BISOPROLOL-PRANA
Interaction
Not recommended combinations:
Class I antiarrhythmic drugs
(for example, quinidine, disopyramide, lidocaine, phenytoin, flecainide, propafenone) when used simultaneously with bisoprolol can reduce AV conduction and cardiac contractility.
Blockers of “slow” calcium channels (SCBC) (verapamil, diltiazem),
when used simultaneously with bisoprolol, they can lead to a decrease in myocardial contractility and impaired AV conduction. In particular, intravenous administration of verapamil to patients taking β-blockers can lead to severe arterial hypotension and AV block.
Centrally acting antihypertensives
(such as clonidine, methyldopa, moxonidine, rilmenidine) can lead to a decrease in heart rate and cardiac output, as well as vasodilation due to a decrease in central sympathetic tone. Abrupt withdrawal, especially before discontinuation of beta-blockers, may increase the risk of rebound hypertension.
Combinations requiring special caution:
BKMK, dihydropyridine derivatives (for example nifedipine, felodipine, amlodipine),
when used simultaneously with bisoprolol, they may increase the risk of developing arterial hypotension. In patients with CHF, the risk of subsequent deterioration in cardiac contractility cannot be excluded.
Class III antiarrhythmic drugs
(eg amiodarone) may increase AV conduction disturbances.
Action of β-blockers for local use
(for example, eye drops for the treatment of glaucoma) may enhance the systemic effects of bisoprolol (lowering blood pressure, lowering heart rate).
Allergens used for immunotherapy or allergen extracts
skin tests increase the risk of severe systemic allergic reactions or anaphylaxis in patients receiving bisoprolol.
Iodine-containing radiocontrast agents
for intravenous administration increase the risk of anaphylactic reactions.
Changes the effectiveness of insulin and oral hypoglycemic agents,
masks the symptoms of developing hypoglycemia (tachycardia, increased blood pressure).
The antihypertensive effect is weakened by non-steroidal anti-inflammatory drugs
(NSAIDs) (retention of sodium ions (Na) and blockade of prostaglandin synthesis by the kidneys), glucocorticosteroids and estrogens (retention of Na+ ions).
Prolongs the effect of non-depolarizing muscle relaxants
and increases the anticoagulant effect
of coumarins.
Tri- and tetracyclic antidepressants, antipsychotics (neuroleptics), ethanol, sedatives and hypnotics
increase depression of the central nervous system.
MAO inhibitors (except MAO B inhibitors)
may enhance the antihypertensive effect of beta-blockers. Concomitant use may also lead to the development of a hypertensive crisis. The treatment break between taking MAO inhibitors and bisoprolol should be at least 14 days.
Non-hydrogenated ergot alkaloids
increase the risk of developing peripheral circulatory disorders.
Ergotamine
increases the risk of developing peripheral circulatory disorders;
sulfasalazine
increases the concentration of bisoprolol in the blood plasma;
Rifampicin
reduces T1/2.
Mefloquine
when used simultaneously with bisoprolol, it may increase the risk of bradycardia.
Parasympathomimetics
when used simultaneously with bisoprolol, they may increase AV conduction disturbances and increase the risk of developing bradycardia.
Means for general anesthesia
may increase the risk of cardiodepressive effects, leading to arterial hypotension.
Cardiac glycosides
when used simultaneously with bisoprolol, they can lead to an increase in impulse conduction time, and thus to the development of bradycardia.
Simultaneous use of the drug with beta-agonists
(eg,
isoprenaline, dobutamine)
may reduce the effect of both drugs.
Combination of bisoprolol with adrenergic agonists
affecting alpha- and beta-adrenergic receptors
(for example,
norepinephrine, epinephrine)
may enhance the vasoconstrictor effects of these drugs that occur with the participation of alpha-adrenergic receptors, leading to an increase in blood pressure
. Such interactions are more likely when using non-selective beta-blockers.
Bisoprolol-Prana, 30 pcs., 10 mg, film-coated tablets
Monitoring of patients taking the drug BISOPROLOL-PRANA should include measuring heart rate and blood pressure (at the beginning of treatment - daily, then - once every 3-4 months), conducting an ECG, determining the concentration of glucose in the blood in patients with diabetes mellitus (once every 4 months). -5 months). In elderly patients, it is recommended to monitor renal function (once every 4–5 months).
The patient should be taught how to calculate heart rate and instructed about the need for medical consultation if the heart rate is less than 50 beats/min.
Before starting treatment, it is recommended to conduct a study of external respiratory function in patients with a burdened bronchopulmonary history.
In approximately 20% of patients with angina, β-blockers are ineffective. The main reasons: severe coronary atherosclerosis with a low ischemic threshold (heart rate less than 100 beats/min) and increased end-diastolic volume of the left ventricle, disrupting subendocardial blood flow.
In smokers, the effectiveness of β-blockers is lower.
Patients using contact lenses should take into account that during treatment the production of tear fluid may decrease.
When used in patients with pheochromocytoma, there is a risk of developing paradoxical arterial hypertension (if effective α-blockade is not previously achieved).
In thyrotoxicosis, bisoprolol may mask certain clinical signs of thyrotoxicosis (for example, tachycardia). Abrupt withdrawal in patients with thyrotoxicosis is contraindicated because it can increase symptoms.
In diabetes mellitus, it can mask tachycardia caused by hypoglycemia. Unlike non-selective beta-blockers, it practically does not enhance insulin-induced hypoglycemia and does not delay the restoration of blood glucose concentrations to normal levels.
When taking clonidine at the same time, it can be discontinued only a few days after discontinuation of the drug BISOPROLOL-PRANA.
It is possible that the severity of the hypersensitivity reaction may increase and there will be no effect from usual doses of epinephrine against the background of a burdened allergic history.
If planned surgical treatment is necessary, the drug should be discontinued 48 hours before the start of general anesthesia. If the patient took the drug before surgery, he should choose a drug for general anesthesia with minimal negative inotropic effect.
Reciprocal activation of the vagus nerve can be reversed by intravenous atropine (1–2 mg).
Medicines that reduce the supply of catecholamines (including reserpine) can enhance the effect of beta-blockers, so patients taking such combinations of drugs should be under constant medical supervision to detect a pronounced decrease in blood pressure or bradycardia.
Patients with bronchospastic diseases can be prescribed cardioselective β-blockers in case of intolerance and/or ineffectiveness of other antihypertensive drugs. Overdose is dangerous for the development of bronchospasm.
If increasing bradycardia (less than 50 beats/min), a pronounced decrease in blood pressure (systolic blood pressure below 100 mm Hg), or AV blockade is detected in elderly patients, it is necessary to reduce the dose or stop treatment.
It is recommended to discontinue therapy if depression develops.
Treatment should not be abruptly interrupted due to the risk of developing withdrawal syndrome (severe arrhythmias and myocardial infarction). Cancellation is carried out gradually, reducing the dose over 2 weeks or more (reduce the dose by 25% in 3-4 days). It should be discontinued before testing the content of catecholamines, normetanephrine and vanillylmandelic acid in the blood and urine, and titers of antinuclear antibodies.
Effect on the ability to drive a car and other mechanical means
The question of the possibility of engaging in potentially hazardous activities that require increased attention and speed of psychomotor reactions should be decided only after assessing the patient’s individual response to the drug (especially at the beginning of treatment, due to the possibility of developing dizziness).
Products
Composition: 1 tablet (10 mg) contains: active substance: bisoprolol hemifumarate (fumarate) 10 mg, excipients: corn starch, microcrystalline cellulose, magnesium stearate, crospovidone, colloidal silicon dioxide, anhydrous calcium hydrogen phosphate.
Shell composition
Macrogol-400, titanium dioxide, dimethicone 100, yellow iron oxide;
Description
Round, biconvex, film-coated tablets with a score. Tablets with a dosage of 5 mg are light yellow, tablets with a dosage of 10 mg are light orange. On a cross section, two layers are visible, the inner layer is white or almost white.
Pharmacotherapeutic group
β1-adrenergic blocker selective. ATX CODE C07AB07.
Pharmacodynamics
A selective β1-adrenergic blocker, without its own sympathomimetic activity, does not have a membrane-stabilizing effect. Reduces plasma renin activity, reduces myocardial oxygen demand, and reduces heart rate (heart rate) (at rest and during exercise). It has hypotensive, antiarrhythmic and antianginal effects. By blocking β1-adrenergic receptors of the heart in low doses, it reduces the catecholamine-stimulated formation of cyclic adenosine monophosphate (cAMP) from adenosine triphosphate (ATP), reduces the intracellular current of calcium ions (Ca2+), has a negative chrono-, dromo-, bathmo- and inotropic effect, reduces atrioventricular conductivity and excitability. When the therapeutic dose is exceeded, it has a β2-adrenergic blocking effect. The total peripheral vascular resistance at the beginning of the use of the drug, in the first 24 hours, increases (as a result of a reciprocal increase in the activity of α-adrenergic receptors and the elimination of stimulation of β2-adrenergic receptors), after 1-3 days it returns to the original level, and with long-term use it decreases. The hypotensive effect is associated with a decrease in minute blood volume, sympathetic stimulation of peripheral vessels, restoration of sensitivity in response to a decrease in blood pressure (BP) and an effect on the central nervous system (CNS). In case of arterial hypertension, the effect occurs after 2-5 days, a stable effect is observed after 1-2 months. The antianginal effect is due to a decrease in myocardial oxygen demand as a result of a decrease in heart rate (HR) and a decrease in myocardial contractility, prolongation of diastole, and improved myocardial perfusion. Due to an increase in end-diastolic pressure in the left ventricle and an increase in the stretch of ventricular muscle fibers, oxygen demand may increase, especially in patients with chronic heart failure (CHF). When used in average therapeutic doses, in contrast to non-selective β-blockers, it has a less pronounced effect on organs containing β2-adrenergic receptors (pancreas, skeletal muscles, smooth muscles of peripheral arteries, bronchi and uterus) and on carbohydrate metabolism; does not cause retention of sodium ions (Na+) in the body; the severity of the atherogenic effect does not differ from the effect of propranolol.
Pharmacokinetics
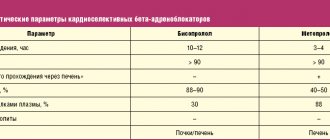
Absorption – 80-90%, food intake does not affect absorption. The maximum concentration in blood plasma is observed after 1-3 hours, the connection with blood plasma proteins is about 30%. Permeability through the blood-brain barrier and placental barrier is low. 50% of the dose is metabolized in the liver with the formation of inactive metabolites, half-life (T1/2) 10-12 hours. About 98% is excreted by the kidneys, of which 50% is excreted unchanged; less than 2% - through the intestines with bile.
Indications for use
arterial hypertension; coronary heart disease: prevention of angina attacks.
Contraindications
Hypersensitivity to the components of the drug and other β-blockers, shock (including cardiogenic), collapse, pulmonary edema, acute heart failure, chronic heart failure in the stage of decompensation, atrioventricular (AV) block II-III degree, sinoatrial block, weakness syndrome sinus node, severe bradycardia, Prinzmetal's angina, cardiomegaly (without signs of heart failure), arterial hypotension (systolic blood pressure less than 100 mm Hg, especially with myocardial infarction); severe forms of bronchial asthma and chronic obstructive pulmonary disease (COPD) in history; simultaneous use of monoamine oxidase inhibitors (MAO) (with the exception of MAO-B), late stages of peripheral circulatory disorders, Raynaud's disease, pheochromocytoma (without simultaneous use of α-blockers), metabolic acidosis, age under 18 years (efficacy and safety have not been established). With caution: liver failure, chronic renal failure, myasthenia gravis, thyrotoxicosis, diabetes mellitus, first degree AV block, depression (including a history), psoriasis, allergic reactions (history), old age.
Use during pregnancy and lactation
Use during pregnancy is possible if the benefit to the mother outweighs the risk of side effects in the fetus and child. There is no data on the excretion of bisoprolol into breast milk. Therefore, if it is necessary to use the drug BISOPROLOL-PRANA during lactation, breastfeeding must be stopped.
Directions for use and doses
Inside, in the morning on an empty stomach, without chewing, once. Arterial hypertension and coronary heart disease: prevention of angina attacks: It is recommended to take 5 mg once. If necessary, the dose is increased to 10 mg 1 time per day. The maximum daily dose is 20 mg. In all cases, the dosage regimen and dosage are selected by the doctor individually for each patient, in particular, taking into account heart rate values and therapeutic response. In patients with impaired renal function with creatinine clearance (CC) less than 20 ml/min, or with severe liver dysfunction, the maximum daily dose is 10 mg. No dose adjustment is required in elderly patients.
Side effect
From the central and peripheral nervous system: increased fatigue, weakness, dizziness, headache, sleep disorders, depression, anxiety, confusion or short-term memory loss, hallucinations, asthenia, myasthenia, paresthesia in the extremities (in patients with intermittent claudication and Raynaud's syndrome), tremors, cramps (including calf muscles).
From the organ of vision: blurred vision, decreased secretion of tear fluid, dryness and soreness of the eyes, conjunctivitis.
From the cardiovascular system: sinus bradycardia, palpitations, myocardial conduction disturbances, AV block (up to the development of complete transverse block and cardiac arrest), arrhythmias, weakening of myocardial contractility, development (worsening) of CHF (swelling of the ankles, feet; shortness of breath), decreased blood pressure, orthostatic hypotension, manifestation of vasospasm (increased peripheral circulatory disorders, coldness of the lower extremities, Raynaud's syndrome), chest pain.
From the digestive system: dryness of the oral mucosa, nausea, vomiting, abdominal pain, constipation or diarrhea, liver dysfunction (dark urine, yellowness of the sclera or skin, cholestasis), changes in taste.
From the respiratory system: nasal congestion, difficulty breathing when prescribed in high doses (loss of selectivity) and/or in predisposed patients - laryngo- and bronchospasm.
From the endocrine system: hyperglycemia (in patients with non-insulin-dependent diabetes), hypoglycemia (in patients receiving insulin), hypothyroidism.
Allergic reactions: skin itching, rash, urticaria.
From the skin: increased sweating, skin hyperemia, exanthema, psoriasis-like skin reactions, exacerbation of psoriasis symptoms, alopecia.
Laboratory indicators: thrombocytopenia (unusual bleeding and hemorrhage), agranulocytosis, leukopenia, changes in the activity of liver enzymes (increased alanine aminotransferase (ALT), aspartate aminotransferase (AST), bilirubin levels, triglycerides.
Effect on the fetus: intrauterine growth retardation, hypoglycemia, bradycardia.
Other: back pain, arthralgia, weakened libido, decreased potency, withdrawal syndrome (increased angina attacks, increased blood pressure).
Overdose
Symptoms: arrhythmia, ventricular extrasystole, severe bradycardia, AV block, marked decrease in blood pressure, chronic heart failure, cyanosis of fingernails or palms, difficulty breathing, bronchospasm, dizziness, fainting, convulsions.
Treatment: gastric lavage and administration of adsorbents; symptomatic therapy: in case of developed AV block - intravenous administration of 1-2 mg of atropine, epinephrine or temporary placement of a pacemaker; for ventricular extrasystole - lidocaine (class IA drugs are not used); when blood pressure decreases, the patient should be in the Trendelenburg position; if there are no signs of pulmonary edema, intravenous administration of plasma-substituting solutions; if ineffective, administration of epinephrine, dopamine, dobutamine (to maintain chronotropic and inotropic effects and eliminate a pronounced decrease in blood pressure); for heart failure - cardiac glycosides, diuretics, glucagon; for convulsions - intravenous diazepam; for bronchospasm - β2-adrenergic stimulants by inhalation.
Interaction with other drugs
Allergens used for immunotherapy or allergen extracts for skin testing increase the risk of severe systemic allergic reactions or anaphylaxis in patients receiving bisoprolol.
Iodine-containing radiocontrast agents for intravenous administration increase the risk of anaphylactic reactions.
Phenytoin, when administered intravenously, and agents for inhalation anesthesia (hydrocarbon derivatives) increase the severity of the cardiodepressive effect and the likelihood of lowering blood pressure.
Changes the effectiveness of insulin and hypoglycemic agents for oral administration, masks the symptoms of developing hypoglycemia (tachycardia, increased blood pressure).
Reduces the clearance of lidocaine and xanthines (except theophylline) and increases their concentration in the blood plasma, especially in patients with initially increased clearance of theophylline under the influence of smoking.
The hypotensive effect is weakened by nonsteroidal anti-inflammatory drugs (NSAIDs) (retention of sodium ions (Na+) and blockade of prostaglandin synthesis by the kidneys), glucocorticosteroids and estrogens (retention of Na+ ions).
Cardiac glycosides, methyldopa, reserpine and guanfacine, blockers of “slow” calcium channels (verapamil, diltiazem), amiodarone and other antiarrhythmic drugs increase the risk of developing or worsening bradycardia, AV block, cardiac arrest and heart failure. Nifedipine can lead to a significant decrease in blood pressure.
Diuretics, clonidine, sympatholytics, hydralazine and other antihypertensive drugs can lead to an excessive decrease in blood pressure.
Prolongs the effect of non-depolarizing muscle relaxants and increases the anticoagulant effect of coumarins.
Tri- and tetracyclic antidepressants, antipsychotics (neuroleptics), ethanol, sedatives and hypnotics increase CNS depression.
Concomitant use with MAO inhibitors is not recommended, due to a significant increase in the hypotensive effect; the break in treatment between taking MAO inhibitors and bisoprolol should be at least 14 days. Non-hydrogenated ergot alkaloids increase the risk of developing peripheral circulatory disorders.
Ergotamine increases the risk of developing peripheral circulatory disorders; sulfasalazine increases the concentration of bisoprolol in the blood plasma; Rifampicin reduces T1/2.
special instructions
Monitoring of patients taking the drug BISOPROLOL-PRANA should include measuring heart rate and blood pressure (at the beginning of treatment - daily, then once every 3-4 months), conducting an ECG, determining the concentration of glucose in the blood in patients with diabetes mellitus (once every 4 months). -5 months). In elderly patients, it is recommended to monitor kidney function (once every 4-5 months). The patient should be taught how to calculate heart rate and instructed about the need for medical consultation if the heart rate is less than 50 beats/min. Before starting treatment, it is recommended to conduct a study of external respiratory function in patients with a burdened bronchopulmonary history. In approximately 20% of patients with angina, β-blockers are ineffective. The main reasons: severe coronary atherosclerosis with a low ischemic threshold (heart rate less than 100 beats/min) and increased end-diastolic volume of the left ventricle, disrupting subendocardial blood flow. In smokers, the effectiveness of β-blockers is lower. Patients using contact lenses should take into account that during treatment the production of tear fluid may decrease. When used in patients with pheochromocytoma, there is a risk of developing paradoxical arterial hypertension (if effective α-blockade is not previously achieved). In thyrotoxicosis, bisoprolol may mask certain clinical signs of thyrotoxicosis (for example, tachycardia). Abrupt withdrawal in patients with thyrotoxicosis is contraindicated because it can increase symptoms. In diabetes mellitus, it can mask tachycardia caused by hypoglycemia. Unlike non-selective beta-blockers, it practically does not enhance insulin-induced hypoglycemia and does not delay the restoration of blood glucose concentrations to normal levels. When taking clonidine at the same time, it can be discontinued only a few days after discontinuation of the drug BISOPROLOL-PRANA. It is possible that the severity of the hypersensitivity reaction may increase and there will be no effect from usual doses of epinephrine against the background of a burdened allergic history. If planned surgical treatment is necessary, the drug should be discontinued 48 hours before the start of general anesthesia. If the patient took the drug before surgery, he should choose a drug for general anesthesia with minimal negative inotropic effect. Reciprocal activation of the vagus nerve can be eliminated by intravenous atropine (1-2 mg). Medicines that reduce the supply of catecholamines (including reserpine) can enhance the effect of beta-blockers, so patients taking such combinations of drugs should be under constant medical supervision to detect a pronounced decrease in blood pressure or bradycardia. Patients with bronchospastic diseases can be prescribed cardioselective β-blockers in case of intolerance and/or ineffectiveness of other antihypertensive drugs. An overdose is dangerous due to the development of bronchospasm. If increasing bradycardia (less than 50 beats/min), a pronounced decrease in blood pressure (systolic blood pressure below 100 mm Hg), or AV blockade is detected in elderly patients, it is necessary to reduce the dose or stop treatment. It is recommended to discontinue therapy if depression develops. Treatment should not be abruptly interrupted due to the risk of developing withdrawal syndrome (severe arrhythmias and myocardial infarction). Cancellation is carried out gradually, reducing the dose over 2 weeks or more (reduce the dose by 25% in 3-4 days). It should be discontinued before testing the content of catecholamines, normetanephrine and vanillinmandelic acid in the blood and urine, and titers of antinuclear antibodies. Impact on the ability to drive a car and other mechanical means: the question of the possibility of engaging in potentially hazardous activities that require increased attention and speed of psychomotor reactions should be decided only after assessing the patient’s individual response to the drug (especially at the beginning of treatment, due to the possibility of developing dizziness) .
special instructions
Film-coated tablets, 5 and 10 mg. 10 tablets per blister pack. 50, 60, 70, 80, 90, 100 tablets in a polymer jar. Each can or 1, 2, 3, 4 blisters along with instructions for use are placed in a cardboard pack.
Storage conditions
Store in a dry place, protected from light, at a temperature not exceeding 25 °C. Keep out of the reach of children.
Best before date
3 years. Do not use after the expiration date stated on the package.