What is damaged by heart defects? Brief anatomical information
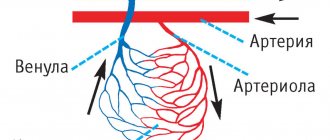
The human heart is four-chambered (two atria and ventricles, left and right). The aorta, the largest blood artery in the body, originates from the left ventricle; the pulmonary artery emerges from the right ventricle.
Between the various chambers of the heart, as well as at the initial sections of the vessels extending from it, there are valves - derivatives of the mucous membrane. Between the left chambers of the heart is the mitral (bicuspid) valve, and between the right chambers is the tricuspid (three-leaf) valve. At the exit to the aorta there is the aortic valve, at the beginning of the pulmonary artery there is the pulmonary valve.
The valves increase the efficiency of the heart - they prevent the backflow of blood during diastole (relaxation of the heart after its contraction). When the valves are damaged by a pathological process, the normal function of the heart is disrupted to one degree or another.
Heart defects include valve insufficiency (the valves do not close completely, causing blood to flow back), stenosis (narrowing), or a combination of these two conditions. Isolated damage to one valve or a combination of various defects is possible.
Multichamber structure of the heart and its valves
Prevention
Prevention of PPS involves treating the underlying disease that caused the valve damage. To prevent the development of defects, a cardiotrophic diet and lifestyle correction are additionally prescribed:
- refusal of salty, spicy, fatty foods;
- complete cessation of smoking and drinking alcohol;
- moderately active lifestyle;
- control of infectious diseases, including colds;
- annual monitoring by a cardiologist.
All prescriptions and dietary adjustments must be prescribed by your doctor during the treatment process. In our center, the Federal Scientific and Clinical Center of the Federal Medical and Biological Agency, several programs have been developed that will help identify whether you have a heart defect and determine the method of its treatment. You can learn more about the programs here.
Classification of valve problems
There are several criteria for classifying heart defects. Below are some of them.
According to the causes of occurrence (etiological factor), defects are distinguished:
- rheumatic (in patients with rheumatoid arthritis and other diseases of this group, these pathologies cause almost all acquired heart defects in children and most of them in adults);
- atherosclerotic (valve deformation due to the atherosclerotic process in adults);
- syphilitic;
- after endocarditis (inflammation of the inner lining of the heart, the derivatives of which are the valves).
According to the degree of hemodynamic disturbance (circulatory function) inside the heart:
- with minor hemodynamic impairment;
- with moderate impairments;
- with severe impairments.
By disturbance of general hemodynamics (on the scale of the whole organism):
- compensated;
- subcompensated;
- decompensated.
According to the location of the valvular lesion:
- monovalve – with isolated damage to the mitral, tricuspid or aortic valve;
- combined - a combination of damage to several valves (two or more), possible mitral-tricuspid, aortic-mitral, mitral-aortic, aortic-tricuspid defects;
- three-valve - involving three structures at once - mitral-aortic-tricuspid and aortic-mitral-tricuspid.
According to the form of functional impairment:
- simple – stenosis or insufficiency;
- combined – stenosis and insufficiency on several valves at once;
- combined – insufficiency and stenosis on one valve.
Diagram of the structure and operation of the aortic valve
Aortic pathology
Aortic defects are diagnosed in 20% of all cases. Aortic valve insufficiency often causes arterial hypertension.
Combined aortic heart disease affects the aorta directly and is combined with insufficient valve function.
This type of illness is characterized by upper and lower noises, the pulse is weakened, and a decrease in upper pressure is noted. The disease is accompanied by shortness of breath due to congestion in the lungs.
Aortic valve disease most often begins due to infectious diseases. Rheumatism extremely rarely causes pathology of this kind.
The mechanism of heart defects
Under the influence of a pathological process (caused by rheumatism, atherosclerosis, syphilitic lesions or trauma), the structure of the valves is disrupted.
If fusion of the leaflets or their pathological stiffness (rigidity) occurs, stenosis develops.
Cicatricial deformation of the valve leaflets, wrinkling or complete destruction causes their insufficiency.
As stenosis develops, resistance to blood flow increases due to mechanical obstruction. If the valve fails, some of the pushed-out blood flows back, forcing the corresponding chamber (the ventricle or atrium) to do extra work. This leads to compensatory hypertrophy (increase in volume and thickening of the muscle wall) of the heart chamber.
Gradually, in the hypertrophied part of the heart, dystrophic processes and metabolic disorders develop, leading to a decrease in performance and, ultimately, to heart failure.
Infectious and prosthetic endocarditis.
The etiology of infective endocarditis has changed significantly due to the active use of antibiotics throughout the world. Currently, the main role is given to staphylococci and gram-negative flora, as well as fungal infections.
From the point of view of surgery, in the pathogenesis of infective endocarditis, the fact of rapid destruction of the valvular apparatus of the heart is of greatest importance. This leads to a catastrophic increase in heart failure, since the myocardium does not have time to adapt to the sudden disruption of hemodynamics. The decision on the need for surgical treatment arises, as a rule, with the development of “complicated infective endocarditis”: changes in hemodynamic status; persistence and prevalence of infection; development of metastatic foci of infection; systemic embolisms. In these cases, surgical treatment is more successful than a therapeutic approach. The main problem of surgical treatment is to prevent recurrence of infection and the development of prosthetic endocarditis. The basis for the choice of tactics is the anatomical changes identified on the operating table: the degree of damage to the fibrous ring and surrounding tissues, as well as the presence of vegetations, abscesses, fistulas, and prosthetic separations. In recent years, particular importance has been given to reconstructive operations, especially when the mitral or tricuspid valves are affected by endocarditis. To replace valve defects after surgical treatment, plastic surgery with one’s own tissue, auto- or xenopericardium is used.
The most common heart defects
Mitral stenosis
Narrowing of the communication between the left chambers of the heart (atrioventricular orifice) is usually a consequence of a rheumatic process or infective endocarditis, causing fusion and hardening of the valve leaflets.
The defect may not manifest itself for a long time (remain in the compensation stage) due to the growth of muscle mass (hypertrophy) of the left atrium. When decompensation develops, blood stagnates in the pulmonary circulation - the lungs, the blood from which is obstructed when entering the left atrium.
Symptoms
If the disease occurs in childhood, the child may lag behind in physical and mental development. Characteristic of this defect is a “butterfly” blush with a bluish tint. The enlarged left atrium compresses the left subclavian artery, so a pulse difference appears in the right and left arms (less filling on the left).
Left ventricular hypertrophy with mitral stenosis (radiography)
Mitral regurgitation
In case of mitral valve insufficiency, it is not able to completely block the communication of the left ventricle with the atrium during heart contraction (systole). Some of the blood returns back to the left atrium.
Given the large compensatory capabilities of the left ventricle, external signs of failure begin to appear only with the development of decompensation. Gradually, congestion in the vascular system begins to increase.
The patient is worried about palpitations, shortness of breath, decreased exercise tolerance, and weakness. Then swelling of the soft tissues of the extremities occurs, enlargement of the liver and spleen due to stagnation of blood, the skin begins to acquire a bluish tint, and the neck veins swell.
Tricuspid insufficiency
Insufficiency of the right atrioventricular valve is very rare in isolated form and is usually part of combined heart defects.
Since the vena cavae flow into the right heart chambers, collecting blood from all parts of the body, venous stasis develops with tricuspid insufficiency. The liver and spleen enlarge due to overflow with venous blood, fluid collects in the abdominal cavity (ascites occurs), and venous pressure increases.
The function of many internal organs may be impaired. Constant venous congestion in the liver leads to the growth of connective tissue in it - venous fibrosis and a decrease in the activity of the organ.
Tricuspid stenosis
Narrowing of the opening between the right atrium and the ventricle is also almost always a component of combined heart defects, and only in very rare cases can it be an independent pathology.
For a long time there are no complaints, then atrial fibrillation and congestive heart failure quickly develop. Thrombotic complications may occur. Externally, acrocyanosis (blueness of the lips, nails) and a jaundiced tint of the skin are determined.
Aortic stenosis
Aortic stenosis (or aortic stenosis) serves as an obstruction to blood flowing from the left ventricle. There is a decrease in the release of blood into the arterial system, from which, first of all, the heart itself suffers, since the coronary arteries feeding it depart from the initial part of the aorta.
Deterioration of blood supply to the heart muscle causes attacks of chest pain (angina). A decrease in cerebral blood supply leads to neurological symptoms - headaches, dizziness, periodic loss of consciousness.
Decreased cardiac output is manifested by low blood pressure and weak pulse.
Schematic representation of aortic stenosis
Aortic insufficiency
When the aortic valve, which normally should block the exit from the aorta, is insufficient, some of the blood returns back to the left ventricle during its relaxation.
As with some other defects, due to compensatory hypertrophy of the left ventricle, heart function remains at a sufficient level for a long time, so there are no complaints.
Gradually, due to a sharp increase in muscle mass, a relative discrepancy in blood supply arises, which remains at the “old” level and is unable to provide nutrition and oxygen to the enlarged left ventricle. Attacks of angina pain appear.
In the hypertrophied ventricle, dystrophic processes increase and cause a weakening of its contractile function. Blood stagnation occurs in the lungs, which leads to shortness of breath. Insufficient cardiac output causes headaches, dizziness, loss of consciousness when taking an upright position, and pale skin with a bluish tint.
Aortic insufficiency (diagram)
This defect is characterized by a sharp change in pressure in different phases of the heart, which leads to the appearance of the “pulsating man” phenomenon: constriction and dilation of the pupils in time with the pulsation, rhythmic shaking of the head and changes in the color of the nails when pressing on them, etc.
Combined and associated acquired defects
The most common combined defect is a combination of mitral stenosis with mitral insufficiency (usually one of the defects predominates). The condition is characterized by early shortness of breath and cyanosis (bluish discoloration of the skin). Combined aortic disease (when narrowing and insufficiency of the aortic valve coexist) combines the signs of both conditions in an unexpressed, mild form.
conclusions
Combined and associated defects are complex cardiac pathologies that require certain skills for timely diagnosis and initiation of treatment. Clinical signs of damage to a valve (or several) with two mechanisms of circulatory disorders occur latently, so most often doctors diagnose some kind of isolated defect. The use of an integrated approach and modern methods allows us to establish a reliable diagnosis and send the patient for surgery before irreversible changes occur in other organs.
Diagnostics
A comprehensive examination of the patient is carried out:
- When interviewing the patient, past illnesses (rheumatism, sepsis), attacks of chest pain, and poor tolerance to physical activity are revealed.
- Examination reveals shortness of breath, pale skin with a bluish tint, swelling, and pulsation of visible veins.
- An ECG reveals signs of rhythm and conduction disturbances, phonocardiography reveals a variety of murmurs during heart function.
- X-ray is determined by hypertrophy of one or another part of the heart.
- Laboratory methods are of auxiliary value. Rheumatoid tests may be positive, cholesterol and lipid fractions may be elevated.
Treatment methods for acquired heart defects
Elimination of pathological changes in the heart valves caused by a defect can only be achieved through surgery. Conservative treatment serves as an additional means to reduce the manifestations of the disease.
Acquired heart defects must be operated on in a timely manner, before the development of heart failure. The timing and extent of surgical intervention is determined by the cardiac surgeon.
Main types of operations for heart defects:
- In case of mitral stenosis, the welded valve leaflets are separated with simultaneous expansion of its opening (mitral commissurotomy).
- In case of mitral insufficiency, the incompetent valve is replaced with an artificial one (mitral replacement).
- For aortic defects, similar operations are performed.
- In case of combined and combined defects, replacement of damaged valves is usually performed.
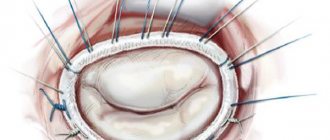
Implantation of artificial mitral valve
The prognosis for timely surgery is favorable . If there is a detailed picture of heart failure, the effectiveness of surgical correction in terms of improving the condition and prolonging life is sharply reduced, so timely treatment of acquired heart defects is very important.