Life is a continuous process of exchange, transformation of substances and energy. A variety of pathological factors can disrupt this process, which is accompanied by disorders of the organs and systems of the body. The disease develops. If in these cases the body’s compensatory reactions are exhausted or do not have time to react, a threat to its vital functions arises (terminal state).
- Terminal states
- Stages and stages of resuscitation
- Treatment after resuscitation
Terminal states
With the help of intensive therapy and the use of resuscitation measures, in many cases it is possible to prevent and eliminate the energy and structural deficit that develops in the body during terminal conditions, and save it from death.
Intensive therapy is a set of methods for temporary artificial replacement of vital body functions, aimed at preventing the depletion of adaptive mechanisms and the occurrence of a terminal condition.
Reanimatology is the science of reviving the body; prevention and treatment of terminal conditions (according to V.A. Negovsky).
For human life to exist, it is necessary that oxygen continuously enters and is consumed by cells and carbon dioxide is released from it. These processes ensure the coordinated functioning of the respiratory and circulatory organs under the control of the central nervous system. Therefore, their defeat leads to death (“the gates of death” - as defined by the ancients - the lungs, heart and brain).
Stopping vital activity (death) can occur suddenly (in accidents) or predictably, as a natural consequence of old age or an incurable disease. During a long process of dying, the following stages are noted.
Peredagonia . The physiological mechanisms of the body’s vital functions are in a state of deep exhaustion:
- the central nervous system is depressed, possibly comatose;
- heart activity is weakened, the pulse is thready, systolic blood pressure is reduced to a more critical level (70 mm Hg);
- external breathing is weakened, ineffective: tidal volume and frequency are inadequate;
- the functions of parenchymal organs are impaired.
Peredagonia can take several minutes, hours, or even days. During this time, the patient's condition worsens even more and ends with a terminal pause. The patient loses consciousness, blood pressure and pulse are not determined; breathing stops, reflexes are absent. The terminal pause lasts up to a minute.
The next stage of dying is agony (struggle). Due to the depletion of higher-order vital activity centers (CNS), the bulbar centers and reticular formation go out of control (activate). The patient's muscle tone and reflexes are restored, external breathing appears (random, with the participation of auxiliary muscles). The pulse is palpated above the main arteries, vascular tone can be restored - systolic blood pressure increases to 50 - 70 mm Hg. However, at this time, metabolic disorders in the body's cells become irreversible. The last reserves of energy accumulated in high-energy connections quickly burn out and after 20 - 40 seconds clinical death occurs.
In a number of pathological situations (drowning, electric shock and lightning, being hit by a car, strangulation asphyxia, myocardial infarction, etc.), clinical death can befall the victim unexpectedly, without preliminary manifestations of dying.
The main signs of clinical death:
- absence of pulsation over the main arteries (carotid and femoral);
- persistent pupil dilation with absence of photoreaction;
- lack of spontaneous breathing.
Auxiliary signs:
- change in skin color (dead gray or bluish);
- lack of consciousness;
- lack of reflexes and loss of muscle tone.
An important factor influencing the effectiveness of resuscitation in case of clinical death is the ambient temperature and the duration of dying. In case of sudden cardiac arrest, clinical death in conditions of normothermia lasts up to 5 minutes, at sub-zero temperatures - up to 10 minutes or more. A long period of dying significantly worsens the effectiveness of resuscitation, reducing the period of clinical death. Biological death occurs when, as a result of irreversible changes in the body, and above all, in the central nervous system, a return to life is impossible.
Stages and stages of resuscitation
A set of emergency measures carried out to patients in a state of clinical death, aimed at restoring the body’s vital functions and preventing irreversible damage to its organs and systems, is called resuscitation. The person who revives the victim is called a resuscitator.
Returning a patient to a full life from a state of clinical death is possible only with a qualified and consistent implementation of a complex of resuscitation measures.
The first stage of resuscitation is the provision of first aid (basic life support) carried out by a resuscitator (not necessarily a medical worker, but every trained person who has basic resuscitation skills). After clinical death is declared (which should take no more than 7-8 seconds!), preparatory measures are immediately carried out: the victim is laid on his back, preferably with the upper part of his body lowered, on a solid base. A savior who is not involved in intensive care lifts the victim’s legs 50–60 cm upward to drain blood from them and increase blood supply to the cavities of the heart.
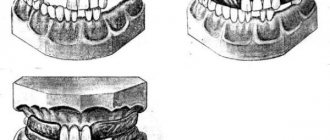
The first stage of resuscitation is to ensure airway patency. The resuscitator performs a “triple technique” (according to P. Safar):
a) opens the victim’s mouth and with a finger wrapped in a handkerchief (gauze cloth for clamps) frees him from foreign bodies and liquids (vomit, sputum, algae, inserted crevices, blood clots, etc.);
b) tilts the victim’s head as far back as possible, placing an improvised cushion under the neck (for example, the forearms). In this case, in most victims, the upper respiratory tract is freed from the tongue and its root, becoming open;
c) brings the lower jaw forward. The patency of the upper respiratory tract is restored in other cases.
The second stage of resuscitation is performing mouth-to-mouth artificial ventilation. Having covered the victim's mouth with a bandage (handkerchief), the resuscitator tightly covers his mouth with his lips and exhales. Mandatory condition: the victim's head is tilted back, his nostrils are pinched with the thumb and forefinger (so that the air does not return back), the exhalation volume for adults should be 800 - 1000 ml. When blowing air, the resuscitator, out of the corner of his eye, watches the movements of the victim’s chest, which should rise and fall. Having made 2 - 3 exhalations, the savior begins to carry out the next stage of resuscitation.
The third stage of resuscitation is closed cardiac massage. Being on the side of the victim, the resuscitator places one hand on the lower third of the sternum, strictly in the middle, so that the fingers are raised up and placed parallel to the ribs. He places the second hand on top and, pressing rhythmically, moves the sternum in the sagittal direction to a depth of 3 - 5 cm. The frequency of pressing is 60 per minute.
Mandatory condition: when pressing on the sternum, the fingers of the hand should be raised up to prevent fractures of the ribs, and the arms should be straightened at the elbow joints. Cardiac massage is thus carried out by the mass of the resuscitator’s torso. Subsequently, the rescuer alternately injects air and presses on the sternum in a ratio of 1: 4. If there are two resuscitators, each of them performs its own stage of resuscitation. If necessary, each time remove the lower jaw to ensure patency, breathe in the 2nd and 3rd stages in a ratio of 2: 10.
Signs of effective resuscitation measures :
- constriction of the pupils,
- normalization of skin color,
- feeling under the fingers of arterial pulsation, synchronous with the massage;
- Sometimes blood pressure is determined.
In some cases, cardiac activity may be restored. The first stage of resuscitation should be carried out continuously until the arrival of a specialized medical team.
The second stage of cardiopulmonary resuscitation is the provision of specialized medical care (further life support). It is carried out by professional doctors using monitoring, diagnostic, therapeutic equipment and medications. Under the control of a laryngoscope, a portable or electric suction is used to better clean the airways and intubate the trachea.
The resuscitation team provides more effective artificial ventilation of the lungs - with a manual portable or stationary ventilator through a mask, air duct or endotracheal tube with an air-oxygen mixture. If you have a special massager, you can perform closed cardiac massage using hardware.
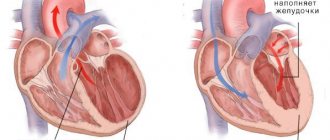
At this stage, the following stages of resuscitation are carried out alternately. The first stage is drug therapy. For all types of circulatory arrest, solutions of adrenaline hydrochloride (1 ml of 0.1% solution) and atropine sulfate (3 ml of 0.1% solution) are used. The second stage is assessing the type of circulatory arrest. For adequate drug therapy, it is necessary to diagnose the functional state of the victim’s heart. To do this, the patient is connected to an electrocardiograph (cardioscope) in the second lead and the curve is recorded.
There are the following types of circulatory arrest : asystole, fibrillation, “ineffective heart”.
- During asystole, the electrocardiograph records a straight line.
- Ventricular fibrillation is manifested by frequent chaotic contraction of individual myocardial fibers (uneven “teeth” of high, medium and variable amplitude).
- “Ineffective heart” - registration of the ventricular complex on the ECG in patients with absent pumping function of the heart.
Ventricular fibrillation and an “ineffective heart” without appropriate correction, as the energy resources of the myocardium decrease, quickly turn into asystole. In the presence of high-wave fibrillation, you can use a 2% lidocaine solution (0.5 mg per 1 kg of body weight, repeatedly).
In case of an “ineffective heart” caused by a sharp decrease in the volume of circulating blood, to ensure its pumping function, hemodynamic media (refortan, stabizol, polyglucin, rheopolyglucin), crystalloids, and glucocorticoids are infused intravenously or intraarterially; in case of massive blood loss - canned blood and its components.
In case of cardiac arrest caused by hyperkalemia or hypocalcemia (acute and chronic renal failure, hemolysis of red blood cells, massive tissue destruction, hypoparathyroidism), calcium chloride should be used (5 - 10 ml of 10% solution, intravenously). Medicinal media are administered intravenously, into the lumen of the trachea, through a cannulated artery, intracardiacly.
Medians administered intravenously, with effective cardiac massage, enter the coronary vessels, exerting their influence on the heart. If it is impossible to provide venous access, the intratracheal method is used, which is no less effective. In this case, with a needle for intramuscular injections, the cricothyroid ligament or the space between the tracheal rings is pierced and solutions of adrenaline, atropine or lidocaine are injected (2-3 ml of 0.1% solution of adrenaline hydrochloride, 1 ml of 0.1% solution of atropine sulfate, 2 ml of 2% lidocaine solution - diluting them in 10 ml of sodium chloride solution). These medications can also be given through an endotracheal tube. During ventilation of the lungs at this time, medicinal media penetrate through the alveoli, and after 30-40 seconds enter the lumen of the coronary vessels.
According to some researchers, using distilled water as a solvent can achieve effective absorption of the solution from the alveoli into the blood due to the difference in osmotic pressure. Due to the large number of complications, intracardiac administration of drugs is used less and less (the technique is described below).
The intra-arterial method of infusion in patients with a significant loss of circulating blood volume (for example, with hemorrhagic shock and an “ineffective heart”) also deserves attention Infusion of blood and other agents into a catheterized artery (eg, radial) is often effective in filling the coronary arteries with blood, ensuring efficient cardiac function and restoring hemodynamics.
The third stage is electrical defibrillation of the heart. It is used in patients with ventricular fibrillation (the method is described below). In an operating room, it is sometimes more effective to perform open cardiac massage. Indications: cardiac arrest during surgery on the organs of the chest and upper abdomen; cardiac tamponade; bilateral pneumothorax; multiple fenestrated rib fractures; congenital and acquired deformities of the chest, which make it impossible to conduct effective closed massage. Open massage is carried out through transthoracic or subdiaphragmatic access, without opening or with opening of the cardiac membrane.
A prerequisite for this is that the fingers of one or both hands, when squeezing the ventricles, should be placed along the vascular bundle so as not to pinch it. The third stage of cardiopulmonary resuscitation.
Fundamentals of resuscitation techniques
The success of resuscitation largely depends on the time elapsed from the moment of circulatory arrest to the start of resuscitation.
The basis of measures to increase the survival rate of patients with circulatory and respiratory arrest is the concept of the “chain of survival”. It consists of a number of stages: at the scene, during transport, in the hospital operating room, in the intensive care unit and in the rehabilitation center. The weakest link in this chain is the effective provision of basic living standards at the scene. The outcome largely depends on it. It should be remembered that the time during which you can count on successful restoration of cardiac activity is limited. Resuscitation under normal conditions can be successful if started immediately or in the first minutes after the onset of circulatory arrest. The basic principle of resuscitation at all stages of its implementation is the provision that “resuscitation should prolong life, and not prolong death.” The final results of resuscitation largely depend on the quality of resuscitation. Errors in its implementation can subsequently be layered on the primary damage that caused the terminal condition.
The indication for resuscitation measures is a state of clinical death. Among the main causes of clinical death requiring resuscitation, the leading ones are: sudden circulatory arrest, airway obstruction, hypoventilation, apnea, blood loss and brain damage. Clinical death is the period between life and death, when there are no visible signs of life, but life processes are still ongoing, making it possible to revive the body. The duration of this period at normal body temperature is 5–6 minutes, after which irreversible changes develop in the tissues of the body. Under special conditions (hypothermia, pharmacological protection), this period is extended to 15-16 minutes.
Signs of clinical death are:
1. Arrest of blood circulation (lack of pulsation in the main arteries);
2. Lack of spontaneous breathing (no chest excursions);
3. Lack of consciousness;
4. Wide pupils;
5. Areflexia (no corneal reflex and pupillary reaction to light):
6. Appearance of the corpse (pallor, acrocyanosis).
When carrying out resuscitation, there are 3 stages and 9 stages. The symbolic abbreviation of resuscitation measures - the first letters of the English alphabet - emphasizes the fundamental importance of methodical and consistent implementation of all stages.
Stage I - basic life support. Consists of three stages:
A (airway open) - restoration of airway patency;
B (breath for victim) - emergency artificial ventilation and oxygenation;
C (circulation his blood) - maintaining blood circulation.
Stage II - further life support. It consists of restoring independent blood circulation, normalizing and stabilizing blood circulation and breathing parameters. Stage II includes three stages:
D (drug) - medications and infusion therapy;
E (ECG) - electrocardioscopy and cardiography;
F (fibrillation) - defibrillation.
Stage III - long-term maintenance of life in the post-resuscitation period. It consists of post-resuscitation intensive care and includes the stages:
G (gauging) - state assessment;
H (human mentality) restoration of consciousness;
I - correction of organ dysfunction.
In this manual, we will examine in detail only the first stage of resuscitation measures (A, B, C), leaving the remaining stages and stages for detailed study in subsequent courses.
So, stage A is the restoration of airway patency. When emergency conditions occur, the patency of the airways is often impaired due to the retraction of the tongue, which covers the entrance to the larynx and air cannot enter the lungs. In addition, in an unconscious patient there is always a danger of aspiration and blockage of the respiratory tract by foreign bodies and vomit.
To restore airway patency, it is necessary to perform a “triple airway maneuver”:
1) throwing back (hyperextension) of the head,
2) moving the lower jaw forward,
3) opening the mouth. To do this, with the II-V fingers of both hands, grab the ascending branch of the patient’s lower jaw near the auricle and push it forward (up) with force, shifting the lower jaw so that the lower teeth protrude in front of the upper teeth. During this manipulation, the anterior muscles of the neck are stretched, due to which the root of the tongue is raised above the back wall of the pharynx.
If the airways are obstructed by a foreign body, the victim should be placed in a lying position on his side and 3-5 sharp blows should be given with the lower part of the palm in the interscapular area. The oropharynx is cleaned with a finger, trying to remove the foreign body, then artificial respiration is attempted. If there is no effect, an attempt is made to restore the airways using the Greimlich maneuver - forced pressure on the abdomen. In this case, the palm of one hand is applied to the stomach in the midline between the navel and the xiphoid process. The second hand is placed on top of the first and presses on the stomach with quick movements up the midline. After ensuring airway patency, the next stage of resuscitation begins.
Stage B - artificial respiration. Artificial respiration is the injection of air or an oxygen-enriched mixture into the patient’s lungs, performed without or with the use of special devices, that is, temporary replacement of the function of external respiration. The air exhaled by a person contains from 16 to 18% oxygen, which allows it to be used for artificial respiration during resuscitation. It should be noted that in patients with respiratory and cardiac arrest, pulmonary tissue collapses, which is greatly facilitated by chest compressions. Therefore, it is necessary to provide adequate ventilation during cardiac massage. Each insufflation should take 1-2 seconds, since with a longer forced insufflation, air may enter the stomach. Insufflation must be done sharply and until the patient’s chest begins to rise noticeably. In this case, the victim exhales passively, due to the increased pressure created in the lungs, their elasticity and the mass of the chest. Passive exhalation should be complete. The respiratory rate should be 12-16 per minute. The adequacy of artificial respiration is assessed by periodic expansion of the chest and passive exhalation of air.
Technically, artificial ventilation of the lungs can be carried out by artificial respiration “mouth to mouth”, “mouth to nose”, artificial respiration through an S-shaped air duct and with the help of a mask and an Ambu bag. The most accessible and common method in prehospital intensive care is the simple method of mouth-to-mouth artificial respiration (Fig. 49 d, e, f). To do this, you need to pinch the patient’s nose with one hand, take a deep breath, press your lips tightly around the patient’s mouth (to the lips and nose of newborns and infants) and blow in air until the chest rises to the maximum. While blowing air, monitor the patient’s chest; it should rise when air is blown in. If the patient's chest rises, it is necessary to stop insufflation, lower the patient's mouth and turn his face to the side, giving the victim the opportunity to make a full passive exhalation; when the exhalation ends, take the next deep breath. First, two inflations of the lungs are made, each lasting 1-2 seconds. Then the pulse in the carotid artery is determined; if there is a pulse, repeat the inflation of the lungs - in adults there is approximately one inflation every 5 seconds (12 per minute); for children - one every 4 seconds (15 per minute); in infants - every 3 seconds (20 per minute) - until adequate spontaneous breathing is restored. Artificial respiration is performed at a frequency of 10-12 times per minute (once every 5-6 seconds).
Auxiliary ventilation is used against the background of preserved independent but inadequate breathing in the patient. Simultaneously with the patient's inhalation, additional air is injected through 1-3 respiratory movements. The inhalation should be smooth and correspond in time to the patient’s inhalation. It should be noted that restoring spontaneous breathing quickly restores all other functions. This is due to the fact that the respiratory center is the pacemaker for the brain.
Stage C – maintaining blood circulation. After circulatory arrest for 20–30 minutes, the heart’s automaticity and conductivity functions are preserved, which makes it possible to restore its pumping function. Regardless of the mechanism of cardiac arrest, cardiopulmonary resuscitation must be started immediately to prevent the development of irreversible damage to body tissues (brain, liver, heart, etc.) and the onset of biological death. The main purpose of cardiac massage is to create artificial blood flow. It should be understood that cardiac output and blood flow created by external cardiac massage are no more than 30% of normal and only 5% of normal cerebral blood flow. But, as a rule, this is enough to maintain the viability of the central nervous system during cardiopulmonary and cerebral resuscitation, provided that sufficient oxygenation of the body is achieved within several tens of minutes. At the prehospital stage, only indirect, or closed, cardiac massage is used (i.e., without opening the chest). Sharp pressure on the sternum leads to compression of the heart between the spine and sternum, reducing its volume and ejecting blood into the aorta and pulmonary artery, i.e. it is an artificial systole. At the moment the pressure stops, the chest expands, the heart takes on a volume corresponding to diastole, and blood from the vena cava and pulmonary veins enters the atria and ventricles of the heart. The rhythmic alternation of compressions and relaxations to some extent replaces the work of the heart, i.e., one of the types of artificial circulation is performed. The technique of performing indirect cardiac massage is as follows. The patient is placed on a hard, flat horizontal surface on his back (Fig. 50). Carrying out chest compressions on an armored bed does not make sense - the patient must be laid on the floor. Conductive massage
is located on the side of the patient and places his palms (one on top of the other) on the lower third of the sternum above the base of the xiphoid process by 2 - 3 cm.
You should pay attention to the fact that not the entire palm is located on the sternum, but only its proximal part in close proximity to the wrist (Fig. 51). Indirect cardiac massage itself consists of rhythmic (80 per minute) pressure on the patient’s sternum. In this case, the sternum should drop by at least 5–6 cm.
You should pay attention to the fact that in order to perform a massage correctly, the arms should be almost completely straightened at the elbow joints and pressure on the sternum should be applied with the entire mass of the torso. Many guidelines recommend starting chest compressions with a single strong blow to the patient’s sternum, since fibrillation is often the cause of impaired myocardial contractility and a precordial blow can stop the arrhythmia.
The actual sequence of actions during cardiopulmonary resuscitation is as follows. Option I – resuscitation is carried out by one person:
- if the victim is unconscious, his head is thrown back as much as possible, supporting his chin so that his mouth is slightly open. If necessary, the lower jaw is advanced. If injury to the cervical spine is suspected, moderate head tilting is used only to maintain airway patency. Check for spontaneous breathing (listening and feeling the flow of air at the victim’s mouth, nose, observing the excursion of the chest);
- if the victim is not breathing, perform two deep inflations of the lungs (the chest should rise). Each inflation is performed relatively slowly for 1-2 seconds, then pause to allow a complete passive exhalation;
- palpate the pulse in the carotid artery (5-10s). If a pulse is present, continue ventilation at a rate of about 12 inflations per minute in adults (one inflation every 5 seconds), 15 inflations per minute in children (about 4 seconds) and 20 inflations per minute (one every 3 seconds) in infants;
- if there is no pulse, begin chest compressions;
- carry out 15 compressions of the sternum with a frequency of 80-100 per 1 min. After 15 compressions, two inflations of the lungs are made and continue to alternate 15 compressions on the sternum with two inflations of the lungs;
- the sternum is pressed to the spine by approximately 4-5 cm in adults, 2.5-4 cm in young children and 1-2 cm in infants. The recovery of spontaneous pulse is checked every 1-3 minutes.
Option II – resuscitation is carried out by two people:
Those resuscitating should be on opposite sides of the victim to make it easier to change roles without interrupting resuscitation.
- if the victim is unconscious, the resuscitator (performing ventilation) tilts his head back;
- if the victim is not breathing, the first resuscitator performs two deep lung inflations;
- checks the pulse in the carotid artery;
- if there is no pulse, the second resuscitator begins compression of the sternum with a frequency of 80-100 per minute, the first resuscitator performing ventilation performs one deep inflation of the lungs after every 5 compressions of the sternum; while the lungs are being inflated, the second resuscitator makes a short pause;
- then continue alternating 5 pressures on the sternum with one inflation of the lungs until an independent pulse appears.
Signs of the effectiveness of the massage are the narrowing of previously dilated pupils, the disappearance of pallor and a decrease in cyanosis, pulsation of large arteries (primarily the carotid) in accordance with the frequency of the massage, and the appearance of independent respiratory movements. Indirect cardiac massage is not stopped for more than 5 seconds; it should be carried out until spontaneous heart contractions are restored, ensuring sufficient blood circulation. An indicator of this will be the pulse detected in the radial arteries and an increase in systolic blood pressure to 80-90 mm. Hg Art. The absence of independent heart activity with undoubted signs of the effectiveness of the massage is an indication for continued resuscitation. Carrying out a cardiac massage requires sufficient endurance; It is desirable to change the massager every 5-7 minutes, carried out quickly, without disturbing the rhythm of the heart massage.