Bisoprolol is an active substance that belongs to the group of selective beta1-blockers, which is part of many medications. Despite the fact that the drug was synthesized about half a century ago, it is included in the “WHO List of Essential Medicines” necessary for a basic healthcare system. Bisoprolol has been sufficiently studied: it has a hypotensive, antiarrhythmic, antianginal effect and is used to treat arterial hypertension and coronary heart disease (angina). Prescribed to patients with chronic heart failure in combination with other drugs (ACE inhibitors, diuretics, cardiac glycosides). The original drug, which contains bisoprolol, is Concor.
Bisoprolol and Concor, what is the difference?
Working as a family doctor, I am asked a huge number of questions every day. Many patients are interested in the question: what is the difference between Concor and bisoprolol? This is a really good question, but before answering it, let's first understand what the active ingredient is and what is the difference between the original and generic drug.
So, let's begin:
1. Bisoprolol is an active ingredient that is part of a huge number of drugs produced by different pharmaceutical companies under the following trade names: Bisoprolol-KV, Bisoprolol-Teva, Bisoprolol Sandoz, Bisoprolol-Ratiopharm, Bisoprolol KRKA, Biprolol, Bisostad, Euro-Bisoprolol FS Coronal, Bisoprolol fumarate, Bisocard, Bicard, Niperten, Coronal, Bisoprolol-Lugal, Bisoprolol-Prana, Concor, etc.
2. All medications are divided into original and generics.
An original drug is a completely new substance, synthesized for the first time, undergoing a full cycle of preclinical and clinical studies, a medicine protected by a patent. The creation of new drugs is a very labor-intensive, lengthy and expensive process.
A generic (reproduced medicinal product) is a medicinal product that has proven therapeutic interchangeability with the original medicinal product without a developer’s license. To create a generic, you do not need to search for a molecule or conduct a lot of research; you just need to register the drug. The quality of generics is largely determined by the quality of the substance. Since the cost of the substance is approximately half the cost of producing generics, manufacturers often purchase cheaper substances in China, India, Vietnam and other countries that are difficult to control. The quality of such substances may be low due to changes in synthesis methods to less expensive ones, which leads to the appearance of pharmacologically active or toxic impurities and degradation products.
Read our article Amelotex or Movalis, which is better
The price of the original drug may be higher due to the unique high-tech synthesis method, which minimizes the amount of impurities and by-products. In Europe, medicines undergo a large number of quality control points. The quality of the drug depends not only on the active substance, but also on excipients (excipients), as they can affect bioavailability or lead to the development of toxic or allergic reactions.
So, the difference between bisoprolol and concor is that concor is the original drug, and all other drugs that contain bisoprolol, which I wrote about above, are generics. The cost of Concor is higher than generic bisoprolol. If you compare the cheapest bisoprolol and concor, the difference in price is approximately 10 times (I compared prices in Russia and Ukraine).
Possibilities of bisoprolol in the treatment of cardiovascular diseases
In real clinical practice, beta-blockers (BABs) are one of the most widely used drugs in the treatment of cardiovascular diseases (CVD). The issues of choosing BAB still remain relevant.
As is known, beta-1-selective ABs are superior to non-selective ones: they significantly less increase peripheral vascular resistance, to a greater extent reduce the severity of the vasoconstrictor response to catecholamines and, therefore, are more effective in smokers, less likely to cause hypoglycemia in patients with diabetes mellitus (DM), less often cause withdrawal syndrome. Beta-1-selective ABs can be used in patients with obstructive pulmonary diseases; they change the lipid composition of the blood to a lesser extent.
One of the most highly cardioselective beta blockers is bisoprolol (Bidop). The affinity of bisoprolol for beta-1 adrenergic receptors is 75 times higher than for beta 2 adrenergic receptors. In a standard dose, the drug has almost no blocking effect on beta-2 adrenergic receptors and is therefore devoid of many undesirable effects. Bisoprolol in therapeutic dosages (2.5–10.0 mg/day) does not cause bronchospasm and does not impair respiratory function in people with chronic obstructive pulmonary disease (COPD). In addition, bisoprolol does not worsen renal function and intrarenal hemodynamics, does not affect carbohydrate metabolism and does not increase the content of cholesterol and lipoproteins in the blood plasma [1].
These properties determine the use of bisoprolol for various CVDs, primarily for arterial hypertension (AH) and coronary heart disease (CHD).
Benefits of bisoprolol for arterial hypertension
The main indications for the use of beta blockers in patients with hypertension are: coronary artery disease, a history of myocardial infarction, chronic heart failure (CHF), tachyarrhythmias, glaucoma [2].
In terms of antihypertensive activity, bisoprolol is not inferior to other beta blockers and is superior to them in a number of indicators. The double-blind randomized BISOMET trial showed that bisoprolol, like metoprolol, reduces blood pressure (BP) at rest, but is significantly superior to metoprolol in its effect on systolic blood pressure and heart rate (HR) during exercise [3]. The pronounced effectiveness of bisoprolol in patients leading an active lifestyle encourages the drug to be prescribed to younger patients with hypertension.
In this regard, we should recall the myths about the effect of beta-blockers on erectile function. Taking beta blockers is often associated with the possibility of sexual dysfunction. With regard to bisoprolol, the absence of a negative effect on sexual function in men has been convincingly proven. This property of bisoprolol increases adherence to treatment in young male patients who begin to suffer from hypertension in the active years of life. In a study by LM Prisant et al. demonstrated that the incidence of sexual dysfunction when taking bisoprolol did not differ from that when taking placebo [4].
When comparing bisoprolol with calcium antagonists (nifedipine) and angiotensin-converting enzyme inhibitors (ACEIs) (enalapril), it was found that it has no less antihypertensive activity. Moreover, in a comparative randomized study, bisoprolol (10–20 mg/day) led to a significant decrease in left ventricular myocardial mass index (LVMI) by 11%, which was identical to the effect of ACEI (enalapril, 20–40 mg/day) [5] .
Another study examined the effectiveness of bisoprolol in doses of 5–10 mg in patients with hypertension and left ventricular hypertrophy (LVH). After 6 months, the LVMM index significantly decreased by 14.6%, the myocardial thickness of the posterior wall of the left ventricle (LV) and interventricular septum by 8% and 9%, respectively, and the volume of cavities and LV ejection fraction did not change. At the same time, the regression of LV hypertrophy could not be explained by the hypotensive effect alone; in 5 patients who did not reach normal blood pressure values, a decrease in LVMM indices was also noted [6].
Assessment of organoprotective properties, including the effect of various antihypertensive drugs on arterial wall stiffness, is currently the subject of active study and debate. Taking into account the discovery of new markers of cardiovascular risk, we present data on the effect of bisoprolol on central pressure, pulse pressure and vascular wall stiffness. The stiffness of the vascular wall is one of the main factors determining pulse blood pressure. Both vascular wall stiffness and pulse pressure are highly correlated with endpoints such as cardiovascular mortality, myocardial infarction, and stroke. Central, or aortic, pulse pressure has an even closer relationship with cardiovascular risk [7].
Bisoprolol at a dose of 10 mg in patients with hypertension led to a significant decrease in pulse wave velocity, as well as an improvement in the elasticity of the brachial artery.
The ADLIB study examined the effects of different classes of antihypertensive drugs (amlodipine 5 mg, doxazosin 4 mg, lisinopril 10 mg, bisoprolol 5 mg and bendroflumethiazide 2.5 mg) on measures of vascular stiffness - central pressure, reflected wave and augmentation index. The most pronounced decrease in blood pressure in the brachial artery was caused by lisinopril and bisoprolol. Bisoprolol, along with lisinopril and amlodipine, reduced central blood pressure. At the same time, bisoprolol had the opposite effect on the augmentation index and reflected wave speed: the augmentation index was higher when using other drugs, and the reflected wave speed was maximum when treated with bisoprolol [8].
It is impossible not to dwell on aspects of the treatment of hypertension in obese patients. Hypertension is diagnosed in 88% of patients with abdominal obesity [9].
Despite the fact that beta blockers belong to the main class of drugs in the treatment of hypertension, obesity and metabolic syndrome are not the primary indication for their use, although the use of beta blockers in obese patients has a pathogenetic justification, given the key role of hyperactivity of the sympathetic nervous system in the development of hypertension in obesity.
The fear of prescribing beta blockers to a patient with metabolic syndrome is due to fears of worsening the course of diabetes. BAs have different prodiabetogenic potential. Thus, while taking bisoprolol and nebivolol in patients with hypertension and diabetes, there was no change in blood glucose levels, while treatment with atenolol led to a significant increase in its level. It was found that bisoprolol does not change blood glucose levels in patients with diabetes, and no dose adjustment of hypoglycemic agents is required, which indicates its metabolic neutrality [10].
Studies involving patients with diabetes, conducted with bisoprolol, have shown that, due to its high selectivity, the drug does not have a significant effect on carbohydrate and lipid metabolism and can be used in patients with diabetes.
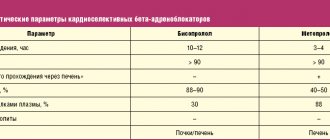
A positive property of bisoprolol for use in obese patients with hypertension is its unique ability to dissolve in both fats and water (amphiphilicity). Due to its amphiphilic properties, bisoprolol undergoes 50% biotransformation in the liver, the rest is excreted unchanged by the kidneys. Considering the frequent presence of a “compromised” liver in patients with metabolic syndrome in the form of non-alcoholic fatty liver disease, the use of bisoprolol is justified for the treatment of hypertension in this category of patients. Amphiphilicity determines the balanced clearance of bisoprolol, which explains the low likelihood of its interaction with other drugs and greater safety when used in patients with moderate hepatic or renal insufficiency [11].
Polymorbidity and the presence of both COPD and CVD in one patient forces a careful approach to the choice of beta blockers. It has been established that the administration of beta blockers to patients with COPD who have suffered a myocardial infarction reduces the risk of mortality by 40% (compared to a similar group of patients without the use of beta blockers). According to S. Chatterjece, in patients with bronchial asthma, changes in bronchial patency when taking 10 and 20 mg of bisoprolol did not differ significantly from those after placebo [12].
The cardioselective beta blocker bisoprolol in patients with CVD and concomitant COPD does not have a negative effect on bronchial patency and improves the quality of life of patients, while the less selective atenolol and metoprolol worsened airway patency in this category of patients [13].
The use of bisoprolol in various forms of ischemic heart disease
Domestic recommendations for the diagnosis and treatment of coronary artery disease [14] consider beta blockers as first-line drugs for the treatment of various forms of coronary artery disease, including serving as a necessary component in the treatment of patients with a history of myocardial infarction and CHF. It is in these clinical situations that beta blockers can improve the prognosis of patients.
Antianginal properties make it possible to prescribe bisoprolol for the prevention of anginal attacks in patients with stable angina pectoris. The multicenter clinical trial TIBBS (Total Ischemic Burden Bisoprolol Study) demonstrated that bisoprolol effectively eliminates episodes of transient myocardial ischemia in patients with stable angina and increases heart rate variability [15]. This study also showed the effect of bisoprolol on improving the prognosis of coronary artery disease. It has been proven that the incidence of cardiovascular events during bisoprolol therapy is significantly lower than when taking nifedipine and placebo.
It was also found that the antianginal effectiveness of bisoprolol is comparable to atenolol, betaxolol, verapamil and amlodipine. Other studies have shown that bisoprolol is more effective in preventing the occurrence of anginal attacks and increases exercise tolerance to a greater extent than isosorbide dinitrate (used as monotherapy) and nifedipine. In patients with stable angina, bisoprolol can be used in combination with other antianginal agents (in particular, nitrates and calcium antagonists).
It was found that bisoprolol significantly reduces the risk of myocardial infarction and mortality from CVD in patients who underwent surgery on the great arteries. As a means of secondary prevention of myocardial infarction, the use of bisoprolol in stable patients who have suffered a myocardial infarction (starting from 5–7 days of the disease) is justified [16].
Choosing bisoprolol
Considering the wide range of medicines on the Russian market and the need for an adequate choice, the problem of interchangeability of original drugs with generics for economic reasons is very relevant. The main limitation in the widespread use of original medicines is their high cost. On the other hand, the fact that the original drug is highly effective is well known. When choosing a generic, it is necessary to have data on therapeutic bioequivalence to the original drug. To prove therapeutic equivalence, a clinical study of a generic drug is required, with comparative clinical studies performed with the original drug to study its effectiveness and safety.
Let us dwell in more detail on the data from clinical studies involving Russian patients with hypertension and coronary artery disease to evaluate the effectiveness of the drug Bidop (bisoprolol).
In 2012, K.V. Protasov et al. A comparison was made of the clinical effectiveness and safety of the original and generic bisoprolol preparations for patients with hypertension and patients with exertional angina. 30 patients with grade 1–2 hypertension (average age 47 years) were examined. Patients were randomized into the original bisoprolol and Bidop groups, which were prescribed at a starting dose of 5 mg/day. After 6 weeks of treatment and a 2-week washout period, the drug was replaced with an alternative one, after which therapy was continued for up to 6 weeks. The study diagram is presented in Fig.
At baseline, on the 2nd and 6th weeks of therapy, blood pressure, heart rate, and unwanted side effects were recorded, and the results of self-monitoring of blood pressure (SBP) were analyzed. At baseline and at week 6, 24-hour blood pressure monitoring (ABPM) was performed. By the 6th week of treatment, office blood pressure significantly decreased in the original bisoprolol group by 23.0/10.5 mmHg. Art., in the generic group - by 21.2/10.0 mm Hg. Art., intergroup differences are not significant. The target blood pressure level (<140/90 mmHg) was achieved in the first group in 71.4%, in the second - in 64.3% of patients (p = 0.57). The degree of heart rate decrease also did not differ and amounted to 11.8 and 10.1 beats/min.
According to self-control and 24-hour blood pressure monitoring, unidirectional and comparable in severity shifts in mean blood pressure and heart rate were identified. Another fragment of the study, which included 18 patients with stable angina, showed that both bisoprolol drugs had similar antianginal effects, reducing signs of ischemia. It is important to note that the doses of the original and generic drugs when achieving a similar antianginal effect in the same patients did not differ, which indicates the identity of their antianginal properties.
Both drugs were well tolerated. Clinically insignificant bradycardia was recorded in only two patients treated with the original bisoprolol. This indicates that Bidop is quite well tolerated and safe [17].
According to T.K. Chernyavskaya (2012), the drug Bidop turned out to be completely therapeutically equivalent to the original bisoprolol. Thus, in the group of patients with grade 1–2 hypertension, the target blood pressure level was <140/90 mmHg. Art. reached 72% of those receiving original bisoprolol and 72.5% of those receiving Bidop. At the same time, the doses of bisoprolol required to normalize blood pressure were 9.5 mg for the original drug and 9.3 mg for Bidop. Transfer to combination treatment was required in 34% of those receiving original bisoprolol and in 33% of those receiving Bidop. No side effects occurred during 16 weeks of observation in any group of patients. With the same therapeutic efficacy, the cost of Bidop therapy was lower [18].
It can be concluded that the original bisoprolol and the drug Bidop are clinically equivalent in terms of safety, antianginal and antihypertensive effects. This allows doctors and patients to reduce the cost of treatment without reducing the effect.
Conclusion
Bisoprolol is a leader among beta blockers due to its high cardioselectivity, unique amphiphilic properties, metabolic neutrality, high efficiency and the absence of a negative effect on the course of other diseases. It is important for Russian patients to confirm the therapeutic equivalence of the original drug bisoprolol and its generic (Bidop). The antihypertensive and antianginal effectiveness of bisoprolol, reducing the cost of treatment through the use of high-quality generic drugs can significantly increase the adherence of patients with CVD to treatment.
Literature
- The Task Force on Beta-Blockers of the European Society of Cardiology. Expert consensus document on b-adrenergic receptor blockers // Eur Heart J. 2004; 25: 1341–1362.
- Russian Medical Society for Arterial Hypertension (RMAS), All-Russian Scientific Society of Cardiologists (VNOK). Diagnosis and treatment of arterial hypertension. Russian recommendations (fourth revision), 2010.
- Haasis R., Bethge H. Exercise blood pressure and heart rate reduction 24 and 3 hours after drug intake in hypertensive patients following 4 weeks of trearment with bisoprolol and metoprolol: a randomized multicentre double-blind study (BISOMET)//Eur Heart Jour. 1987; 8; 103–113.
- Prisant LM, Weir MR, Frishman WH, Neutel JM, Davidov ME, Lewin AJ Self-Reported Sexual Dysfunction in Men and Women Treated With Bisoprolol, Hydrochlorothiazide, Enalapril, Amlodipine, Placebo, or Bisoprolol/Hydrochlorothiazide // J Clin Hypertens (Greenwich). 1999, July; 1 (1): 22–26.
- Podzolkov V.I., Osadchiy K.K. Rational choice of beta-blocker for the treatment of arterial hypertension: focus on Bisogamma // Breast Cancer. 2008, vol. 16, no. 16, p. 4–8.
- Teresa E., Gonzdlez M., Camacho-Vazquez C., Tabuenca M. Effect of bisoprolol on left ventricular hypertrophy in essential hypertension // Cardiovasc. Drugs ther. 1994, 8, 837–843.
- Asmar R. Effect of antihypertensive agents on arterial stiffness as evaluated by pulse wave velocity: clinical implications // Am. J. Cardiovasc. Drugs; 2001, 1(5): 387–397.
- Leonova M.V. Beta blockers and organ protection for arterial hypertension // Clinical pharmacology and therapy. 2012, 21 (3), p. 26–30.
- Drapkina O. M., Korneeva O. N., Ivashkin V. T. Activation of the sympathetic nervous system in obesity. How to influence energy homeostasis? // Arterial hypertension. 2011, vol. 17, no. 2, p. 102–107.
- Kukes V. G., Ostroumova O. D., Baturina A. M., Zykova A. A. Beta-blockers in the treatment of arterial hypertension in patients with diabetes mellitus: contraindication or drugs of choice? // Rus. honey. magazine 2002; 10: 446–449.
- Semenov A.V., Kukes V.G. Clinical and pharmacological aspects of the use of bisoprolol // RMJ. 2007, vol. 15, no. 15, p. 38–43.
- Ostroumova O. D., Maksimov M. L. Possibilities of using highly selective beta-blockers in patients with concomitant diseases // Consilium Medicum. 2012; (4), No. 1: 721–725.
- Korneeva O. N. The place of beta-blockers in the treatment of obese patients with hypertension // Doctor. 2011, no. 11, p. 38–40.
- Diagnosis and treatment of stable angina. On Sat. "National Clinical Guidelines". MEDI Expo, 2009, p. 35–74.
- Weber F., Schneider H., von Arnim T. et al. Heart rate variability and ischaemia in patients with coronary heart disease and stable angina pectoris; influence of drug therapy and prognostic value. TIBBS Investigators Group. Total Ischemic Burden Bisoprolol Study // Eur Heart J. 1999; 20 (1): 38–50.
- Syrkin A.L., Dobrovolsky A.V. // Russian Medical Journal. 2010. No. 22. pp. 1352–1355.
- Protasov K.V., Dzizinsky A.A., Shevchenko O.P. et al. Antianginal and antihypertensive effectiveness of bisoprolol: comparison of generic Bidop with the original drug // Pharmateka. 2012, no. 17, p. 57–63.
- Chernyavskaya T.K. Fundamentals of optimal choice among interchangeable drugs in the treatment of cardiovascular diseases // Systemic hypertension. 2012, No. 1, p. 29–32.
O. N. Korneeva, Candidate of Medical Sciences
GBOU VPO First Moscow State Medical University named after. I. M. Sechenova Ministry of Health of the Russian Federation, Moscow
Contact information about the author for correspondence
Bisoprolol analogues of the drug
There are a huge number of bisprolol analogues, since the drug is included in the WHO List of Essential Medicines.
- Concor;
- Concor cor;
- Bisoprolol-KV;
- Bisoprolol-Teva;
- Bisoprolol Sandoz
- Biol Sandoz;
- Bisoprolol-Ratiopharm;
- Bisoprolol KRKA;
- Biprolol;
- Bisostad;
- Euro-Bisoprolol FS;
- Coronal;
- Bisoprolol fumarate;
- Bisocard;
- Bicard;
- Niperten;
- Coronal;
- Bisoprolol-Lugal;
- Bisoprolol-Prana;
- Bisoprolol - BORIMED;
- Bisoprolol - MAKSPHARMA;
- Bisoprolol - MIC;
- Cordinorm;
- Cordinorm Cor.
This list can be continued almost indefinitely)))), so here I have given analogues registered in Russia, Ukraine and Belarus.
Are there any disadvantages to any of the drugs and what are they?
The selection of an effective remedy for the management of patients with coronary artery disease or arterial hypertension is carried out by the attending physician, taking into account the individual characteristics of the patient: age, gender, and the presence of concomitant diseases.
The pleiotropic effect of the drug (directed at different stages of pathogenesis) causes a wide list of contraindications and restrictions for use.
Conditions in which the use of drugs with bisoprolol is not recommended:
- hypertensive crisis - the active substance of the medication is aimed at controlling the course of the pathology, and not relieving acute conditions;
- dilated cardiomyopathy - a decrease in cardiac output worsens the condition of such patients;
- conduction disturbance in the atrioventricular node (blockade): additional slowing of the rhythm contributes to the development of the Morgagni-Adams-Stokes symptom with loss of consciousness and convulsions;
- bronchial asthma – the influence of bisoprolol on bronchial smooth muscle in compromised patients at risk of developing obstruction cannot be excluded;
- uncompensated uncontrolled diabetes mellitus type 2;
- stenosis of the aortic mouth (grade 3 or higher) – decreased force of myocardial contraction, decreased release and delivery of blood to organs and tissues;
- during pregnancy and breastfeeding - active metabolites penetrate the hematoplacental barrier and slow down the baby’s heart rate.
The disadvantages of the drugs "Concor" and "Bisoprolol" are associated with the long course of the underlying disease and a wide range of effects:
- selection of an effective dose lasts 1-2 weeks;
- drug treatment – daily, lifelong;
- contraindicated in patients with concomitant somatic pathologies;
- side effects: bradycardia, drop in blood pressure, dizziness, spots before the eyes, nausea, abdominal pain.
Patients intolerant to Bisoprolol are not recommended to use Concor as a substitute due to its similar composition and pharmacological effects.