discs become thinner, the distance between them decreases, and nerve roots are pinched. Osteoarthritis also affects the joints of the spinal column.
Neck muscle damage
One of the most common cases of neck pain is damage to muscle tissue. If you hit yourself or simply overstrain your muscles by being in a not very comfortable position for a long time, or get too cold, inflammation may begin, accompanied by pain and sometimes fever.
Complications
Most often, headaches can be controlled with the help of painkillers. But most patients again experience pain after a while, which negatively affects everyday life. In this case, only a specialist can help, who will help adjust the treatment therapy and eliminate the pain.
As a rule, there are no complications with headaches. They can become permanent, develop into a migraine, or spread to other parts of the body. To improve the prognosis, it is necessary to correctly determine the root cause and choose treatment.